Chapter 36 Childhood cataracts
Incidence
Cataracts, which are opacities of the crystalline lens, are an important problem in children worldwide. The incidence varies, but in the UK the adjusted cumulative incidence at age 1 year is 2.49/10 000, increasing to 3.46/10 000 by age 15 years.1 Bilateral cataracts are more common than unilateral.
Detection
Children with visually significant unilateral cataracts often present with strabismus and dense amblyopia. However, visual behavior will usually be unaffected by a unilateral cataract, and for this reason the parents may not be aware of it. In contrast, dense bilateral cataracts are usually associated with impaired visual behavior. If nystagmus develops, visual prognosis is worse, although it may be reversed by prompt treatment.2
Morphology
The morphology of cataracts offers important clues to their age of onset and visual prognosis. In addition, it provides insights into the etiology of a cataract. When possible, a slit-lamp examination is invaluable in identifying the morphology. Refinements in the morphology can be obtained intraoperatively.3 The morphology is largely determined by the anatomy of the lens, its embryology, and the timing and nature of the insult that caused it (Box 36.1).
Box 36.1
Morphological classification of infantile cataract
Fetal nuclear Opaque lens material between anterior and posterior “Y” suture that may spread into the surrounding (especially posterior) cortex and often associated with posterior capsule plaque
Cortical Anterior and/or posterior cortical opacity not involving the fetal nucleus and often associated with posterior capsule plaque
Persistent fetal vasculature A combination of one or more of the following: retrolental membrane with or without visible vessels, patent or non-patent persistent hyaloid vessel, or stretched ciliary processes
Isolated posterior capsule plaque (posterior polar) Opacity of the posterior capsule without overlying opacity in the cortex or nucleus
Posterior lentiglobus Posterior bowing of the posterior capsule with or without a pre-existing posterior capsule defect
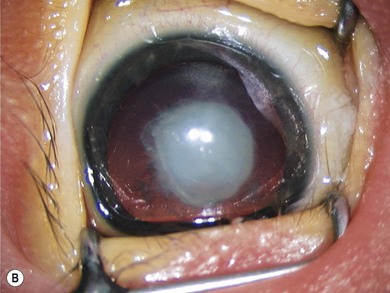
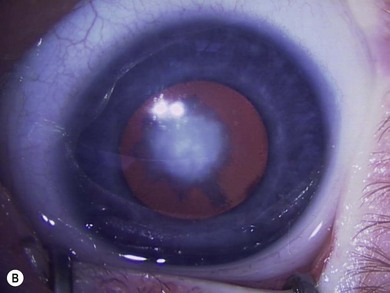
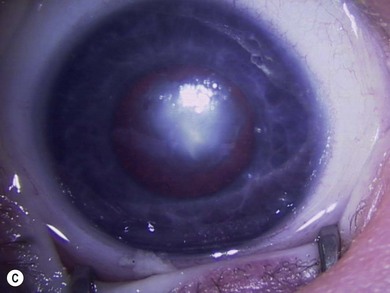
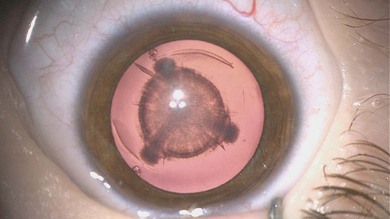
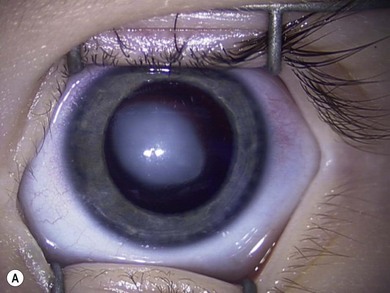
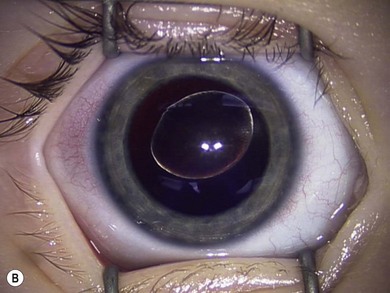
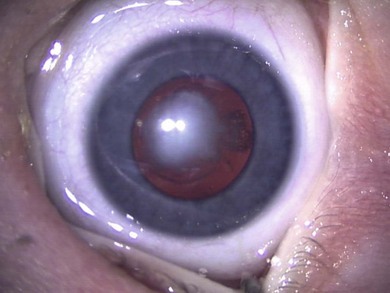
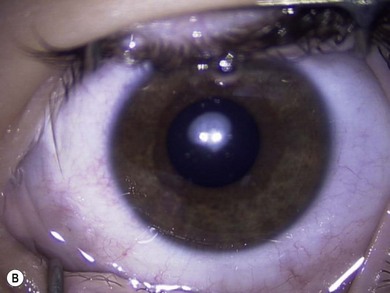
Some morphological types of cataracts have a better prognosis than others. Anterior polar (Fig. 36.1), lamellar (Fig. 36.2), sutural (Fig. 36.3), and posterior lentiglobus (Fig. 36.4) cataracts are associated with the best visual prognoses, whereas dense, central, and posterior cataracts have poorer visual prognoses.4 Acquired cataracts generally have a more favorable visual prognosis than congenital cataracts.


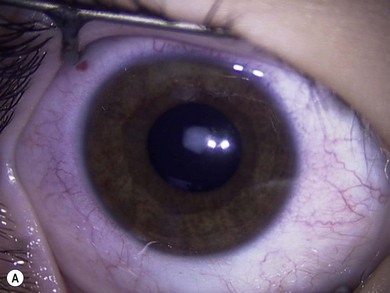
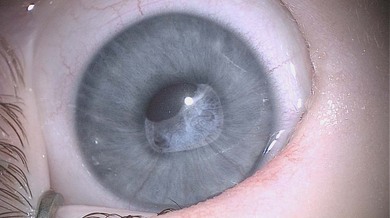
Certain types of cataracts are frequently associated with other ocular abnormalities. For instance, nuclear cataracts are often associated with microphthalmos (Fig. 36.5) while autosomal dominant anterior polar cataracts (Fig. 36.6) are more commonly associated with corneal guttata or astigmatism. Anterior subcapsular and anterior capsular cataracts are often associated with severe skin diseases (syndermatotic cataract). Partially reabsorbed cataracts in an infant boy are suggestive of Lowe’s syndrome or Hallermann-Streiff syndrome. Wedge-shaped or sectional cataracts may occur with Stickler’s syndrome and Conradi’s syndrome and may be due to lyonization.
Persistent fetal vasculature
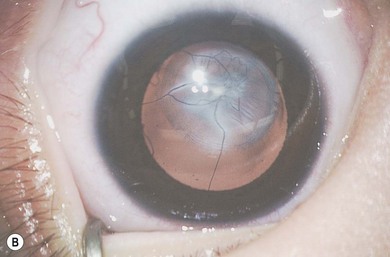
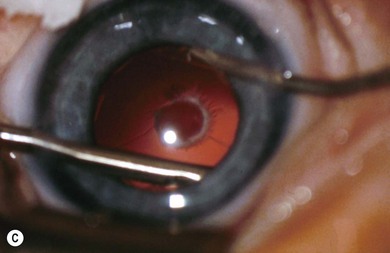
The term persistent fetal vasculature (PFV) describes a wide spectrum of congenital anomalies which commonly consist of a retrolental plaque (Fig. 36.7) in a microphthalmic eye with prominent blood vessels on the iris, a shallow anterior chamber, elongated ciliary processes, and occasionally intralenticular hemorrhages.5 Less commonly, these patients may present with a vascularized pupillary membrane, microcoria, and an anterior capsular cataract (Fig. 36.8).6 PFV is unilateral in 90% of patients. Although the lens may be clear initially, over time they usually become cataractous. The lens may undergo spontaneous absorption. In others, it becomes swollen, with loss of the anterior chamber and glaucoma. The fibrovascular plaque may bleed if cut. The retrolental plaque may contract with traction on the vitreous base and peripheral retina. Usually the posterior pole is normal, but fibrous tissue from the hyaloid remnants may cause peripapillary tractional retinal detachment. Conditions that can mimic PFV include retinoblastoma, retinopathy of prematurity, retinal dysplasia, and posterior uveitis. The presence of microphthalmos, a shallow anterior chamber, elongated ciliary processes, a cataract, and a retrolental opacity with a persistent hyaloid artery are all helpful in distinguishing PFV from these conditions.


Etiology
Bilateral
An etiology can be established in about 50% of children with bilateral congenital cataracts. The most common etiology in Europe and the US are autosomal dominantly inherited cataracts. Less frequently, cataracts can be associated with trisomy 21 (Fig. 36.9), Lowe’s syndrome (Fig 36.10) and Hallerman-Streiff-Francois syndrome (Fig. 36.11) (Box 36.2). Congenital rubella syndrome is a cause of cataracts where rubella immunization rates are low.7