Chapter 153 Circumscribed Choroidal Hemangioma
Introduction
Choroidal hemangiomas are benign vascular hamartomas which occur in two forms: circumscribed and diffuse. The circumscribed form is typically an isolated finding without systemic associations, while the diffuse form generally occurs in association with Sturge–Weber syndrome (discussed separately in Chapter 132, Phakomatoses). There have been rare reports of circumscribed choroidal hemangioma in patients with Sturge–Weber syndrome.1,2 The first histologically confirmed case of choroidal hemangioma was published by Leber in 1868.3 The incidence of the disease is difficult to estimate since most circumscribed choroidal hemangiomas only come to medical attention if patients become symptomatic or if they are discovered incidentally during routine examination; however, the disease is felt to be relatively rare, with five cases discovered upon histological examination of 4500 enucleated eyes.4 More than 90% of reported cases have been in Caucasian patients (though there have been published cases in black, Hispanic, and Asian patients), with a relatively even distribution between males and females.5,6 The mean age at diagnosis in the two largest case series ranged from 38.7 years to 47 years, considerably older than the mean age at diagnosis for diffuse choroidal hemangioma, which is typically in the first decade of life.5,6
Clinical features
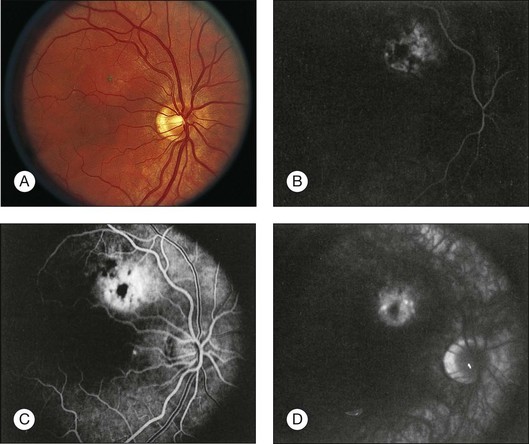
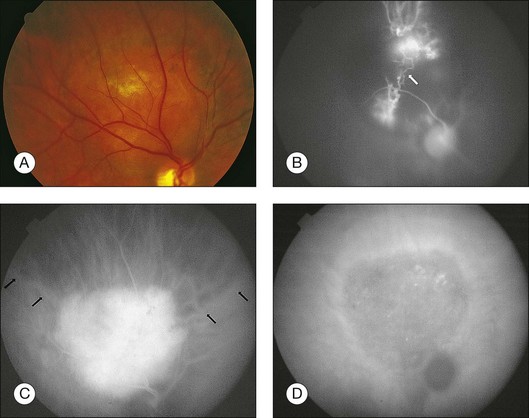
Circumscribed choroidal hemangiomas are generally orange-red elevated masses, which are found posterior to the equator (Figs 153.1–153.4). The color of the tumor has also been variably described as “salmon-colored”,7 “yellow-white”,8 and “grayish-pink”.6 Choroidal elevation may be difficult to discern on color photographs, and may be more apparent on clinical examination. Pigmentary changes have also been reported on the surface of the tumor or as a ring of pigmentation around the edge of the tumor.6 There may be accumulation of lipofuscin pigment (orange pigment) over the lesion, though this is often difficult to distinguish except with fluorescein angiography.9 In the largest published series of 200 patients by Shields et al., 67% of tumors were in the macula, 34% were between the macula and the equator, and no tumors were anterior to the equator.5 In the second-largest series of 45 patients with circumscribed choroidal hemangioma reported by Witschel and Font, all of the circumscribed tumors were located posterior to the equator.6 In the Shields series, the mean tumor diameter was 6.7 mm, and the mean tumor thickness was 3.1 mm.5 Lesions are usually solitary and unilateral, though bilateral choroidal hemangiomas have been reported.7 Overlying subretinal fluid or serous retinal detachment is a common finding, present in 47% of patients in the Witschel series,6 and 81% of the patients in the Shields series (Fig. 153.3).5 Cystoid macular edema is also a common finding, present in up to 17% of patients, and exudates, epiretinal membrane, and retinal hemorrhages have also been reported.5 Exudates are uncommon in melanocytic lesions. Choroidal neovascularization is rare but has been reported in four patients.5,10 Retinal neovascularization has also been reported in three eyes with circumscribed choroidal hemangioma.11 Patients with total retinal detachments can also develop neovascularization of the iris and angle and neovascular glaucoma.5
These lesions usually remain stationary in size, though there have been reports of gradual progressive enlargement.12,13 In five cases, there was only slight enlargement with a mean of 1.6 × 1.5 mm in basal diameter and 0.9 mm in thickness over an average of 52 months of follow-up.12 In another case with significant enlargement, the eye was enucleated due to concern for choroidal melanoma and pathologic examination revealed that the increase in size was most likely due to vascular congestion of the tumor vessels, and possibly an increase in the caliber and number of tumor vessels.13 There has also been one report of “blackening” of a circumscribed choroidal hemangioma from red-orange to dark gray after tantalum clip placement in preparation for external proton beam irradiation.14 The hemangioma subsequently returned to its original red-orange color 2 weeks after surgery (prior to proton beam irradiation), leading the authors to hypothesize that the transient color change may have been due to extravascular hemorrhage from surgical manipulation.14 Bosch and Helbig also reported blackening of a choroidal hemangioma after photodynamic therapy.15
The most commonly reported symptom is blurred vision in up to 81% of patients, though patients also note visual field deficits, metamorphopsia, and floaters.5 Presenting visual acuity ranged from 20/20–20/40 in 24% of eyes to 20/400 or worse in 34% of eyes in the Shields series, and 60% of eyes were “blind” in the Witschel series.5,6
Differential diagnosis
The differential diagnosis of circumscribed choroidal hemangioma includes choroidal nevus, amelanotic choroidal melanoma, choroidal metastasis, choroidal osteoma, and central serous chorioretinopathy. On clinical examination, choroidal hemangiomas have a characteristic orange-red color, unlike choroidal metastases which tend to be creamy-yellow and amelanotic melanomas which tend to be more yellow-tan.5 Ancillary testing is very helpful to distinguish these conditions. Ultrasonography shows high internal reflectivity due to the vascular component of the lesion, in contrast to choroidal melanomas which display low to medium internal reflectivity. Circumscribed choroidal hemangiomas also have a very distinct appearance on indocyanine green angiography with rapid filling and “washout” phenomenon, unlike choroidal melanoma and metastasis which have slower and less intense filling.5 On MRI, circumscribed choroidal hemangiomas show bright signal on both T1- and T2-weighted images, whereas choroidal melanomas and metastases show bright signal on T1-weighted images but low signal on T2-weighted images.5
Ancillary studies
Intravenous fluorescein angiography
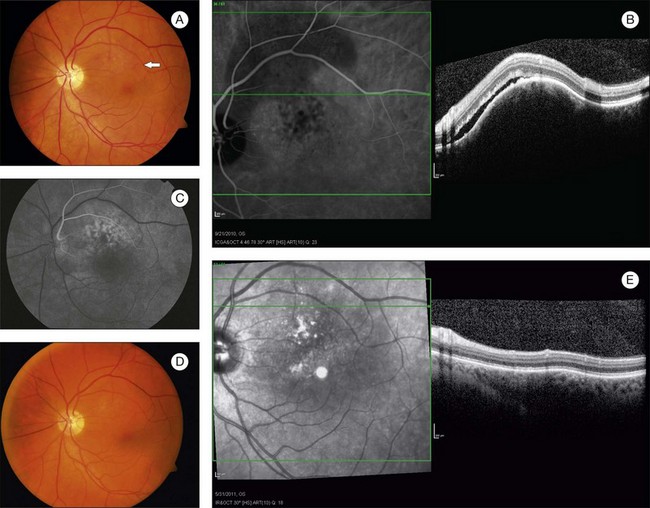
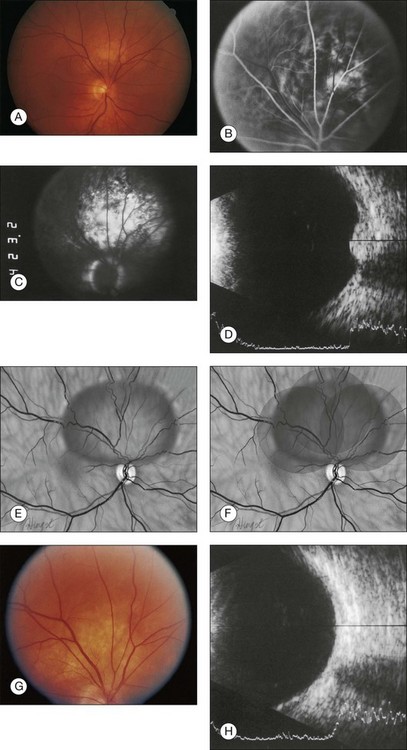
Fluorescein angiography (FA) of circumscribed choroidal hemangiomas generally reveals mild early lacy hyperfluorescence of the tumor in the pre-arterial and arterial phase, followed by moderate hyperfluorescence during the arteriovenous phase, and increasing hyperfluorescence through the late phase with variable amounts of late leakage (Figs 153.1, 153.3, 153.4).5,16,17 The FA pattern of choroidal hemangioma can be somewhat variable and similar to other amelanotic choroidal tumors, hence FA may not be diagnostic in the absence of other ancillary testing.18 FA can also be helpful for visualization of associated subretinal fluid and cystoid macular edema, which are not typically seen on indocyanine green angiography.18
Indocyanine green angiography
Indocyanine green angiography (ICGA) is particularly helpful in the diagnosis of circumscribed choroidal hemangioma since it provides better visualization of the choroidal vasculature. Circumscribed choroidal hemangiomas have a characteristic pattern of rapid onset of fluorescence around 30 s which occurs much earlier than in other choroidal tumors.18–20 The fluorescence occurs in a lacy diffuse hyperintense pattern which fills first peripherally then centrally.19 In the late frames, the tumor demonstrates loss of dye resulting in a hypofluorescent appearance compared with the surrounding choroid, which is known as the “wash out” phenomenon (Fig. 153.2).18–20 In addition, a late hyperfluorescent rim around the tumor is almost always present.18–20 Intrinsic tumor vessels are more likely to be seen with ICG than with FA, and the normal choroidal vasculature beneath the tumor is obscured, a feature which is also considered pathognomonic.18,20 Chronic lesions with significant retinal pigment epithelial changes may have blocked fluorescence on ICGA.
Ultrasonography
Circumscribed choroidal hemangiomas have a consistent characteristic appearance on ultrasonography. On B-scan ultrasonography, the hemangioma appears as an acoustically solid mass, which is almost always identical in character to the surrounding normal choroid (Fig. 153.4).5,17 The tumor is typically dome-shaped but can occasionally appear mushroom-shaped or plateau-shaped.5 On A-scan, the choroidal hemangioma demonstrates high internal reflectivity.5,17 Both of these features are useful to distinguish choroidal hemangioma from choroidal melanoma which is usually acoustically hollow with medium to low internal reflectivity.5
Neuroimaging
Magnetic resonance imaging (MRI) of choroidal hemangiomas typically shows hyperintensity in contrast to vitreous on T1-weighted images, and hyperintensity or isointensity to vitreous on T2-weighted images.5 Choroidal hemangiomas show enhancement with gadolinium contrast.5 The MRI findings are helpful for differentiation from choroidal melanoma and metastasis which show bright signal on T1-weighted images and low signal on T2-weighted images.5
Optical coherence tomography and enhanced depth imaging
In choroidal tumors, traditional time-domain and spectral-domain optical coherence tomography (SD-OCT) are most useful for visualizing secondary changes to the retina and retinal pigment epithelium (RPE).21 In choroidal hemangiomas, OCT can be used to demonstrate macular edema, epiretinal membranes, and subretinal fluid (Fig. 153.3). Until recently, wavelength-dependent light scattering and decreasing sensitivity and resolution with increased displacement from zero delay prevented detailed imaging of the choroid and sclera with OCT.22 Spaide and colleagues described a method of placing the SD-OCT closer to the patient to purposefully image deeper layers, producing a detailed inverted image of the choroid.22 Torres et al. have used this enhanced depth imaging (EDI) technique to look at a variety of choroidal tumors, including three circumscribed choroidal hemangiomas.23 Circumscribed choroidal hemangiomas in this series showed low to medium homogeneous reflectivity with intrinsic spaces.23
Autofluorescence
Fundus autofluorescence (AF) is an imaging technique which visualizes lipofuscin distribution in the RPE cell monolayer.24 AF is increased in dysfunctional RPE and decreased in areas of photoreceptor loss, and has been useful in age-related macular degeneration (AMD), Best disease, and various chorioretinal inflammatory disorders.24 A study of AF in 34 eyes with choroidal hemangiomas (27 of which were circumscribed) found that the intrinsic tumor AF of untreated circumscribed choroidal hemangiomas was either iso-autofluorescent (58%) or hypo-autofluorescent (42%), and treated circumscribed choroidal hemangiomas were all hypo-autofluorescent (100%).25 The extrinsic AF of the overlying retinal pigment epithelium and retinal alterations showed hyper-autofluorescence of orange pigment in two cases of untreated circumscribed choroidal hemangioma, and hypo-autofluorescence of RPE hyperplasia, atrophy, and fibrous metaplasia.25
Pathology
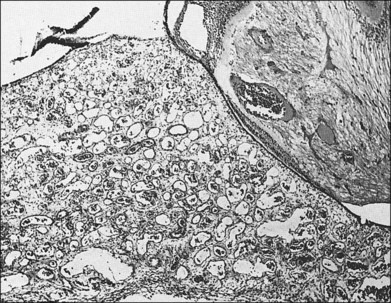
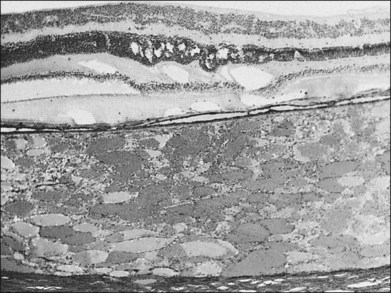
Choroidal hemangiomas are hamartomas, benign vascular tumors which are composed of tissue elements normally found in a given location. Hemangiomas of the choroid are classified histopathologically according to the prevailing type or types of vessels within the tumor: capillary, cavernous, or mixed.6 The capillary type is composed of small vessels separated by loose connective tissue (Fig. 153.5), whereas the cavernous type is composed of larger vessels separated by relatively little connective tissue (Fig. 153.6). The mixed type shows both capillary and cavernous features. Choroidal hemangiomas are notable for the lack of cellular proliferation of the elements of the vessel walls, supporting the idea that these tumors are nonproliferative lesions.6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


