CHAPTER 54 Cerebrospinal Fluid Rhinorrhea
Historical Perspective
CSF rhinorrhea was first reported in the 17th century.1 In the early 20th century, Dandy2 reported the first successful repair, which used a bifrontal craniotomy for placement of a fascia lata graft. Although this surgical strategy provided direct access for the repair, reported failure rates were quite high and the procedure entailed the morbidity of craniotomy. In fact, reported recurrent rates were as high as 27%,3 and in one series only 60% of leaks were successfully repaired.4
Extracranial approaches were introduced in the mid-20th century. In 1948, Dohlman5 presented a patient whose CSF leak was repaired through a standard naso-orbital incision. Several years later, Hirsch6 reported the successful closure of two sphenoid sinus CSF leaks through a pure endonasal approach. In 1964, Vrabec and Hallberg7 described the repair of a cribriform defect through an endonasal route. All of these endonasal procedures were performed before the advent of surgical nasal endoscopy.
Endoscopic approaches were introduced and popularized in the 1980s and early 1990s. Both Wigand8 and Stankiewicz9 described closure of incidental CSF leaks during endoscopic sinus surgery. In 1989, Papay and colleagues10 introduced rigid transnasal endoscopy for the endonasal repair of CSF rhinorrhea, and in 1990, Mattox and Kennedy11 presented another series of cases in which the CSF rhinorrhea was addressed with use of endoscopic visualization. Since then, numerous series have been published,12–14 and endoscopic repair has emerged as a mainstay of surgical management.15
Classification
Box 54-1 summarizes a classification system for all cases of CSF rhinorrhea. This approach, which is based on the established pathophysiology of CSF rhinorrhea, has important clinical implications for the selection of treatment strategies as well as patient counseling about prognosis.
Box 54-1 Classification of Cerebrospinal Fluid Rhinorrhea
The importance of accurate classification was first recognized by Ommaya and associates,16 who proposed dividing CSF rhinorrhea into traumatic and nontraumatic forms. These researchers believed that the application of the term “spontaneous” to cases of CSF rhinorrhea was inappropriate because comprehensive investigations of all cases of CSF rhinorrhea should reveal the true proximate cause. Most cases of so-called spontaneous rhinorrhea have a specific etiology, so the term “spontaneous” is probably best reserved for cases of true idiopathic CSF rhinorrhea, in which various investigations cannot determine a specific cause.
Data about the incidence of CSF rhinorrhea are sparse. Only 4% of all CSF leaks are nontraumatic, and 16% occur as a direct result of intracranial and extracranial procedures.17 The vast majority result from accidental or surgical trauma. Approximately 80% of all cases of CSF rhinorrhea occur in the setting of accidental trauma, mostly in the form of closed-head injury. Conversely, CSF rhinorrhea is noted in only 2% to 3% of cases of serious head trauma.17 The presence of a skull base fracture is associated with a CSF fistula in 12% to 30% of cases.18 More than 50% of CSF fistulas resulting from accidental head trauma are located at the anterior cranial base, most of them involving the cribriform plate.19,20 The majority of traumatic CSF leaks become clinically evident within 2 days, and almost all manifest within 3 months after the traumatic event.21 Most CSF fistulas resulting from accidental head trauma resolve spontaneously or with conservative management, including lumbar drainage and bed rest.
Pathophysiology
CSF is produced by the choroid plexus in the ventricles at a rate of 20 mL per hour in adults. The CSF circulates from the ventricles through the foramina of Luschka and Magendie to the subarachnoid spaces around the cerebral hemispheres, cerebellum, and spine. Total CSF volume is 140 mL, consisting of 20 mL in the ventricles, 50 mL in the intracranial subarachnoid space, and 70 mL in the paraspinal subarachnoid space. The typical upper limit of normal CSF pressure ranges from 40 mm H2O in infants to 140 mm H2O in adults. CSF pressure fluctuates with respirations and arterial pulse pressures as well as with changes in head position. CSF pressure is maintained by a relative balance between CSF secretion (from the choroid plexus) and CSF resorption (by the arachnoid villi). Because CSF secretion occurs at a steady rate, the rate of CSF resorption plays the major role in determining CSF pressure.22 Processes that disrupt CSF resorption tend to lead to increased intracranial pressure (ICP).
The other major factor in the pathogenesis of CSF rhinorrhea is increased ICP. Both an intracranial mass and hydrocephalus are associated with elevated ICP. Strong coughing and the Valsalva maneuver both serve to transiently increase ICP. Elevated ICP is also an important factor in cases of apparent idiopathic CSF rhinorrhea. In a series of publications, Schlosser and coworkers23,24 have noted that all patients who underwent clinically indicated lumbar puncture or drainage after successful endoscopic repair of nontraumatic CSF rhinorrhea had elevated ICP (mean 26.5 cm H2O in the first report23 and 32.5 cm H2O, in the second report24), suggesting that occult elevation of ICP may be an etiologic factor in even so-called idiopathic or spontaneous CSF rhinorrhea. It could be postulated that in patients with occult elevated CSF pressure, the CSF leak may serve as a release valve that decompresses the elevated pressure. (If the patient has an active leak at the time of lumbar puncture, the opening pressure may be normal—because the leak has decompressed the ICP. Thus, the increased pressure may be apparent only after a site of leakage has been surgically repaired.)
In at least certain instances, nontraumatic CSF rhinorrhea seems to result from abnormally elevated ICP. Given that elevated ICP is a primary characteristic of benign intracranial hypertension (BIH), the pathophysiology of nontraumatic CSF rhinorrhea and that of BIH may be similar. Benign intracranial hypertension, also known as idiopathic intracranial hypertension and pseudotumor cerebri, is a syndrome of increased ICP in the absence of specific causes such as intracranial masses, hydrocephalus, and dural sinus thrombosis. Clinical manifestations of BIH include headache, pulsatile tinnitus, papilledema, and visual disturbances including abducens nerve palsy. Most patients with BIH are obese, middle-aged women. In fact, the demographics of the population with spontaneous CSF leak are quite similar to those of the average population of patients with BIH.25 Thus the diagnosis of BIH must be examined in the setting of spontaneous CSF rhinorrhea. In fact, Schlosser and coworkers26 demonstrated that 8 of 11 patients (72%) with apparent idiopathic CSF rhinorrhea strictly fulfilled the modified Dandy criteria used by neuro-ophthalmologists to make the diagnosis of BIH.26 The other 3 patients fulfilled most but not all the criteria.
In a separate publication, Schlosser and Bolger27 assessed the incidence of an empty sella in 15 patients with apparently spontaneous CSF rhinorrhea and in 9 patients with nonspontaneous CSF rhinorrhea and noted a statistically significant (P = .01) greater incidence of empty sella in the nontraumatic CSF leak group (100% vs. 11%, respectively). An empty sella may therefore serve as a marker of elevated ICP.28 Normally, the pituitary gland fills the entire sella turcica; however, if arachnoid and CSF herniate through the sellar diaphragm, this CSF-filled sac may partially or completely compress the pituitary gland. When this compression occurs, an “empty sella” results. The clinical manifestations and demographic profile of patients with empty sella syndrome (ESS) are highly similar to those for patients with BIH and patients with nontraumatic CSF leaks. The clinical presentation of ESS includes headache, memory losses, cerebellar ataxia, papilledema, and visual field defects. In addition, many patients with ESS are obese, middle-aged women with elevated body mass index (BMI). In a later report, Silver and colleagues29 demonstrated that the radiographic signs displayed in 14 patients with nontraumatic, apparently idiopathic, CSF rhinorrhea were largely similar to those seen in patients with ICP and BIH. The signs included arachnoid pits in 79% of patients, empty sella in 50% of patients, meningoencephaloceles in 50% of patients, and dural ectasias in 35% of patients. Because ESS is associated with altered CSF circulation dynamics,30 treatment of nontraumatic CSF rhinorrhea, which has a demonstrated association with ESS, should include consideration of the concomitant diagnosis of ESS as well as the potential clinical impact of ESS.
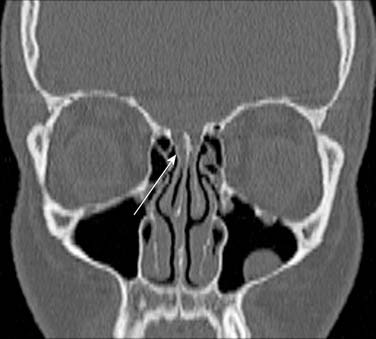
The bony architecture of the skull base plays a role in the development of CSF rhinorrhea. Certainly bony dehiscences or even partial thinning weakens the normal barrier that separates the subarachnoid space from the paranasal sinus space. Alternatively, these weaknesses can be considered congenital anomalies. In addition, specific areas of the skull base are normally quite thin. In particular, the lateral lamella of the cribriform plate (LLCP) has been well recognized as an area of potential weakness (Fig. 54-1). The length of the LLCP shows considerable variation; if the LLCP is especially long, this anatomic variation weakens a significant portion of the skull. Congenital dehiscences in the lateral sphenoid roof, occurring from persistence of the lateral craniopharyngeal canal (Sternberg’s canal), have also been implicated in the pathogenesis of sphenoid CSF leaks and meningoencephaloceles.31,32 In all instances of thinning of the bony skull base, the pressure from the overlying intracranial contents coupled with constant dural pulsations may further erode the weakened area with the resultant development of CSF rhinorrhea.
Although skull base trauma leading to CSF rhinorrhea during or after routine endoscopic sinus surgery is a rare event, the frequency of this procedure makes this complication an important cause of CSF rhinorrhea today.9,33,34 Inadvertent pressure along the thin skull base may fracture the skull base and lacerate the dura. Because the LLCP is the weakest part of the skull base, even minor trauma in this region may cause CSF rhinorrhea. Aggressive middle turbinate retraction or resection (Fig. 54-2) may be associated with LLCP injury. The mechanism of injury during the procedure should also be considered. It is likely that powered instrumentation produces a greater skull base injury than the standard sinus forceps and through-cutting forceps. Powered instrumentation is invariably associated with greater removal of tissue; as a result, the resultant skull base defect may be quite extensive. Later generations of powered instrumentation may increase the risk of this complication, because they can remove tissue more quickly and easily. CSF rhinorrhea may occur both intraoperatively and postoperatively. When patients report symptoms that are consistent with CSF rhinorrhea after sinus surgery, the diagnosis of CSF rhinorrhea should be considered, even if the procedure itself was seemingly uneventful.




