CHAPTER 166 Central Vestibular Disorders
The first task of an otolaryngologist in examining a patient with dizziness is to determine if the symptom is of central or peripheral origin1 (Table 166-1). Some central causes of acute vertigo can be life-threatening and may necessitate immediate intervention.2 The differentiation can almost always be made by physical examination based on the type of nystagmus, result of head thrust test, severity of imbalance, and presence or absence of other neurologic signs.
Table 166-1 Differentiation of Central and Peripheral Vertigo
| Feature | Central Origin | Peripheral Origin |
|---|---|---|
| Imbalance | Severe | Mild to moderate |
| Neurologic symptoms | Frequent | Rare |
| Nystagmus | Changes direction No change with fixation | Unidirectional Decreases with fixation |
| Hearing loss | Rare | Frequent |
| Nausea | Variable | Severe |
| Recovery | Slow | Rapid |
Spontaneous nystagmus of peripheral origin typically is horizontal, or horizontal with a torsional component, and does not change direction with direction of gaze. Spontaneous nystagmus of central origin also can be purely horizontal but often is purely vertical or torsional and usually changes direction with changes in gaze.1
The head thrust test is performed as follows: The examiner grasps the patient’s head and applies a brief, high-acceleration head rotation, first in one direction and then the other.3 During these maneuvers, the patient fixates on the examiner’s nose and the examiner watches for corrective rapid eye movements (saccades), which are a sign of decreased vestibular response (i.e., the eyes move with the head, rather than remaining fixed in space). If a “catch-up” saccade occurs after head thrusts in one direction but not in the other, a peripheral (including the labyrinth and the eighth cranial nerve on its course from the brainstem) lesion on that side is likely.
Migraine
Migraine is characterized by recurrent headaches associated with nausea, vomiting, hypersensitivity to light, sound, and smell.4 This clinical entity is an important consideration in the diagnosis because patients with migraine often present with dizziness. Neurologic aura symptoms are present in one third of migraine patients. Migraine affects nearly 25% of women, 15% of men,5,6 and 5% of children.7 In the prepubertal period, boys with migraine slightly outnumber girls, but at puberty, migraine decreases in boys and increases in girls, so that a 2 : 1 female preponderance is established by adulthood.8 Migraine typically begins in young adulthood, with onset of symptoms after the age of 40 in only 10% of sufferers.
The diagnosis and classification of migraine and other headache disorders have been a controversial issue. The most recent effort of the Headache Classification Committee of the International Headache Society (IHS)4 sets up criteria that allow meaningful comparisons of groups of patients between centers. The IHS classifies the most common type of migraine as migraine with and migraine without aura (Box 166-1); other classified types of migraine headache have been designated but are not considered in this chapter because they will only rarely be encountered by the otolaryngologist.
Box 166-1 Diagnostic Criteria for Migraine
Migraine without Aura
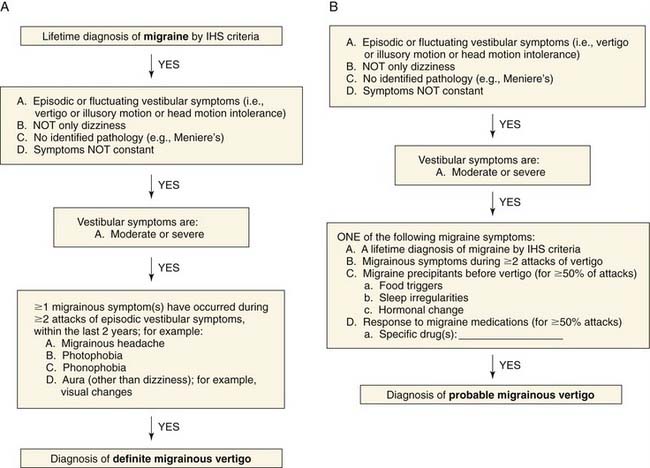
The definition of migrainous vertigo also has been controversial. Neuhauser and colleagues9 proposed criteria for definite migrainous vertigo as follows: (1) episodic vestibular symptoms (rotational vertigo, other illusory self or object motion, positional vertigo, head motion intolerance) of at least moderate severity; (2) migraine according to IHS criteria; (3) at least one of the following migrainous symptoms during at least two vertiginous attacks: migrainous headache, photophobia, phonophobia, visual or other auras; and (4) other causes ruled out by appropriate investigations. Probable migrainous vertigo was the designation chosen for patients who did not meet definite criteria but were still believed to have migrainous vertigo as the most likely diagnosis. This definition requires criteria 1 and 4 from the foregoing list, plus at least one of the following: migraine according to IHS criteria; migrainous symptoms during vertigo; migraine-specific precipitants of vertigo (e.g., specific foods, sleep irregularities, hormonal changes); and response to antimigraine drugs. A diagnostic algorithm10 for definite and probable migrainous vertigo (Fig. 166-1) has been proposed.
Vestibular Symptoms
Vertigo
Vertigo is extremely common in patients with migraine and occurred in 26.5% of Kayan and Hood’s group of patients with migraine, compared with 7.8% of those with tension headache (P < .001).11 Some studies have found the incidence of vertigo in classic migraine sufferers to be as high as 42%.12 The severity of vertigo in patients with migraine tends to be greater than in those suffering from tension headaches. Vertigo severe enough for the patient to seek medical attention for relief occurred in 5% of those with migraine but in less than 1% of those with tension headache.11
The temporal relationship of vertiginous spells to migraine headaches is important to ascertain. Vertigo does not usually manifest as an aura immediately preceding the headache as a prodrome. Of the 53 patients with vertigo and migraine interviewed by Kayan and Hood,11 the vertigo immediately preceded the headache in only 15%, whereas it occurred during the headache in 47% and during the headache-free interval in 36% of patients. In a series of 50 patients with basilar migraine, Olsson13 and Cuttler and Baloh14 also found vertigo to occur more often during the headache-free interval than as a prodrome before the headache.
Motion Sickness
The relationship between migraine and motion sickness is well established. In his seminal study of 9000 Swedish schoolchildren, Bille15 matched children with more pronounced migraine to children in a similar group without migraine. Severe motion sickness was present in 49% of the children with migraine and in only 10% of the control group. Barabas and colleagues found that 45% of 60 children with migraine experienced at least three episodes of motion sickness culminating in vomiting, compared with 5% to 7% of three similar-sized control groups of subjects with non-migraine headaches, seizure disorders, and learning disabilities or neurologic perceptual impairments.16 In adults, a similarly significantly greater incidence of motion sickness has been observed in patients with classic migraine than in patients with tension and cluster headaches.12 In the Kayan and Hood11 series of 200 unselected patients with migraine, 51% reported motion sickness, compared with 20% of the patients with tension headache.
Auditory Symptoms
Of the patients studied by Kayan and Hood,11 20% complained of hearing loss, tinnitus, or pitch distortion, and one fourth of the 20% had multiple auditory symptoms. In descending order of frequency, the temporal patterns for occurrence of these symptoms were during the headache, during the headache-free interval, and immediately before the headache. The temporal relationship of these symptoms mirror the relationship of vertigo to headache in this same series.
Hearing Loss
The association of hearing loss to migraine is reported to be approximately 7%.11 Hearing loss is a more prominent symptom in patients with basilar migraine. In Olsson’s study,13 52% of the patients noticed a change in hearing as part of the aura immediately preceding the migraine headache and 50% had a fluctuating low-frequency sensorineural hearing loss. A group of migraine patients in whom hearing loss thought to be due to vasospasm has been reported.17
Tinnitus
Tinnitus was experienced by 15% of migraine patients, but none with tension headache,11 and in more than 60% of basilar migraine patients.13
Distortion
Although distortion was noted by only 4% of patients in the Kayan and Hood series,11 its actual prevalence may be higher. More attention may be given to more bothersome symptoms, and auditory distortion may be ignored by physicians and patients alike as unimportant.
Phonophobia
Loud noise aversion distinguishes patients with migraine from those suffering other types of headaches. Only 12% of tension headache sufferers experienced phonophobia, but 81% of those with migraine had the symptom.11 Olsson13 detected phonophobia in patients with basilar migraine at a rate of 70% during headache and 76% during headache-free intervals. Furthermore, he documented an abnormal loudness discomfort level in 78% of these patients, whereas only 14% had abnormal speech reception thresholds.
Migraine Associated with Neuro-otologic Symptoms
Basilar Migraine
Bickerstaff18 described a form of migraine ascribed to ischemia in the distribution of the basilar artery. This syndrome currently is known as basilar migraine, replacing “basilar artery migraine” and “posterior fossa migraine,” which occasionally appear in the older literature. This subtype of migraine was similar to classic migraine in that it consisted of an aura followed by a severe headache. However, a majority of affected patients were adolescent girls, in whom the migraine attacks often occurred premenstrually. Later observers emphasized other aspects of the clinical picture such as stupor,19 loss of consciousness,20 neurologic symptoms,21 hearing loss, and vertigo.22 These symptoms are thought to be due to involvement of the brainstem, cerebellum, cranial nerve nuclei, and occipital lobe cortex.
Migraine without Headache
Migraine should not be eliminated as a cause for vertigo just because headaches are not present. Whitty23 reported on a series of patients with symptoms typically experienced during a migraine aura but no headaches. In these patients, typical headaches sometimes developed later in life, or auras that were only intermittently related to headaches were noted. Other observers have described similar patients using the term migraine equivalent24–26 or migraine accompaniments.27 A history of motion sickness, premenstrual clustering of attacks, or headaches associated with some of the attacks is frequent. Personal or family history of migraine also is helpful in diagnosing these patients.
Etiology
Historically migraine headache was thought to result from dilation of intracranial and dural arteries causing stretching of pain fibers in the walls of the arteries. The complex phenomena associated with migraine cannot be fully explained by a vascular theory. More recently, neurally based spreading of depression activity has been implicated,28,29 although the neurophysiology is far from completely understood.
A family history of migraine is present in approximately 40% to 90% of affected persons, compared with 5% to 20% of unaffected subjects. When migraine sufferers with and without aura are examined separately, patients who have migraine with aura are more likely to have affected family members. When twins are studied, conconcordance rates for migraine are only 10% to 34%, depending on the country, suggesting that both genetic and environmental factors play a role.30
Familial hemiplegic migraine (FHM) is a rare type of migraine that affects only 0.01% of the general population.31 However, the underlying cellular cause is relatively well understood. Unlike most types of migraine, FHM has a clear autosomal dominant pattern of inheritance. Thus far, mutations have been found in three different genes that determine neuronal excitability.
Management
Treatment of migraine has historically been focused on headache symptoms. Management of migraine headache can be divided into two categories: symptomatic and prophylactic. Some interventions are useful in ameliorating the symptoms of the acute attack, whereas others are designed to reduce the frequency or severity of attacks. Symptomatic management includes analgesics, antiemetics, antivertiginous drugs, sedatives, and vasoconstrictors. In many patients, over-the-counter analgesics such as ibuprofen, aspirin, or acetaminophen and rest are all that is needed to relieve headache symptoms. Decreased gastric motility occurs during and between migraine attacks, which may decrease absorption of oral drugs, contributing to nausea and vomiting.32 Metocopramide promotes normal gastric motility and may improve absorption of oral medication.
Nutrition may play a significant role in the frequency and severity of migraine headaches and migraine-associated dizziness. Riboflavin (vitamin B2) has been shown to be more effective than placebo in reducing the frequency of migraine headache when given in a dose of 400 mg daily.33 High-dose magnesium also has been found to have a therapeutic effect on migraine; suggested mechanisms have included inhibiting platelet aggregation, counteracting vasospasm, stabilizing cell membranes, and anti-inflammatory effects.34 Patients suffering from migraine symptoms have been found to have lower levels of magnesium, and infusion of magnesium can relieve symptoms.35 Magnesium given orally in a dose of 600 mg daily also has been shown to decrease headache symptoms36; however, diarrhea is a potential side effect at these doses.
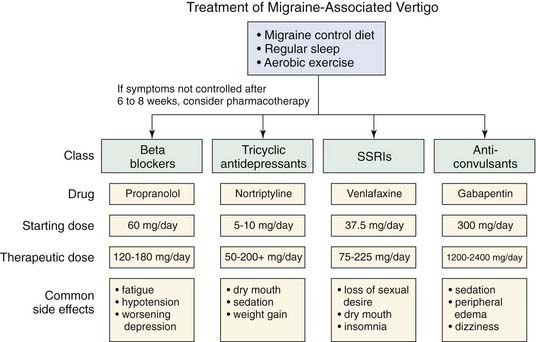
Food sensitivity may be a migraine trigger in a significant number of patients with migraine symptoms.34 Although some patients have observed that consuming a certain food will reliably provoke a headache, the effect of diet is more subtle. Foods that should be avoided include red wine, aged cheeses, beer, chocolate, caffeine, and yogurt.37 Alcohol itself does not seem to be a trigger, because vodka consumption does not provoke attacks.38 Dietary modification may be considered as first-line therapy for migraine prophylaxis (Fig. 166-2).
Vestibular migraine symptoms often are not directly related to the headache symptoms, and in some cases, dizziness as a manifestation of migraine can be present nearly continuously. Treatment of vestibular migraine has tended to mirror that of traditional migraine symptoms, and medications that alleviate headache symptoms also tend to be effective for vertigo symptoms.39 However, because the migraine-associated dizziness often is much more frequent than the headaches, prophylaxis usually is necessary.
Sumatriptan (Imitrex), a 5HT1D receptor agonist, has become the principal drug to abort severe migraine headache. Initial trials indicate that in 90% of cases the drug effectively aborts migraine headache symptoms within an hour of their onset when it is given subcutaneously; in 70% to 85%, symptoms may be aborted within 2 hours.40 Common side effects include sensations of heaviness and pressure in the chest, with coronary artery vasospasm more rarely reported. Although sumatriptan is remarkably effective in relief of early migraine headaches, breakthrough is common, and the drug has limited efficacy for concurrent vestibular symptoms.
Propranolol (Inderal) is the drug most commonly used for preventing migraine episodes. Approximately 50% to 70% of patients with headache symptoms derive benefit from prophylactic propranolol therapy, which also may be beneficial for vertigo symptoms.21 The medication is contraindicated in patients with asthma, congestive heart failure, peripheral vascular disease, diabetes, or hypothyroidism. Principal side effects include fatigue, lethargy, and dizziness, which usually occurs on rising from a seated or supine position. Side effects are minimized by slowly increasing the dose from a low starting level. Doses of 80 to 180 mg per day usually are effective. The medication should be continued for at least 2 to 3 months at the highest level of tolerance before it is considered a failure. On discontinuation, the drug should be gradually tapered over several days.
Calcium channel blockers (nifedipine, verapamil) also have been reported to reduce the frequency of migraine attacks, but the effect is likely to be only modest.41 Diltiazem (Cardizem) does not seem to have any effect on migraine prevention.
Tricyclic antidepressants also have been shown to decrease the frequency and severity of migraine attacks. Amitriptyline is perhaps the most-studied drug in this category, with several studies showing its efficacy.42 Starting doses usually are 10 to 25 mg, which usually is given at bedtime, to avoid the side effects of sedation and anticholinergic activity. Weight gain is a side effect that limits patient compliance with therapy in some populations. Therapeutic doses usually are 50 to 100 mg, with some patients who also suffer from depressive symptoms requiring doses of up to 400 mg. Nortriptyline is less sedating than amitriptyline and has a dosage profile similar to that of amitriptyline.
The role for selective serotonin reuptake inhibitors (SSRIs) for treatment of migraine remains controversial. Some evidence shows that they seem to be less effective than tricyclic antidepressants43 for headache symptoms. However, in patients with chronic subjective dizziness as their primary symptom, SSRIs seem to be effective.44
Clinical trials have shown gabapentin (Neurontin) to be effective at dosages of 1200 to 2400 mg per day,45 which usually is divided into three doses daily. Dizziness, peripheral edema, and somnolence are common side effects.
Acetazolamide (Diamox) has been shown to be effective in preventing migraine headaches and episodic vertigo in families who also exhibit essential tremor.46 However, it has not been shown to be of benefit in larger migraine headache populations.47 It may be effective in ameliorating motion-induced vestibular symptoms in patients with migraine.
Vestibular Disorders Associated with Migraine
Benign Paroxysmal Positional Vertigo
BPPV is the most common cause of peripheral vertigo. The disorder probably is due to free-floating particles in the semicircular canal (canalithiasis), which usually collect in the posterior semicircular canal owing its low point with respect to gravity. Classic symptoms include brief episodes (lasting less than 1 minute) of vertigo when the head is tilted backwards or during rolling over in bed. An extensive discussion of diagnosis and treatment of this common disorder is outside the scope of this chapter. Of note, however, migraine and motion sickness are three times more common in patients with BPPV than in the general population, with 59% of patients having a family history of migraine.48
Meniere’s Disease
Meniere’s disease classically manifests with unilateral low-frequency fluctuating hearing loss, a sense of aural fullness, and dizziness lasting several minutes to hours.49 However, the presence and severity of these symptoms are variable, which can overlap with those of migraine.50
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


