CHAPTER 211 Caustic Ingestion
The preceding quote comes to mind when reviewing more recent caustic ingestion literature, most of which is from developing countries. Over the last decade, numerous articles have been published from various institutions in the developing world.1–10 The fundamental problem is “uncontrolled and cheaper domestic cleaners have been introduced through common informal or open markets.”6 More recent reports estimate the incidence of caustic injuries in the United States to be 5000 to 15,000 per year; this low incidence has not always been the case.5 During the early 1900s, in concert with the ready availability of cleaning solutions composed of strong alkalis or acids, reports of caustic ingestions filled the medical literature. These early cleaning solutions were packaged in inconspicuous containers that concealed the potential danger of the content. This public health issue was highlighted in a landmark article in 1921 by Jackson,10 developer of the first distal lighted esophagoscope. Supported by extensive lobbying efforts by Jackson, the U.S. Congress passed legislation that controlled the sale of these potential toxins in 1927. Legislation led to the 1953 creation of the first National Poison Control Center in Chicago. In 1971, the U.S. Federal Hazardous Substance and Poison Prevention Packaging Act passed, mandating childproof container caps and banning excessively hazardous products and concentrations.
Pathophysiology
Acid and alkali solutions are the two main categories of caustic products. Commonly ingested substances include cleaning agents, bleach, concentrated laundry detergent, concentrated ammonia, dishwashing detergent, alkali hair straighteners, nail-decorating liquids, sodium hydroxide–containing glucose testing tablets, and disk batteries.11–15 Extensive local damage can occur after ingestion of sodium hydroxide–containing glucose test tablets and disk-shaped batteries if they lodge in the esophagus. Disk-shaped batteries are easily swallowed, and if they become lodged cause injury by several mechanisms: leakage of alkali causing direct caustic injury; absorption of toxic substances; pressure necrosis; and electrical discharge, which can cause mucosal burns.16 Subsequently, the following types of esophageal injuries may occur: esophageal burn with or without perforation, tracheoesophageal fistula, and aortoesophageal fistula. Caustic substances present in farming homes used as disinfectants, pipeline clearance, and cattle horn removal are not subject to U.S. protective packaging legislation.17
Acid ingestion leads to coagulative necrosis with eschar formation that subsequently prevents further tissue penetration. Esophageal damage secondary to acid ingestion is less likely because of the protection afforded by the slightly alkaline pH of the esophagus, and because of the resistance of the squamous epithelium to acids. The antrum of the stomach is the most vulnerable region of the upper digestive tract to acidic substances owing to pooling and prolonged contact with the compound.18
Alkalis are responsible for more severe caustic ingestion sequelae; multiple factors contribute to the extensive damage. Direct contact with cell membranes leads to their disruption secondary to saponification and proteinate formation as the alkali reacts with membrane components. Solubility of alkalis allows for deeper penetration of the caustic agents typically in areas of anatomic narrowing (e.g., cricopharyngeus, aortic arch, left main stem bronchus, and diaphragmatic hiatus).18 Damage ceases only when the alkali is neutralized by its reaction with tissue. The histopathologic events that occur after a 10% sodium hydroxide burn of esophageal mucosa include edema of the submucosa, inflammation of the submucosa with thrombosis, sloughing of the superficial layers, necrosis of the muscular layer, fibrosis of the deep layers, and delayed re-epithelialization.19
Initial Assessment and Diagnosis
Patients with caustic ingestion present with many symptoms, ranging from asymptomatic to overt stridor with severe dysphagia secondary to laryngeal edema and hypopharyngeal or esophageal injury (Box 211-1). As with all injured patients, the primary survey focuses on airway, breathing, and circulation (ABCs). A rapid assessment of the patient’s airway and determination of the need for intervention is of primary importance. Simultaneously, patients suspected to have a severe injury should have large-bore intravenous catheters for early fluid resuscitation and medication. Patients with significant oral mucosal burns, tongue edema, hoarseness, stridor, and dyspnea should be monitored closely for possible airway obstruction.
Fiberoptic laryngoscopy is an invaluable tool in the assessment of hypopharyngeal damage and the risk of airway compromise. In a patient with an injured but stable airway, dexamethasone (20 to 30 mg intravenous bolus in adults; 0.5 to 1 mg/kg in children) can help prevent further deterioration. Direct visualization of the larynx is necessary for a successful and safe intubation; blind nasotracheal intubation should be avoided for fear of destabilizing a tenuous airway. If orotracheal intubation cannot be performed safely because of edema or exudate or both, a surgical airway (cricothyrotomy or tracheotomy) is the safer choice. Dyspnea associated with rales and rhonchi may indicate aspiration of caustic material or pulmonary edema. Chest and abdominal radiography should be obtained to rule out pulmonary infiltrates or free air. Patient complaints of epigastric pain and examination findings of peritonitis (e.g., abdominal wall rigidity, tenderness) are highly correlated with gastric injury.20
Vital information necessary for appropriate care of a patient with a caustic ingestion includes identification of the ingested agent and its characteristics (pH, concentration, physical form [i.e., granular, liquid]), time and setting of ingestion, and volume swallowed. The social setting of the ingestion may provide clues to the amount of caustic involved in the injury and should be explored in the history. Children ingest caustic substances accidentally while exploring their surroundings or because of lack of parental education or parental neglect.9,21 Adult ingestions are generally suicide attempts, and large volumes are ingested. In the laboratory, the amount of titratable base is a more accurate predictor of a strong alkaline substance.22 Vancura and colleagues23 showed esophageal ulceration at a pH 12.5 or greater and significant mucosal damage with sodium hydroxide concentrations of 0.4% in mongrel cats. pH is clinically a more practical, rapid method of estimating the risk of mucosal injury.
Although the acute crises of esophageal perforation and upper airway obstruction are more dramatic, the most common complications from strong alkaline burns result from the more protracted courses of fibrosis and delayed epithelialization. Superficial burns generally heal without sequelae; however, deeper injuries involving the muscular layer and submucosa are associated with a more extensive loss of mucosa with subsequent fibrosis. A characteristic esophageal stricture develops in four stages: (1) An intense inflammatory response with associated dysmotility occurs in the area of the burned mucosa and deeper layers. (2) Granulation tissue with fibroblasts brings a matrix of collagen fibers to the newly formed connective tissue. (3) These collagen fibers begin to contract 3 or 4 weeks after the initial injury, with irregular formation of this collagen matrix, which enables the formation of adhesive bands. (4) Pseudodiverticula form between these adhesions as the contracting process continues until a dense inflexible fibrous scar replaces the destroyed submucosa and muscular layers. Circumferential burns are much more likely to lead to a symptomatic stricture than are noncircumferential injuries.24
Endoscopy
The clinician’s principal diagnostic challenge lies in accurately predicting which ingestion injuries are prone to rapid, inconsequential healing, and which are prone to stricture formation or perforation. Endoscopy is the most useful method of assessing whether esophageal injury has occurred. Traditional adjunctive studies, such as barium esophagogram, are inadequate because of the reliance on motility disturbance and mucosal irregularities to detect injury25 and significant false-negative rates (30% to 60%).26,27 The usefulness of technetium 99m–labeled sucralfate has been shown; it has high sensitivity and specificity in determining the presence of an esophageal injury after pediatric caustic ingestion.28 The high sensitivity and specificity allow this nuclear medicine study to serve as a screen for injury; however, it does not determine severity of injury or enable intervention. Depending on radiography alone for guidance may lead the clinician to underestimate the degree of injury in some patients.
The timing and necessity of endoscopy remains a topic of debate. Proponents of endoscopy within 24 hours in all cases of caustic ingestions are supported by retrospective reviews detailing instances of significant esophageal injury despite the absence of symptoms or signs of mucosal burns.3,4,6,29–32 In citing the poor correlation of signs, symptoms, and esophageal injury, such studies frequently do not differentiate the form of the ingested substance (liquid vs. granular), and whether the asymptomatic burns were from more potent liquid alkalis. This association may lead to the conclusion that any form of an ingested caustic may cause significant distal injury even in the absence of signs or symptoms of mucosal burns. Although conservative and cautious, this approach may subject patients (and parents) occasionally to unneeded procedures, worry, and expense. In a retrospective study of 41 ingestions that noted the type of lye ingested, the granular form did not cause significant mucosal injury, whereas all strictures resulted from liquid alkalis.30
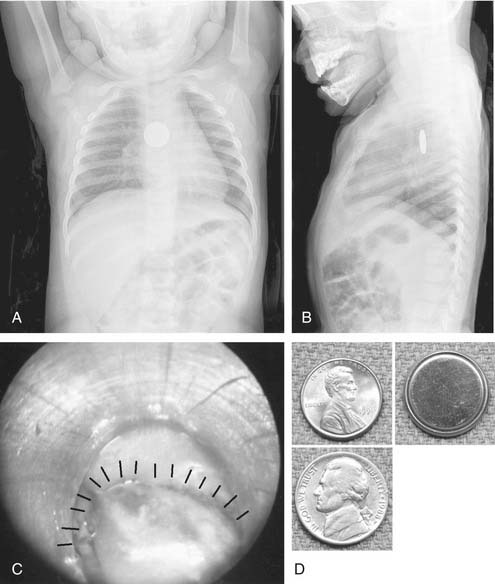
In contrast, toxic agents are accidentally swallowed in children as a result of innocent curiosity and confusion with food and drink. Just as children do not swallow a great deal of any distasteful food or medicine, they would not swallow any noxious, bitter acid or unpalatable granular lye. These compounds are rarely associated with significant esophageal burns because the volume ingested is generally very small.30,33,34 Exceptions have been reported, but these cases are associated with presenting combinations of oral burns, drooling, and dysphagia that easily raise suspicion that a significant amount of the compound has been swallowed. In cases of pediatric ingestion of acids or granular lye, endoscopy can be reserved for children with significant oral burns, dysphagia, or stridor. A glucose test tablet or disk-shaped watch battery needs to be endoscopically removed as quickly as possible because these items cause localized transmural necrosis and esophageal perforation. This recommendation can be extended to any coin-shaped object lodged in a child’s esophagus because some disk batteries may resemble a coin on chest radiographs (Fig. 211-1).
Most severe pediatric esophageal injuries are the result of just a few milliliters of a strong liquid alkali, usually sodium hydroxide. Some investigators have found that the presence of two or more signs and symptoms (e.g., oral burns, drooling, dysphagia, vomiting, stridor) reliably indicates esophageal injury significant enough to lead to stricture formation or perforation, requiring endoscopy.33–35 Based on evidence from a retrospective study, one series concluded that unless a pediatric patient is symptomatic (e.g., vomiting, drooling, oral lesions, respiratory distress, hemostasis), endoscopy is unnecessary because asymptomatic children were not found to develop sequelae. The authors of the series confined this recommendation to developed countries with a more controlled, lower concentration of alkalis and acids.36
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


