Thyroid reoperation is known to carry a higher risk for complications because of the increased challenge of identifying tissue planes, presence of adherent strap muscles, and generalized scarring of the thyroid bed. Consideration of postsurgical changes in the anatomy of important landmarks, such as the recurrent and superior laryngeal nerves, brachiocephalic artery, and parathyroid glands, is crucial during preoperative planning for thyroid reoperations. This article provides a review of these key changes in surgical anatomy and the implications of the anatomic changes after thyroidectomy.
Reoperations in the thyroid bed are surgically challenging because of distortion of anatomic planes and scarring from prior surgery. These technical challenges have resulted in an effort to treat thyroid disease completely at the time of the initial operation. In circumstances of residual or recurrent disease, however, thyroid reoperations are unavoidable. Within the surgical bed after thyroidectomy, postoperative fibrosis, degenerative cysts, fat necrosis, and suture granuloma have been identified . These findings can be difficult to distinguish from recurrent disease. Additionally, alteration of anatomic structures occurs from fibrosis and wound contracture. The purpose of this article is to further define anatomic variations and relationships of key anatomic structures in the neck and thyroid bed after thyroidectomy. The anatomic considerations are not all-inclusive but are designed to provide a framework for thyroid reoperation.
Indications for reoperation
The indications for reoperation after thyroidectomy fall into three broad categories: malignancy, multinodular goiter, and thyrotoxicosis . Malignancy is the most common indication for reoperation. Frequently, a second operation is required as a result of a histologic diagnosis of malignancy on a permanent section not identified on fine-needle aspiration or frozen section. The histologic diagnosis of thyroid cancer, especially follicular lesions, is challenging even to experienced pathologists and changes in diagnosis on permanent section can occur at rates of up to 50% . Reoperation also can be required for residual or recurrent tumor after unsuccessful I-131 ablation and nodal disease in the central or lateral neck.
A symptomatic recurrence of a multinodular goiter also necessitates thyroid reoperation. Over the past several decades, the extent of thyroidectomy in patients who have had multinodular goiter has been controversial. Although many surgeons now opt for a total thyroidectomy, classically a subtotal thyroidectomy was performed to minimize operative risk and leave a small portion of functioning tissue . The remaining tissue can then lead to a recurrence of toxic or nontoxic multinodular goiter, requiring reoperation. Recurrent thyrotoxicosis or other inflammatory conditions of the thyroid gland unresponsive to medical management are additional indications for reoperation.
Risks of reoperation
The risks of thyroid surgery are known to be increased at the time of reoperation. A recent review reported an overall transient morbidity rate of 8% and a permanent morbidity rate of 3.8% . The major transient and permanent complications involve damage to the recurrent laryngeal nerve (RLN) and hypoparathyroidism. In a comparison of reoperation and primary surgery of the thyroid, a higher rate of RLN palsy (3.4% versus 1.1%) and hypoparathyroidism (3.9% versus 1.2%) was reported in the reoperative group . Other investigators have reported similar complication rates of permanent RLN palsy and hypoparathyroidism of up to 4% . This equates to relative risks for RLN palsy and hypoparathyroidism to be 3.4 and 1.9, respectively . A central neck dissection, indicated for metastases to the paratracheal and mediastinal lymph nodes, carries the same risks and complications as does surgery to the thyroid remnant .
Several factors contribute to the increased risk of reoperation. Often patients have undergone their initial surgery at another institution and status of the parathyroid glands, therefore, may be unknown. An initial nodulectomy or subtotal thyroidectomy can make identification of the RLN especially difficult . Recurrent locally invasive carcinoma, which can involve the trachea, larynx, RLN, and esophagus, requires challenging, aggressive surgical resection .
In an effort to avoid scar formation and thereby decrease the risk for surgery, a short interval to reoperation is advocated . Reoperation within 7 to 10 days or after an interval of 3 months is believed to avoid anatomic distortion from inflammation and scar formation. Not all patients are able to return to the operating room within 1 week, however, or agree to delaying a second operation for 3 months. Other investigators have found no difference in risk resulting from timing of reoperation, making the time frame for reoperation controversial .
Risks of reoperation
The risks of thyroid surgery are known to be increased at the time of reoperation. A recent review reported an overall transient morbidity rate of 8% and a permanent morbidity rate of 3.8% . The major transient and permanent complications involve damage to the recurrent laryngeal nerve (RLN) and hypoparathyroidism. In a comparison of reoperation and primary surgery of the thyroid, a higher rate of RLN palsy (3.4% versus 1.1%) and hypoparathyroidism (3.9% versus 1.2%) was reported in the reoperative group . Other investigators have reported similar complication rates of permanent RLN palsy and hypoparathyroidism of up to 4% . This equates to relative risks for RLN palsy and hypoparathyroidism to be 3.4 and 1.9, respectively . A central neck dissection, indicated for metastases to the paratracheal and mediastinal lymph nodes, carries the same risks and complications as does surgery to the thyroid remnant .
Several factors contribute to the increased risk of reoperation. Often patients have undergone their initial surgery at another institution and status of the parathyroid glands, therefore, may be unknown. An initial nodulectomy or subtotal thyroidectomy can make identification of the RLN especially difficult . Recurrent locally invasive carcinoma, which can involve the trachea, larynx, RLN, and esophagus, requires challenging, aggressive surgical resection .
In an effort to avoid scar formation and thereby decrease the risk for surgery, a short interval to reoperation is advocated . Reoperation within 7 to 10 days or after an interval of 3 months is believed to avoid anatomic distortion from inflammation and scar formation. Not all patients are able to return to the operating room within 1 week, however, or agree to delaying a second operation for 3 months. Other investigators have found no difference in risk resulting from timing of reoperation, making the time frame for reoperation controversial .
General anatomic considerations
Scar formation is the body’s natural response to disruption of normal tissue planes from manipulation or radiation. The response to surgical “damage” of tissue is a cascade of inflammation that begins with a fibrin clot and neutrophil infiltration. The neutrophils are believed to be pro-inflammatory mediators that encourage fibroblast and keratinocyte activation. Fibroblast activation and transformation into myofibroblasts, capable of contraction similar to smooth muscle cells, are important for wound contraction and collagen matrix production . The myofibroblasts are beneficial for wound closure but also result in fibrosis and scar formation in the areas of tissue disruption .
Fibrosis and scar formation has several implications during reoperation. The widely used capsular technique, made popular in 1973 by Thompson and colleagues , is technically difficult in a fibrosed thyroid remnant. The capsular technique relies on a plane between the thyroid capsule and inferior thyroid artery for a clean dissection around the thyroid gland. The tissue plane, now encased in scar, no longer remains. Furthermore, fibrosed tissue, more resistant to retraction, can lead to stretch injuries on the RLN. Along with increased traction, scarring leads to difficulty in structure identification and increased tissue manipulation and bleeding.
As a result of anatomic distortion, a retrograde or modified lateral approach to the thyroid remnant may be used. This approach allows access along the medial border of the sternocleidomastoid muscle and carotid sheath remaining lateral to the strap muscles rather than accessing the thyroid bed through the anterior midline scar . From any approach, adequate exposure, a heightened surgical awareness, and identification of key structures remain paramount to successful reoperation.
Strap muscles
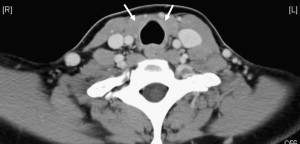
The strap muscles, or infrahyoid musculature, include the sternohyoid, sternothyroid, and superior belly of the omohyoid. Scarring of the strap musculature can distort the midline raphe on re-exploration and the strap muscles will be scarred in the area previously occupied by the thyroid gland ( Fig. 1 ). These muscles generally are re-approximated at the end of a thyroid operation and if the reoperation is after a brief time interval, suture or suture granuloma may be encountered. If not re-approximated, the trachea may have scarred anteriorly to the skin, which can be identified preoperatively by careful examination of the neck during swallowing.
Scarring of the strap muscles to the remaining thyroid tissue, trachea, and carotid sheath is especially challenging. The sternothyroid is associated most closely with the thyroid gland and the muscle must be separated from the thyroid gland for a capsular dissection. If prior surgery was undertaken for known malignancy, the overlying sternothyroid muscle may have been partially removed during the initial operation in an effort to remove all cancerous tissue . The carotid sheath then may be encountered in an unexpected medial location and the trachea encountered superficially.
If extensive scarring of the strap musculature has occurred, the strap muscles may be sectioned to gain better exposure. Strap muscles should be divided superiorly so as not to disturb the innervation by the ansa cervicalis, which inserts more inferiorly . Another limiting factor to exposure can be the insertion of the sternothyroid into the thyroid cartilage, which limits the midline rotation of the thyroid lobes . This attachment should be identified carefully and sectioned if rotation of the gland or lateral exposure is difficult.
Recurrent laryngeal nerves
Identification and preservation of the RLN is the most critical challenge during thyroid reoperation. Damage to the RLN is a known risk with devastating consequences to patients. Identification of the RLN can be difficult as a result of scar formation over the nerve or change in location of the RLN because of overall wound scarring and contracture. The use of intraoperative RLN nerve monitoring can play an adjunctive role in aid of identification of the RLN in these high-risk operations . The intraoperative nerve monitor is shown to be safe, reproducible, and valuable for nerve identification and protection . Despite the usefulness of the intraoperative nerve monitor, visualization of the RLN remains the gold standard for nerve protection .
Adequate exposure is a key tenet in identification of the RLN. There are two approaches to achieving this goal: superior or inferior. The literature remains controversial regarding which approach is best. Many investigators advocate an inferior approach to the RLN to avoid formed scar . A substernal goiter, however, prevents initial identification of the RLN inferiorly, as the superior aspect of the gland first must be mobilized. Additionally, the technique of identifying the nerve in the inferior part of the thyroid region at the crossing of the inferior thyroid artery is not possible during re-exploration if the gland previously was removed. A superior approach identifies the RLN at the point of laryngeal penetration immediately behind the inferior cornu of the thyroid cartilage . If extensive fibrosis is encountered the upper pole, identification of the RLN at the upper pole can be a dangerous endeavor. Therefore, based on surgeon experience and comfort, each approach must be individualized and selected by identifiable anatomic structures.
Wound contracture is a natural response to wound repair, but this contracture can medialize the RLN. The RLN has been identified anterior to the trachea during reoperation and easily can be severed during removal of thyroid tissue from the trachea . Literature reports that even after identification of the RLN, a medial branch of the identified nerve has been severed during reoperation . Dissection should not be performed on the anterior tracheal wall without first identifying the RLN. Attention to nerve identification during the initial stages of the operation is crucial as scarring of the strap musculature to deeper tissue may bring the RLN to a more anterior location than expected. Finally, if a patient has RLN palsy from prior operation, it is reasonable to leave a small remnant of thyroid tissue on the contralateral RLN and use I-131 ablation as necessary if it remains an option .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


