Cataract Surgery
Robert J. Cionni
Michael E. Snyder
Robert H. Osher
THE HISTORY OF CATARACT SURGERY
The unprecedented success of contemporary cataract surgery has been the result of continuing innovation in technique and technology. This section is meant to provide a quick overview of the major events in the history of cataract surgery that are responsible for the current state of the art. For an instructive, entertaining, and detailed review, the reader should peruse “The History of Cataract Surgery” by Norman Jaffe,1 “The History and Development of Phacoemulsification” by Charles Kelman,2 and “Harold Ridley and the Invention of the Intraocular Lens” by David J. Apple.3 Moreover, Stephen Obstabaum and Emmanuel Rosen must be given credit for the rapid dissemination of information in this specialized field, having devoted more than two decades serving as Editors of the American and European Cataract Journals.
It is remotely possible that ophthalmic surgeons would be experts at couching were it not for the French physician, Jacques Daviel, who reported the first series of extracapsular cataract extractions to the Royal Academy of Surgery in 1753.4 However Daviel’s operation did not become immediately popular because it required the management of the cortex. At that time, the operating microscope had not yet been invented, which made identification and removal of the cortex virtually impossible. Residual cortex was associated with severe and disastrous inflammatory reactions. Moreover, vitreous loss was a common and serious complication, given that the concept of vitrectomy did not yet exist.
Intracapsular cataract extraction was the standard at the beginning of the 20th century. Leaders of the American Academy of Ophthalmology and Otolaryngology were influenced by the work of Henry Smith in India, who had developed a quick, safe method of delivering the lens within its capsule using external manipulation.5 Intracapsular cataract extraction continued to evolve with the design of capsule forceps, Joaquin Barraquer’s discovery of the enzyme α-chymotrypsin to facilitate zonulolysis in 1957,6 and eventually the introduction of cryoextraction by T. Krawicz and Charles Kelman, independently, in 1961.7
Several major events raised the quality of cataract surgery to a new level during the 20th century. Ophthalmic sutures were introduced and anesthesia techniques improved. Intraocular visualization was enhanced by the development of loops and then, the operating microscope. Digital massage was found to decrease the risk of intraoperative complications. Then, two gigantic contributions changed cataract surgery forever.
The first came in 1949, when a British surgeon named Harold Ridley implanted the first intraocular lens (IOL) into the posterior chamber using the posterior capsule to support this heavy discoid implant.8 There were many complications and tremendous controversy concerning his intraocular implants. Even so, a new frontier had been established; superior visual rehabilitation could be achieved with IOL implants.
The next enormous contribution came in 1967, when Charles Kelman introduced the extracapsular small incision technique of phacoemulsification,9 which was at least as controversial as Ridley’s historic breakthrough. Both innovators suffered extreme ostracism, yet each was largely responsible for contemporary cataract surgery. Surgeons began to realize that phacoemulsification and IOL implantation resulted in exquisite control of the intraocular environment, greater safety in handling complications or challenging cases, quicker visual rehabilitation, and a reduction in surgically induced astigmatism. Therefore, the pendulum began to swing from intracapsular to extracapsular surgery. The latter enjoyed even greater acceptance as the protective nature of the posterior capsule became better understood when Gass and Norton initiated their fluorescein angiographic study of cystoid macular edema.10 Soon afterward David Kasner declared the “vitreous our enemy,” demonstrating the benefits of manual, and later, automated vitrectomy.11
Intraocular lens pioneers such as Cornelius Binkhorst, Peter Choyce, Jan Worst, Edward Epstein, Steven Shearing, and Svyatoslav Fyodorov among many others modified IOL design and the location for implantation. In England, John Pearce returned the IOL to the posterior chamber preceding the development of the Shearing style lens, which marked the real acceptance of the IOL. The safety and growing popularity of intraocular lenses was intimately linked to the introduction of Healon, a hyaluronic acid derived from Swedish rooster combs. It was Pape and Balaz who pioneered the concept of viscosurgery in 1979.12 Modern implant surgery was revolutionized by Richard Kratz, Robert Sinskey, William Simcoe, John Sheets, Norman Jaffe, Gerald Tennant, Eric Arnott, and Charles Kelman. Outstanding teachers such as David McIntyre, Jared Emery, Henry Hirschman, Herve Byron, Richard Lindstrom, Harry Grabow, Douglas Koch, Roger Steinert, and Samuel Masket spread the word as phacoemulsification techniques, improved instrumentation, and IOL designs proliferated.
Another huge step forward was taken in the early 1980s when French surgeon Danielle Aron-Rosa and her colleagues introduced the neodymium:yttrium-aluminum-garnet (Nd:YAG) laser for performing posterior capsulotomy, which eliminated an additional procedure in the operating room.13 Clifford Terry introduced the surgical keratotomer, which provided us with a new understanding of astigmatism,14 leading to the combination of astigmatic keratotomy with phacoemulsification to reduce pre-existing astigmatism introduced by Robert Osher in 1983.15,16 Then in 1985, Thomas Mazzocco developed and implanted the first foldable IOL17; Australian Graham Barrett and associates ushered us into the materials era with the use of silicone, hydrogels, and acrylics.18 Remarkable insights by David Apple correlated clinical observation with histopathology using the photographic technique developed by Kensaku Miyake of Japan.19
At about the same time, another Japanese surgeon, Kimiya Shimizu, began removing cataracts using topical anesthesia. A Canadian physician, Howard Gimbel and a German surgeon, Thomas Neuhann independently arrived at the concept of capsulorrhexis, although there is mounting evidence that Calvin Fercho20 was the first to perform a continuous curvilinear capsulorrhexis.21,22 Gimbel also popularized the divide and conquer technique,23 John Shepherd disassembled the nucleus into quadrants,24 and Kunihiro Nagahara introduced the concept of chopping in 1993.25 Ken Faust published the technique of hydrodissection26 and Douglas Koch described multilamellar hydrodelineation.27 Robert Osher modified the “phaco” machines by introducing the concept of slow-motion phacoemulsification, which allowed the surgeon to control the intraocular environment more exactly with variable ultrasound, aspiration rate, vacuum, and bottle height.28 John Shepherd introduced the horizontal one-stitch closure,29 eventually leading to the abandonment of sutures altogether, as championed by Michael McFarland.30 Howard Fine returned the smaller phacoemulsification incision back to the cornea using foldable IOLs.31
In the late 1990s, the transition from extracapsular surgery to phacoemulsification was almost complete, as surgeons enjoyed a quicker and safer near-clear or clear corneal incision, capsulorrhexis, hydrodissection, nuclear disassembly, the insertion of a UV-blocking foldable IOL, and a sutureless closure. The incidence of operative and postoperative complications was never lower and the recovery of excellent vision was achieved as technical advances in equipment, lens design, and biometry continued to improve. Intraocular lens formulas were refined by Donald Sanders, Manus Kraff, and Jack Retzlaff; Kenneth Hoffer; and Jack Holladay. Robert Osher challenged ASCRS to adapt a new standard in reporting visual results emphasizing the importance of early-uncorrected vision and promoting the new concept of refractive cataract surgery.32 Industry introduced higher-quality silicone and acrylic IOL materials, viscosurgical tools, and sophisticated phaco machines, which were more versatile and reliable.
At the turn of the century, the incidence of posterior capsular opacification (PCO), the most common untoward event after surgery, was plummeting as the result of a square edge design on the IOL optic. The haptics themselves had evolved from Prolene material to polymethylmethacrylate and then Alcon introduced a soft haptic on a single-piece acrylic platform. Every company developed an injector for improved IOL insertion, and industry was teaming up with innovative surgeons in developing a number of optic modifications. Attempts to achieve multifocality with diffractive optics had been introduced by 3M and their design team of Richard Lindstrom, John Sheets, and Robert Osher. This technology was placed on the back burner until Allergan developed the array multifocal IOL. Alcon purchased and improved the 3M defractive optic and introduced ReStor IOL on a single-piece acrylic platform. The surgical assault on presbyopia accelerated as Eyeonics developed the Crystalens, the first IOL with a pliable optic aimed at generating accommodation, a concept introduced a decade before by Spencer Thornton.33 A toric optic was developed by Staar Surgical; Pharmacia introduced Tecnis, the first spherical aberration-correcting IOL; and Alcon developed the first blue-light–filtering optic to provide macular protection. The once narrowly defined specialty of cataract and IOL surgery was exploding with new ideas and technologies. Smaller-incision IOLs were being designed that could be injected through <2-mm incisions. A host of surgeons, including Amar Agarwal, Jorge Alio, Richard Packard, Hiroshi Tsuneoka, Virgilio Centurion, Howard Fine, and Randy Olson, were exploring microincisional cataract surgery through 1.5-mm incisions by separating the sleeveless ultrasound tip from the irrigating chopper.
Refractive lens replacement and phakic implantation also were gradually earning a rightful place in anterior segment surgery. In the early 1980s, Franco Verzella from Italy initially removed the clear lens for extreme myopia, but surgeons were concerned about the incidence of retinal detachment in this group of high-risk eyes. Robert Osher performed the first clear lensectomy for hyperopia in 1985 and although the risk of retinal detachment was lower, these eyes were challenging both in surgery and in accurately selecting the IOL.34,35 John Gayton’s novel approach of using “piggyback” IOLs met with enthusiasm until interlenticular opacification emerged.36 AcriTec engineers from Germany identified a method of manufacturing lens power up to +60 diopters. Phakic implantation with IOLs fixated in the anterior chamber (Baikoff, Kelman, Choyce) and the posterior chamber (Fyodorov, Adatomed, PRL, Staar Surgical) were being developed. The iris-supported Verisyse (Artisan developed by Jan Worst) became the first phakic IOL approved in the United States.
The introduction of innovative adjunctive devices was able to improve the management of challenging cases. The capsular tension ring introduced independently by Tsutomu Hara37 and Toshiyuki Nagamoto38 in Japan was identified as a major weapon in managing zonular weakness by Ulrich Legler and Bernd Witschel of Germany.39 The CTR came to the United States in 1993,40 after which modifications by Robert Cionni,41 Iqbalk Ahmed and Alan Crandall,42 and Burkhard Dick were developed. Iris reconstruction had been primarily limited to suture techniques developed by Malcolm McCannel43 and later Steven Siepser.44 The prosthetic irides were introduced by German surgeons, Ranier Sundmacher45 and Volker Rasch,46 and brought to the United States by Kenneth Rosenthal and then Robert Osher in 1996.47 Although many devices had been developed to mechanically open the small pupil, it was the stretch technique developed by Luther Fry that greatly simplified these difficult cases.48 Improving visibility by staining the anterior capsule of the white cataract was introduced by Masayuki Horiguchi from Japan (ICG)49 and Gerritt RJ Melles from The Netherlands (Trypan Blue).50
It has been said that we can see further because we are standing on the shoulders of those who came before us. Nowhere is this truer than in the field of cataract surgery. We are able to provide our patients with painless surgery, rapid visual recovery, and little chance of complications because of the hard work and innovative thinking of these, and other, dedicated cataract surgeons.
PREOPERATIVE EVALUATION
EXAMINATION
Preoperative evaluation for cataract surgery begins by eliciting the chief complaint, which may be as general as blurred vision or more specific, such as trouble driving at night. In short, it states the reason for the patient’s visit and represents the juncture from which future clinical decisions derive. The history of present illness expands on the chief complaint to give a more complete understanding of the nature of the patient’s functional problems. Current documentation guidelines suggest that the history of present illness should include certain specific details such as the location, duration, timing, severity, and quality or context of symptoms, associated symptoms, and aggravating or alleviating factors.
The patient’s medical history should include all current medications, the reason for their use, and, in addition, information about current illnesses, previous illnesses, and previous surgeries. Any known drug allergies must be documented.
A complete review of systems may reveal information that patients may not have initially recalled about their health history. A form filled out by the patient before the appointment begins can be helpful. The physician must review this information and any uncertainties must be discussed with the patient.
Visual acuity testing is first performed either uncorrected or with the patient’s current eyeglasses. A manifest refraction determines the patient’s best possible spectacle-corrected vision. If the patient has glare complaints, glare testing can be performed using the patient’s manifest refraction. Near vision testing should also be checked because it may help the surgeon better understand the nature of the patient’s visual symptoms related to near tasks.
Evaluation of the pupils should not only determine the presence or absence of an afferent pupillary defect, but also pupil shape, size (before and after dilation), and reactivity. Photopic and scotopic pupil size is important when determining IOL size, and it may help the surgeon to select the implant style as well, especially when considering a multifocal IOL. A relative afferent pupillary defect indicates either optic neuropathy or diffuse retinal disease. The origin should be sought before considering cataract surgery, because it will likely have an impact on vision subsequently.
Similarly, evaluation of visual fields may alert the ophthalmologist to pathology unrelated to cataract. Routine confrontational visual field testing can disclose valuable information about the patient’s visual system. When confrontational testing results are abnormal, formal visual field testing is indicated.
Extraocular motility and ocular alignment always should be evaluated preoperatively. It is not uncommon to discover a small-angle heterotropia that might indicate amblyopia or alert the ophthalmologist to the possibility of postoperative diplopia. The surgeon thereby can better advise the patient.
Orbital anatomy should be evaluated and the presence of any abnormalities documented. It is best to investigate significant proptosis, lagophthalmus, epiphora, or other external abnormalities that might affect the surgical outcome before surgery. The surgical plan may need modification because of prominent superior orbital rims, marked adipose tissue prolapse, or other significant findings. Additionally, patients often comment on how noticeable wrinkles, drooped lids, or baggy lids appear after cataract surgery. It could be helpful to have documented such findings preoperatively.
Slit-lamp evaluation needs to be thorough, beginning with inspection of the lids and lashes. Blepharitis, trichiasis, ectropion, and other lid abnormalities may increase the risk for infection after cataract surgery and therefore should be addressed before surgery.
The quantity and quality of the tear film should be noted. Patients with significant keratitis sicca often can improve vision by rehabilitating their tear film, occasionally obviating the need for cataract surgery. Conversely, cataract surgery in the setting of an unstable ocular surface risks corneal melting, scarring, or ulceration. Untreated blepharitis may increase the risk of endophthalmitis.
Conjunctival abnormalities should be investigated carefully. Symblepharon formation, for example, may alert the surgeon to the possibility of pemphigoid, which is more likely to reactivate with cataract surgery if appropriate precautions have not been planned in advance. Filtering blebs or scarring from previous surgeries might encourage the surgeon to use a clear corneal approach. An area of limbal thinning might influence the surgeon’s decision about incision placement or affect planning for astigmatic reduction by limbal relaxing incisions.
Detailed evaluation of the cornea is essential, with attention given to each layer. Many corneal diseases are possible and many of these may affect the outcome of surgery or the decision to have cataract surgery. Corneal basement membrane dystrophies, including map-dot-fingerprint (MDF) dystrophy, or Salzmann’s nodules, for example, may cause irregular astigmatism and therefore could be a contributing factor to the patient’s visual complaints. Treating MDF before surgery may improve the patient’s vision sufficiently that cataract surgery may be avoided altogether. Additionally, keratometry readings are more accurate after treating significant MDF, reducing the risk of a postoperative refractive surprise. The presence of corneal guttae alerts the surgeon to the increased risk of corneal decompensation with surgery. The knowledge of such increased risk may affect the patient’s decision to proceed with surgery or not. The surgeon also may want to change technique to provide the cornea with supplemental protection during surgery.
The depth of the anterior chamber should be noted and any inflammation investigated. If slitlamp examination reveals normal anterior chamber depth, then gonioscopy is not necessary unless indicated for other reasons such as glaucoma, trauma, or for consideration of an anterior chamber IOL (ACIOL).
The iris is inspected for lesions, synechiae, sphincter tears, transillumination defects, abnormal vessels, and other abnormalities. The surgeon should carefully compare the color of the irides; it is easy to miss subtle heterochromia when looking through the slit-lamp at each eye independently. In addition, one must look for iridodonesis and keep in mind that both iridodonesis and phacodonesis often are more evident before dilation.
The crystalline lens, of course, is scrutinized, describing any opacities, their location, and their correlation to the recorded vision. Some opacities are best seen in retroillumination and should be described as such. Careful inspection is necessary to visualize trace amounts of pseudoexfoliative material on the anterior lens capsule. Some patients may have anteriorly placed zonules that might compromise a wide capsulorrhexis.51 Cortical changes typically occur in either spokes, plates, or both. They may invade or cross completely over the entrance pupil from one or more quadrants. Cortical spokes are more commonly anterior but occasionally may involve the posterior aspect of the lens as well.
Nuclear cataractous changes manifest in three general patterns: nuclear color, nuclear opacity, and intralenticular blisters. Color and opacity are best assessed by biomicroscopy with a thin, bright slit beam and should be graded separately.52 Blisters are better visualized by retroillumination. Sometimes nuclear changes are somewhat diffuse, whereas other cataracts display prominent opacity only in the most central fetal nucleus. These findings should be accordingly described.
Posterior subcapsular cataractous changes may be fine or coarse, focal or diffuse, and axial or peripheral. Axial posterior subcapsular cataractous changes are, not surprisingly, more symptomatic in most patients. Even subtle changes on biomicroscopy may induce disabling glare.
The ophthalmologist should take care to evaluate for phacodonesis, zonular dialysis, and lens subluxation, especially with a history of trauma or other factors that make such findings more likely, such as Marfan’s syndrome or pseudoexfoliation. These findings indicate that special techniques, devices, and instrumentation may be required for surgery. A subtle gap between the iris and anterior lens capsule may indicate undiagnosed zonular weakness.
The posterior segment is examined by indirect ophthalmoscopy, biomicroscopy, or direct ophthalmoscopy. When evaluating the optic nerve head, the ophthalmologist should direct attention to the cup:disc ratio, health of the neural tissue, and peripapillary anatomy. Stereomicroscopic evaluation of each macula is performed while carefully looking for subtle epiretinal membranes, microaneurysms, or other abnormalities.
The retinal periphery is best examined using the indirect ophthalmoscope. Choroidal nevi, retinal tears, and other abnormalities detected are documented and treated, if necessary. Some retinal abnormalities, such as diabetic macular edema and retinal tears, are best treated and given time to heal before proceeding with cataract surgery.
SPECIAL PREOPERATIVE TESTING
When evaluating a patient before cataract surgery, several special tests may be undertaken, which fall into three broad categories. First, some tests seek to correlate the patient’s complaints and functional problems with measurable parameters; other tests help give prognostic information about the potential degree of visual recovery; finally, still further tests guide the ophthalmologist in planning the surgery.
SPECIAL MEASUREMENTS OF VISION
Preoperative measurement of vision is meant to determine the patient’s current state of visual function. Snellen acuity is routinely tested on all patients as part of their preoperative evaluation. This usually is performed by having the patient read a standardized chart in a darkened room. Although the Snellen acuity scale is the most ubiquitous measure of vision, it measures only one tiny aspect of visual function. Many patients may be profoundly functionally impaired by their degree of visual disability, yet may test surprisingly well measuring Snellen acuity in a darkened room. In these cases, it is incumbent on the ophthalmologist to seek to better understand and document the patient’s problems by performing additional testing.
Many patients are most bothered by cataract-induced glare. For these patients, acuity testing under glare situations is indicated. There are several methods to assess visual acuity reduction by glare. The choice of method is often best dictated by the patient’s history. If a patient complains of glare problems in the supermarket, or other uniformly illuminated environment, the brightness acuity test can be performed (Mentor Ophthalmics). For this test, the specially illuminated handpiece is held in front of the tested eye using best spectacle correction (Fig. 1). The Snellen acuity is rechecked and can be recorded on each of three light settings.
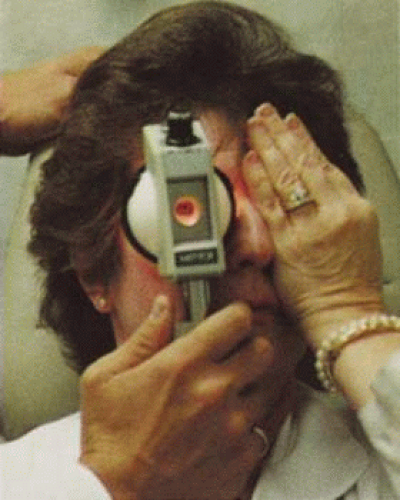 Fig. 1. Brightness acuity test. |
Patients who complain of glare from point sources of light, such as oncoming headlights or bright sunshine, may be best evaluated by a different form of glare testing. To simulate the environment of the patients’ symptoms, Snellen acuity is measured while directing a point source of light obliquely toward the eye outside their best spectacle correction or outside of a phoropter dialed in with their best manifest refraction (Fig. 2).
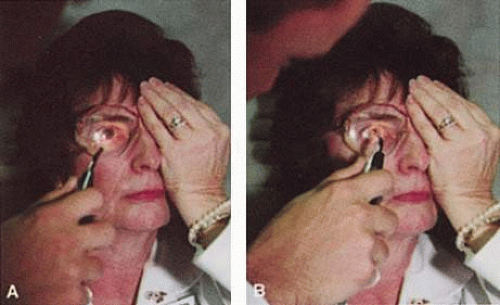 Fig. 2. The correct method for performing a “point light source” glare test. A. Transilluminator is directed toward the eye at an angle. B. Shining the transilluminator from directly in front of the eye is not a valid method for testing glare because it underestimates the glare acuity. |
Still other patients’ problems may center on difficulty with reading, seeing street signs, or distinguishing fine patterns. In these individuals, the complaints are related more to contrast; therefore, contrast testing is most appropriate. There are a number of ways to assess the effect of contrast on vision. Regan’s sine wave gradients have been used frequently for research purposes and are available in some settings. Various commercial devices are now available to measure visual acuity in different contrast settings and each has its relative merits and detractions. The authors have found the Baylor Visual Acuity Tester (BVAT) monitor (Mentor Ophthalmics) testing of contrast to correlate well with patients’ complaints and its simplicity is appealing to both patients and technical staff.
In rare instances, patients’ complaints may be primarily related to distinguishing colors. Although patients frequently remark about their dramatic improvement in color perception after cataract surgery, there are no convenient methods to document diminished color perception preoperatively. This underscores the importance of correlating patients’ complaints with the biomicroscopic examination and the degree of nuclear color change.
PROGNOSTIC TESTS
Physicians often order special tests to help determine a patient’s visual potential. Some of these tests are acuity specific. These can be particularly helpful in guiding patients who may have comorbid ocular conditions. Some devices have been designed to project a Snellen chart through the clearest area of the cataractous lens to assess retinal acuity potential such as the potential acuity meter. Studies also have shown a good predictive value by checking vision with a brightly illuminated near card.53 Of course, this can be performed with no additional office equipment. Various other commercial devices, including interferometry and various different pinhole and illumination device combinations, are available.
These approaches are not possible for patients with mature cataracts. Some more general, nonspecific prognostic tests can be performed. If a patient is able to identify the colors of projected lights, this usually indicates that some cone-mediated macular function is present.
Blue field endoscopy also may indicate some macular function. This test is performed by projecting a blue light into the eye. The patient may report seeing small round specks moving around in the vision. These specks correspond to white blood cells passing through the perifoveal capillaries.
The Purkinje phenomenon is tested easily by rapidly wiggling a transilluminator directed toward the globe through the lower lid in a darkened room. If the patient reports a pattern of crooked lines or branches, then he or she is seeing the shadows cast by the retinal blood vessels, indicating that the posterior pole is attached and functioning to at least some degree. Although positive results from the test are encouraging, some patients may still have limited vision after surgery; similarly, some rare patients may test negatively on all these tests and still recover good vision.
Diagnostic Studies
Several diagnostic studies provide information that supplements the historical and clinical data obtained by the surgeon. This information enables proper preoperative patient consultation and surgical planning. This section outlines many preoperative tests used for cataract patients.
A-SCAN BIOMETRY.
Accurate axial length measurement is critical to determine the correct power of the implant lens for the desired refractive result. A-scan biometry is imperative in any patient undergoing cataract surgery. Both contact (applanation) and immersion varieties of A-scan ultrasound units are commercially available. With applanation biometry, a hand-held or slit-lamp mounted probe is gently touched to the corneal surface along the visual axis. Contact A-scans are user dependent and sometimes the authors adjust the surgeon-specific IOL A-constant depending on which ultrasonographer has performed the scan. Nonetheless, outstanding refractive outcomes have been achieved, and the authors have been satisfied with the contact applanation technique.
With an immersion probe, a water bath around the eye acts as the medium to conduct sound waves. Although there is no direct contact of the probe with the globe, the water and water bath must, of course, remain in contact with the ocular surface and periorbita. Immersion scans may reduce interobserver variations but are less comfortable and less convenient for patients.
A-scan biometry is particularly challenging in eyes containing an oil fill. In this instance laser biometry is still able to achieve excellent measures.
LASER PARTIAL COHERENCE OPTICAL BIOMETRY.
Although ultrasound requires continuous contact with media that conduct sound waves, laser light passes easily through any clear media, including air, making this a truly noncontact or “no touch” test. Furthermore, the speed of light is not appreciably different in the clear media of the eye and thus excellent, reliable measures can be achieved in eyes containing intraocular lenses, regardless of type and eyes with oil fills within the vitreous cavity. Although some calculation adjustments can be made depending on the pseudophakic status, the differences among implant material are not appreciable different from a practical clinical perspective. Currently, the only commercially available laser biometry device is the IOLMaster (Zeiss). The measurements obtained by the IOLMaster device are extremely reliable, reproducible, and seem to be relatively technician- and observer-independent.54,55 This device also can measure keratometry, optical anterior chamber depth measurements, and “white-to-white” measurements in an automated fashion. Because it relies on the passage of laser light through the ocular media, this instrument is unable to obtain measurements in cases where the media prevent laser light passage; for example, white cataracts, axial posterior subcapsular cataracts, or corneal scarring.
B-SCAN ULTRASOUND.
A mature cataract precludes visualization of the fundus. A B-scan ultrasonographic examination provides a real-time, two-dimensional (2D), cross-sectional image of the globe along the marked axis of the probe (Fig. 3). Cataracts are more common in patients with chronic retinal detachment, prior trauma, or intraocular tumors; therefore, a B-scan study is helpful in excluding structural posterior segment pathology before surgery on a mature cataract. Although a negative result to B-scan evaluation is reassuring, the surgeon should remember that it does not predict postoperative visual outcome. The B-scan can be thought of as a picture of Cincinnati from an airplane; the office buildings may all be standing, but you cannot tell whether the people in them are working.
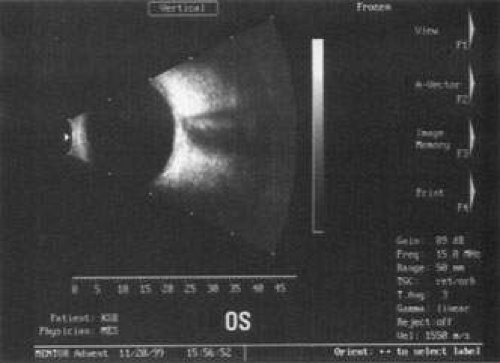 Fig. 3. This B-scan ultrasound shows a normal looking posterior pole, without retinal detachment or intraocular mass. The vitreous cavity is echo lucent. |
ENDOTHELIAL CELL COUNT.
Although slit-lamp examination can give the ophthalmologist an excellent estimate of endothelial health, sometimes a formal assessment of the corneal endothelial cell density is helpful (Fig. 4). This information is most likely to be helpful in advising patients who may be at greater risk of postoperative corneal decompensation. Specifically, patients with cornea guttata, previous ocular surgery, history of blunt ocular injury,56 exfoliation syndrome,57 iridocorneal-endothelial syndromes,58 or a history of glaucoma59 are known to have reduced endothelial cell counts. Patients with a history of acute angle closure are at particular risk because each episode of elevated intraocular pressure can damage endothelial cells.60
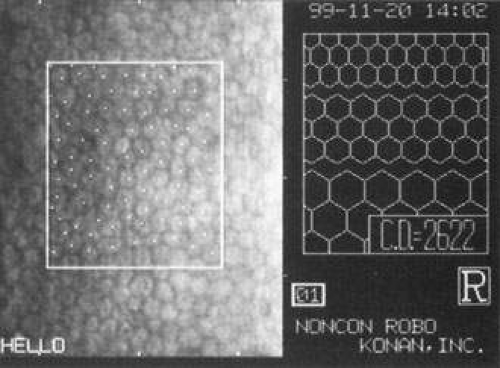 Fig. 4. A noncontact endothelial cell photograph demonstrates a normal cell mosaic and density. The cell count is calculated by identifying those cells within the box and touching two of the four adjacent edges. |
There are qualitative and quantitative methods for endothelial cell evaluation. Cell density can be measured directly with an endothelial cell camera. The surgeon also should view the photograph and qualitatively estimate the regularity of the endothelial cell mosaic. Some instruments calculate a coefficient of variability and percent of hexagonal cells.
When an endothelial cell camera is not available, qualitative assessment of count and cell morphology can be accomplished at the slit-lamp using a technique called specular reflection.61 The ophthalmologist focuses a narrow parallelepiped on the corneal epithelium, directing the beam at the periapical cornea from a 45-degree angle. The slit beam is moved slowly from side to side until the bright corneal reflex strikes the examiner’s view from the epithelial surface reflection (first Purkinje-Sanson image). On high magnification, the examiner should focus on the endothelial surface just next to the bright reflex. The image of the endothelial mosaic will come into view. The surgeon can make a qualitative assessment of the cell density and degree of regularity. With practice, these estimates can be surprisingly accurate.
The implications of a reduced endothelial cell count are primarily prognostic and can provide the surgeon with more information to help counsel the patient about the risk of corneal decompensation with cataract surgery. Gentle phacoemulsification without triple procedure is recommended when cornea is clear and compact, given that a significant number of patients may be able to avoid a corneal transplant despite uncountable cell densities. However, these patients should be advised that they may be at an increased risk of requiring a corneal transplant.
PACHYMETRY.
Ultrasonic pachymetry measures central corneal thickness. When endothelial function is tenuous, corneal thickness begins to increase gradually, indicating subclinical stromal edema. Similar to endothelial cell count measurements, pachymetry is primarily of prognostic value.
Surgical planning also may differ for the patient with a compromised endothelium. In this case, use a more highly dispersive viscoelastic and minimal amounts of infusional fluids during surgery. When the degree of compromise is severe, additional dispersive viscoelastic material can be added periodically during the phacoemulsification. Because corneal transplant is a distinct possibility, such patients are not good candidates for a multifocal implant.
CORNEAL TOPOGRAPHY.
Computed corneal topography may be helpful from both a diagnostic perspective and as an aid to preoperative surgical planning. The diagnostic value of corneal topography is most obvious when keratoconus or irregular astigmatism is suspected. In cases with irregular astigmatism, superficial keratectomy or excimer phototherapeutic keratectomy may be indicated before cataract surgery, particularly when the relevant pathology precludes accurate keratometry.
In some cases, corneal topography is an invaluable aid in surgical planning as well. In patients with high astigmatism, the topography can indicate the best meridian for placement of limbal relaxing incisions (Fig. 5). The topography also may be used to confirm the keratometric measurements.
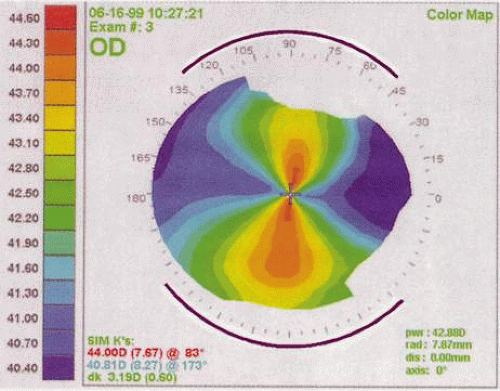 Fig. 5. Corneal topography demonstrates with-the-rule astigmatism. The purple lines drawn suggest the pattern for limbal relaxing incisions. |
ULTRASOUND BIOMICROSCOPY.
The ultrasound biomicroscope is a specialized, high-resolution form of 2D ultrasound, similar to the B-scan discussed in the preceding. An ultrasound biomicroscope study may be helpful to the cataract surgeon in cases of mature cataract when retroiridial, anterior segment pathology is suspected. Currently, the ultrasound biomicroscope instrument is expensive and not widely available, and has uncommon indications.
ANESTHESIA TECHNIQUES
Many approaches for ocular anesthesia achieve satisfactory results. Historically, topical anesthesia with cocaine was the first approach. As general anesthetic techniques became more widely available, topical cocaine use for eye surgery was abandoned. Later, orbital blocks became popular to reduce systemic risks associated with general anesthesia. More recently, with the advent of small incision phacoemulsification, many surgeons have returned to topical anesthesia, although with a much higher safety profile than in the days of intracapsular surgery.
GENERAL ENDOTRACHEAL ANESTHESIA
Although general anesthesia is an uncommon choice for today’s cataract procedures, in rare instances it may be necessary. Even though improvements in anesthesia techniques and agents have improved the safety of general anesthesia, the risks for patients with other medical conditions may be significant. Although rare, idiosyncratic reactions can still result in dire consequences or death, even in previously healthy patients. This sobering knowledge, combined with the additional patient and physician inconveniences of general anesthesia, makes it an uncommon choice for cataract surgery. Certainly, general anesthesia may be considered when a patient is unable to hold steady or cooperate with regional anesthesia. This is likely to be more commonly required in young children or people with significant cognitive disabilities. Occasionally, general anesthesia is required for patients with neurologic conditions such as high amplitude resting head tremor or spasmodic torticollis.
ORBITAL BLOCKS
The purpose of an orbital block is to provide ocular akinesia and anesthesia. Different anesthetic agents can be administered. Relatively short-acting 1% lidocaine offers a more rapid recovery of vision with less diplopia and lower risk of muscle toxicity, although it may not be appropriate for an anticipated lengthy case. Bupivacaine or lidocaine-bupivacaine combinations induce a longer anesthetic effect, although bupivacaine is reported to have a higher incidence of muscle toxicity with resultant diplopia or ptosis.62,63,64,65 The addition of hyaluronidase to the injection mixture improves the anesthetic’s ability to spread through the orbital tissues. Agents containing epinephrine increase the longevity of anesthetic action but rarely induce central retinal artery occlusion.66 Varieties of block styles are used with mild variations in effectiveness and complication profiles.
Retrobulbar Block
Retrobulbar blocks were among the earliest of orbital block techniques and have stood the test of time. Although there are many approaches to block administration, each technique intends delivery of the anesthetic medication into the intraconal space. These blocks are highly effective (about 95%) in achieving adequate ocular akinesia and anesthesia. Potential complications include retrobulbar hemorrhage,67 globe penetration,68,69 optic nerve sheath hemorrhage, extraocular muscle toxicity with persistent diplopia, and, rarely, brainstem anesthesia. Visualization of the globe is improved when using a transconjunctival approach (Fig. 6) or when the skin is indented with a cotton-tipped applicator (Fig. 7), making globe perforation less likely.
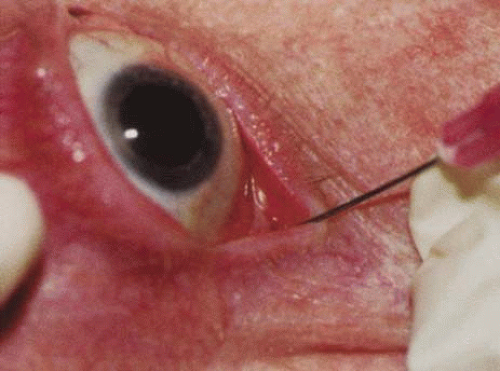 Fig. 6. Retrobulbar block using a transconjunctival approach. |
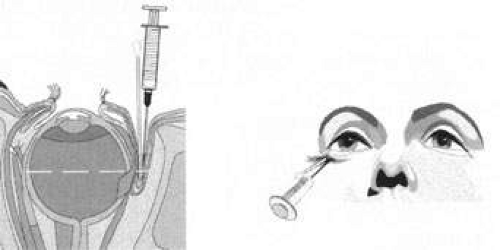 Fig. 7. The skin is indented with a sterile cotton-tipped applicator until it is past the equator of the globe, thereby reducing the risk of globe perforation when the needle is inserted. |
Peribulbar Block
A peribulbar block differs from the retrobulbar approach by delivering the anesthetic dose to the extraconal peribulbar space. The medication then spreads into the muscle cone, aided by a hyaluronidase enzyme, facilitating diffusion through the orbital tissues. The speed of onset is typically a few minutes longer than retrobulbar blocks, and typically a higher volume of anesthetic agent is given. This approach is slightly less effective than the retrobulbar block. Yet, by virtue of staying outside the muscle cone, some potential complications are less likely and others less severe. The sequelae of retrobulbar hemorrhage are less ominous when it occurs outside the muscle cone, as optic nerve compression is less likely. Direct optic nerve or nerve sheath injury is virtually eradicated. As with retrobulbar injections, using a transconjunctival approach or indenting the skin with a cotton-tipped applicator before peribulbar injection, improves visualization of the globe and decreases the likelihood of globe perforation.
PARABULBAR ANESTHESIA
Various approaches can instill anesthetic into the subconjunctival or subtenon space using either a needle or a posteriorly directed blunt cannula.70 Parabulbar anesthetics are fairly effective for anesthesia, although they generally achieve less than maximal akinesia. Ballooning of the conjunctiva may cause fluid to build up around the limbus, creating a fluid meniscus lens, markedly limiting surgical visualization (Fig. 8). A posteriorly directed cannula in the parabulbar space could disturb a vortex vein. These injections also may induce unsightly subconjunctival hemorrhage. The authors reserve parabulbar anesthetic techniques primarily for augmentation of anesthesia when an initial anesthetic has either worn off or proved ineffective.
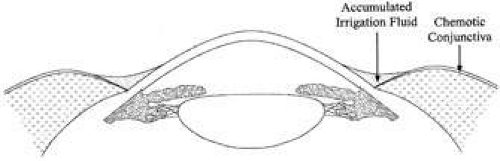 Fig. 8. Chemosis can cause pooling of the irrigation fluid, which creates a negative meniscus lens, inhibits the view, and reduces stereopsis. |
LID BLOCKS
Some surgeons combine orbital block with facial nerve block. The main indication for an eyelid block is to limit the patient’s forced lid closure against the speculum. Such squeezing can markedly increase posterior pressure and cause anterior chamber collapse. Lid blocks usually are applied only when orbital blocks are given, although occasionally they may be indicated in a case under topical anesthesia when the patient has blepharospasm. A lower lid block can be achieved easily by injecting an additional 1 or 2 ml of anesthetic into the lower lid when withdrawing the needle from an orbital injection. Typically this is satisfactory in most cases, because an upper lid, unopposed by lower lid tone, induces almost negligible effects on the globe.
If more complete facial nerve block is required, an Atkins, Van Lint, modified Van Lint, or Nadbath block may be administered. The surgeon should be reminded that increasing degrees of facial nerve block may have some undesirable effects. Fibers from the lower divisions of cranial nerve VII serving the lower face also may be affected by an eyelid block, producing temporary facial asymmetry and slurred speech, which patients may find frustrating. Transcutaneous facial nerve injections also may cause unappealing facial ecchymosis as well.
TOPICAL ANESTHESIA
With the advent of self-sealing wounds and closed-chamber systems for phacoemulsification, the need for absolute ocular akinesia has diminished. Accordingly, topical anesthesia for cataract surgery has become increasingly more common. In topical anesthesia techniques, the patient receives several drops of a topical anesthetic agent, inducing anesthesia of the ocular surface and allowing the initial incision to occur painlessly. During the surgery, the patients may detect some sensations of pressure or fullness and should be told to expect this at any step in which the globe is pressurized. The patient should be counseled in advance that he or she may feel pressure, but not pain. To explain this to the apprehensive patient, the authors sometimes shake the patient’s hand in the office and ask “Can you feel this?” Then, after the patient responds “Yes,” inquire “Does that hurt?” The patient invariably responds, “Of course not.” With topical anesthesia, there is no induced amaurosis and patients may see some steps in the surgery. For example, hydrodissection is associated with a blurring of the distinct image of the microscope light. Continuous patient communication may ease or pre-empt anxiety. Some surgeons instill intracameral preservative-free 1% lidocaine to blunt patients’ sensations further. Studies demonstrate different results in assessing safety and efficacy.71,72,73,74 Topical anesthesia techniques eliminate the inherent risks of orbital injections and offer rapid visual recovery. Additionally, topical anesthesia is anticoagulant friendly for patients on warfarin (Coumadin) and other blood thinners. However, topical anesthesia is not suitable for all patients or all surgeons.
Selecting the appropriate patient for topical anesthesia is paramount to both the surgeon’s and the patient’s satisfaction. This determination should be made during the preoperative patient examination. Extremely photosensitive patients or patients who are noted to be “squeezers” in the office might be better suited to regional block. Communication with the patient during surgery is a vital component of the topical anesthetic experience. Accordingly, patients with whom the surgeon cannot easily communicate are not good candidates. For patients who are hard of hearing or patients who do not speak the surgeon’s language, an orbital block should be considered. Occasionally, the cataract surgeon encounters patients with disorders of ocular motility that preclude effective topical anesthetic approaches. Certainly, patients with nystagmus require the akinesia of an orbital block. Moreover those patients with large angle strabismus may have difficulty maintaining their gaze while their contralateral eye is unable to fixate.
OPERATIVE MYDRIASIS
One can achieve an adequate pupillary size for routine cataract surgery by a number of different mechanisms. Tradition has favored administration of frequent mydriatic drops on the patient’s arrival to the surgical facility. These may include tropicamide, phenylephrine, cyclopentolate, hyoscine, and perhaps a nonsteroidal agent for reducing intraoperative miosis. Although this tried and true approach is still highly effective, other more convenient options have flourished recently. Some centers have patients administer mydriatic drops before arrival, whereas other surgeons have incorporated mydriatic drops into a Xylocaine gel, applied at arrival to the facility in a single dose. Some investigators have instilled miotics into the anterior chamber, while others have demonstrated effective mydriasis by instillation of intraocular, nonpreserved Xylocaine alone.75
INFECTION PROPHYLAXIS
Although infectious endophthalmitis following cataract surgery is now rare, its occurrence can be so devastating that its prevention is of paramount importance.76 Therefore patients should receive appropriate prophylaxis. Patients with blepharitis should be treated with eyelid hygiene measures. In the operating room, a drop of topical povidone-iodine paint instilled at the beginning of surgical preparation has been shown to reduce bacterial flora significantly and decrease the incidence of endophthalmitis.77,78 One survey79 also has shown a correlation between use of preoperative topical povidone-iodine and decreased incidence of endophthalmitis.80 Although there appears to be no benefit to trimming the eyelashes, the authors recommend isolating the lashes with a sterile plastic adhesive drape or a Steri-Strip. Antibiotic use is discussed in detail in the following paragraphs.
ANTIBIOTIC COVERAGE
Despite significant and widespread debates, the use and best method of administration of antibiotics in cataract surgery remains controversial. Traditionally, subconjunctival antibiotic injections were given at the completion of cataract surgery. As topical anesthesia became more popular, surgeons sought alternatives to painful subconjunctival injections. Several regimens of topical, infusional, and intracameral antibiotic agents have since become popular, although there may be a good rationale for avoiding some of these approaches.
It is difficult to determine the best antibiotic coverage choice with existing imperfect and incomplete data. A rational approach should examine the purposes of using an antibiotic, the relative likelihood of achieving those goals, and the possibility of unintended, undesirable effects of each antibiotic choice.
There are essentially two goals of perioperative antibiotic use: prophylaxis of endophthalmitis and avoiding bacterial ulcerative keratitis. Endophthalmitis prophylaxis receives the greatest attention because of the severity of its consequences. Several antibiotic regimens in current practice are reviewed here, stating their strengths and weaknesses.
PREOPERATIVE TOPICAL ANTIBIOTICS
Preoperative topical antibiotic drops certainly can reduce the colony counts on the ocular surface, provided that they are given for a sufficient time in advance of surgery to effect the conjunctival flora. Some believe that preoperative drops create a selection bias for resistant, aggressive organisms, even though there is no evidence of this.81 With sound arguments on either side and data lacking, preoperative drops seem reasonable but not mandated. Many agents address a broad spectrum of gram-positive and -negative organisms. The surgeon should be aware of kill curve data for the selected agent to ensure that the preoperative dosing regimen begins far enough in advance to have a meaningful effect.
PREOPERATIVE ORAL ANTIBIOTICS
There is a wide body of general surgery literature indicating a diminished risk of wound infection with preoperative systemic antibiotics. Some ophthalmic surgeons have theorized that the same philosophies should apply to ophthalmology and the prophylaxis of endophthalmitis. They maintain that a preoperative dose of a broad-spectrum oral antibiotic that produces therapeutic levels in the vitreous cavity should be effective in preventing an errant organism that finds its way into the vitreous gel from colonizing. Although this theory is appealing, no data exist yet on safety or efficacy. Surgeons who consider this method of therapy also should consider the potential for serious idiosyncratic reactions with systemic antibiotics. Remember that some 500 people die in the United States each year from penicillin-induced anaphylaxis,82 1 in 40,000 who receive chloramphenicol can die of aplastic anemia,83,84 and trovafloxacin mesylate, an oral, broad-spectrum fluoroquinolone with a previously presumed high safety profile, has been associated with an infrequent incidence of liver failure.85
ANTIBIOTICS IN THE IRRIGATING SOLUTION
During the past several years, it has become increasingly popular to place antibiotics in the irrigating solution. Although informal surveys seem to report a decreased incidence of endophthalmitis, from the microbiologic perspective, infusional antibiotics are not entirely rational.86 The concentrations of antibiotics that are widely used are not bacteriocidal. Furthermore, such dilute solutions may create a selection bias for resistant organisms on the conjunctival surface and in the operating room. Dilutional errors in preparing the antibiotic in the infusate can have devastating visual sequelae from retinal toxicity.
INTRACAMERAL ANTIBIOTIC INJECTION
In response to the homeopathic dosage criticisms of infusional antibiotics, some surgeons have opted to place a therapeutic antibiotic dose into the anterior chamber at the completion of surgery. Typically, surgeons administer half the dose used for intravitreal injection. This approach makes some theoretical therapeutic sense, given that the antibiotic is present in sufficient concentration to kill introduced organisms. Because the antibiotic-containing fluid does not bathe the ocular surface or access the operating room surfaces, selection of resistant organisms might be less likely. Critics of routine intracameral antibiotics cite the lack of safety and efficacy data and point out that although the administered antibiotic dose may be bacteriocidal, the agent is rapidly diluted by aqueous turnover. Dilutional errors could induce severe retinal or corneal endothelial damage. Insufficient available peer review data preclude widespread recommendations for this mode of endophthalmitis prophylaxis.
SUBCONJUNCTIVAL ANTIBIOTICS
Historically, subconjunctival antibiotic injection has been the mainstay of endophthalmitis prophylaxis. The safety profile is fairly broad, except for aminoglycosides, which have been reported to access the anterior chamber after injection to cause retinal toxicity.87
POSTOPERATIVE TOPICAL ANTIBIOTICS
Topical antibiotic drops are used almost uniformly after cataract surgery. Motivation for their use has been to reduce the risk of endophthalmitis. In one rabbit study, topical 0.5% moxifloxacin was shown to prevent endophthalmitis when an inoculum was placed into the anterior chamber, whereas the control animals treated only with normal saline developed infectious endophthalmitis.88 However, topical agents do have an important role in the prophylaxis of bacterial keratitis, because it may take several days for the corneal epithelial barrier to regain its integrity after even flawless clear corneal surgery. The authors advocate the use of topical antibiotics postoperatively.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


