Chapter 146 Charged-Particle Irradiation of Uveal Melanoma
Introduction
Radiotherapy is currently the most widely used method for treating intraocular melanomas, having replaced enucleation as the standard of care for most tumors. It offers the advantage of eye salvage and retention of vision in many cases, although a survival advantage has not been demonstrated.1
There are two major radiotherapeutic techniques for the treatment of uveal melanomas: radioactive plaques2,3 sutured on the sclera over the area of the tumor, and external beam irradiation using charged particles such as protons,4 helium ions5 and the gamma knife.6,7 The advantages of charged-particle irradiation are based on the physical characteristics of particles, which make possible highly localized dose distributions,8–10 and provide highly attractive depth-dose distribution patterns.11 Although effective, helium ion irradiation5 is no longer in use due to its high cost. The dose distributions achieved with stereotactic radiosurgery using the gamma knife6,7 do not appear to be as attractive as those of proton irradiation.7 Additional experience and long-term follow-up are necessary to better evaluate its efficacy as most published studies to date have reported short-term results in small groups of patients.
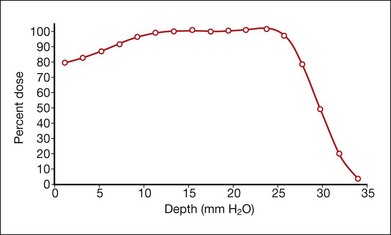
Protons are positive, singly charged particles that have minimal scatter and a well-defined, finite, and energy-dependent tissue range. Proton beams can be collimated to deliver maximum density of ionization in a sharply focused, localized volume because of the inherent Bragg peak at the end of the beam path. The Bragg peak can be broadened to cover a tumor at any depth (Fig. 146.1). The uniform dose of radiation delivered to the whole tumor and the sharp reduction of the dose outside the treated area allow tumors located near critical structures to be treated with the possibility of retaining visual acuity. Larger tumors can be treated because the overall irradiated volume is reduced. These properties should improve the therapeutic ratio of local control versus complications.
Early experimental work in monkey eyes, followed by clinical and histopathological studies in humans provide evidence of the advantageous properties of protons. The Bragg peak of small-diameter collimated beams positioned on the fundus by stereotactic radiography produced lesions confined to the intended radiation field.12 Normal retinal architecture as close as 1 mm from the edge of radiation-induced lesions was seen in irradiated monkey eyes more than 3.5 years after proton treatment.13 Similar data on humans substantiate the favorable effects obtained with protons. Using mathematical superimposition of fundus photographs, computer treatment plans, and visual fields, correlation between patterns of visual loss and radiation isodose calculations was established.14,15 Histologic examination of irradiated tumors revealed vessel thrombosis exclusively in retina overlying the tumor,16 and reduced or absent choroidal vasculature and RPE beneath and above the tumor but intact tissue adjacent to it.17
Treatment
Operative technique
The conjunctiva is incised, and the tumor is localized by transillumination, indirect ophthalmoscopy, or both. The episcleral tissues over the area of the tumor are examined carefully for evidence of extrascleral extension. The edges of the tumor are marked with a surgical marking pen, and four tantalum rings, 2.5 mm in diameter, are sutured to the sclera at the margins of the tumor. Ring to limbus distances and distances between the rings are measured. Highly elevated tumors can cast a variable shadow during transillumination, depending on the angle of illumination, which may result in an overestimate of the dimensions of the tumor. Therefore, the angle of illumination in the most precise shadow must be carefully chosen. For tumors that extend into the ciliary body and iris, rings are placed at the posterior margin of the tumor and accurate measurements are made of the distance from the rings to the anterior margin of the lesion. If tumors are in contact with the optic nerve, rings are placed only at the anterior and lateral margins of the lesion, and the distance from the rings to the posterior margin is estimated from fundus photographs. The tumor is transilluminated again after suturing of the rings (Fig. 146.2), the distances from the rings to the edges of the tumor are measured, and careful drawings of the tumor margins in relation to the rings are made. No operation is necessary for lesions confined to the ciliary body. The margins of the tumor in relation to anatomic landmarks of the iris and conjunctiva are defined by transillumination on the ocular surface.

Treatment planning
An interactive three-dimensional treatment planning computer program (EYEPLAN, Martin Sheen, Clatterbridge Centre for Oncology, Bebington, UK) facilitates the selection of the appropriate fixation angle, which is chosen to minimize irradiation of the lens, optic disc, and fovea.18 Such a program helps to select the best direction of gaze relative to the proton beam line; design the shape of the field-defining aperture; determine the proton range modulation necessary to encompass the target volume; determine the extent to which important structures are included within (or excluded from) the beam; and indicate the relative positions of the tumor-defining rings, beam aperture, and crosshairs that should be observed in the alignment film when the patient is correctly aligned. The treatment planning program creates a spherical model of a globe that is scaled to the ultrasonically determined length of the patient’s eye and the position of the tantalum rings previously sutured to the sclera, determined by orthogonal X-rays taken of the patient in the treatment position (gazing in three different directions). The structures of the eye are added to the model, including the anterior chamber depth and of the lens obtained ultrasonographically. The program then superimposes on this globe a three-dimensional model of the tumor based on fundus pictures and ultrasonograms. The fundus photographs are especially useful for very posterior tumors and tumors abutting the optic nerve where it is impossible to surround the tumor with marker rings. Two tumors can be created if needed, e.g., if there is a tumor with an irregular shape. Tumors in the iris or ciliary body, for which placement of marker rings is unnecessary, are drawn from clinical and ultrasound information.
The program automatically designs an aperture that gives a 3 mm margin around the tumor, at which the dose falls to 50%. This margin may be reduced to 2.5 mm for a tumor border at the limbus or increased to 4 mm for a patient without surgical markers. The program calculates the maximum and minimum depths of the tumor and allows the user to choose proximal and distal margins to give the needed beam range and modulation. The program calculates dose distributions on the fundus displayed in the geometry of a wide-angle fundus photograph (Fig. 146.3) and in any plane through the eye (Fig. 146.4). It also calculates dose–volume histograms for the tumor and many structures of the eye.
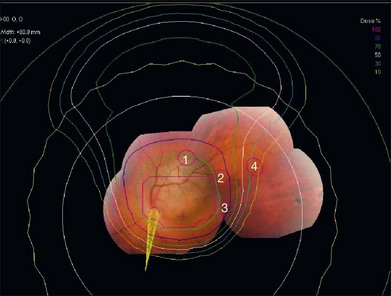
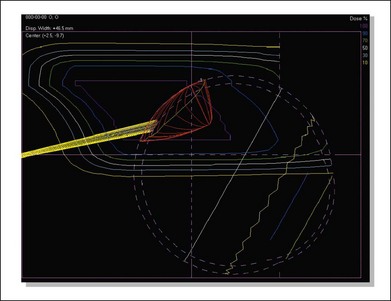
Fig. 146.4 Isodose curves in a vertical plane through the eye parallel to the beam direction for the case shown in Figure 146.3. The tumor is shown in red and the yellow cone represents the optic nerve. The innermost magenta line corresponds to the area receiving 100% of the dose (70 CGE) and the outermost yellow line corresponds to the area receiving 10% of the dose (7 CGE).
Treatment techniques
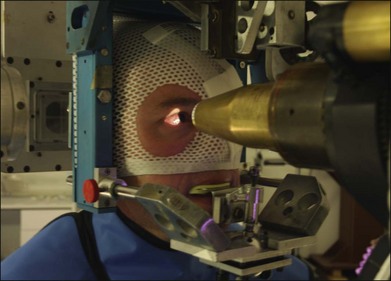
The patient is seated in a specially designed chair, and his or her head is immobilized with a bite-block made of a dental impression compound and fastened to the headholder. Individually contoured plastic masks mounted into a frame are also used for head fixation (Fig. 146.5). Orientation of the patient’s eye is established by voluntary fixation of the eye to be treated (the other eye is covered) on a small light that is attached to the collimator. If the vision is poor in the eye to be treated, the other eye can be used for fixation. The eyelids are held open with a lid speculum.
The eye is monitored using a high-magnification closed-circuit television system with its effective viewing point on the beam axis. This system provides a magnified image of 10 times the size of the patient’s eye and permits continuous monitoring of the eye’s position throughout the procedure. The alignment of the proton beam is achieved with orthogonal X-rays. The lesion, defined spatially by the radiopaque tantalum rings, can be positioned by translating the headholder until it is in the desired position relative to the beam axis. For tumors treated without surgical localization, a light beam coaxial with the central axis of the proton beam is used to position the tumor relative to the beam during treatment.8,19,20 Positioning is achieved with a fluoroscopic system that provides a virtually instantaneous picture held on an image-storage device. This system hastens alignment and assists in confirming eye immobilization during treatment. The alignment procedure lasts approximately 15 minutes. The patient is asked to fixate, and the eye’s position is observed on the television monitor in the control area. The treatment field is checked with a beam-simulation field light, and if the position and fixation are satisfactory, the treatment begins. If eye movement of more than 0.5 mm is observed, the treatment is halted immediately. Each treatment takes approximately 1–2 minutes, most without interruption.
Radiation dose
The standard dose administered for most tumors is 70 cobalt Gy equivalents (CGE) delivered in five equal fractions in 5 days (63.6 proton Gy times 1.1 relative biologic effectiveness equals 70 CGE). Dose fractionation increases the radiosensitivity of tumor tissue, as increased oxygenation of hypoxic tumor cells occurs between fractions. We selected large fractions based on favorable clinical results demonstrated with the use of a small number of relatively large dose fractions10,21 in patients with skin melanomas. At the prescribed dose of 70 CGE, we estimate that the optic nerve and macula receive the full dose when the tumor is less than 1 mm from these visual structures, half the dose (35 CGE) when the tumor is located 3 mm from these structures, and a small dose (≤15 CGE) when the tumor is peripheral (beyond 9 mm). As part of a randomized clinical trial to establish safety and efficacy of a dose reduction, 94 patients received a lower dose of 50 CGE.22 No significant differences were found between patients who received the standard dose and those who received the lower dose with regard to tumor control and ocular complications. Thus, the optimal dose level to achieve tumor control and minimize ocular morbidity has not been established. Nevertheless, in select patients, i.e., those with small- or medium-sized tumors located near the optic nerve or fovea, a dose of 50 CGE is chosen in an effort to reduce vision-threatening treatment complications. At several facilities in Europe, a total dose of 60 CGE is given in four equal fractions over 4 days.23–25
Clinical findings in treated patients
To date, more than 3500 patients with uveal melanomas have been treated at Massachusetts Eye and Ear Infirmary and Massachusetts General Hospital. The mean age of patients at the time of diagnosis was 61 years. Diagnosis before age 40 was uncommon, representing 12% of treated patients. Bilateral involvement and extrascleral extension were rare (approximately 1% and 4%, respectively). The median basal diameter of treated patients was 13.2 mm (range: 5.0–28.0 mm) and median tumor height was 5.3 mm (range: 0.6–17.1 mm). Approximately 26% of patients had small tumors (≤10 mm greatest diameter and 2.5 mm in height), and approximately half had medium-sized tumors (>10 mm and ≤16 mm in diameter and/or >2.5 mm and ≤10 mm in height). Nearly 20% had large tumors (>16 mm in diameter and >10 mm in height). More than two-thirds of the treated tumors were located within 3 mm of the optic nerve or macula.26 Approximately 20% of the patients had 20/20 or better visual acuity at presentation, and less than 10% had visual acuity of counting fingers or worse.
Results
Tumor regression
The majority of treated tumors show some regression after the first 6 months of treatment, with a usual range between 1 and 24 months.27 Disappearance of the lesion, or formation of a flat scar is observed in 15% of eyes. Resolution of a secondary serous retinal detachment is usually the earliest finding. Detachments can transiently increase in size during the first few months after treatment, but most eventually resolve. Continuous regression of the tumor over several years is frequently observed. Tumor regression is thought to be due primarily to direct killing of tumor cells by irradiation, and secondarily to the effect of radiotherapy on the tumor vasculature. Cell death from irradiation is achieved by damage to chromosomal DNA, with subsequent loss of proliferative potential. Damage to DNA is lethal when the cell enters mitosis. Delayed regression, observed in some irradiated tumors, is probably due to prolonged intermitotic phases of melanoma cells. This protracted pattern of tumor regression has been supported by histologic studies of tumors enucleated at varying times after proton therapy, which showed a greater decline of mitotic figures with longer periods between irradiation and enucleation. Tumors enucleated more than 30 months after irradiation had no mitotic figures.28 Rapid regression of tumors has been associated with higher rates of metastasis in both proton-irradiated29 and plaque-treated patients,30 suggesting that more aggressive tumors, due to more rapidly dividing cells, are more radiosensitive.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


