Fig. 20.1
Retinography of a patient with non-proliferative diabetic retinopathy and diffuse macular edema (dotted line). Hard exudates (asterisks) and microaneurysms (arrows) are present in the paramacular area
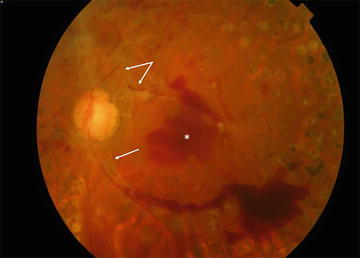
Fig. 20.2
Retinography of a patient with proliferative diabetic retinopathy. There is a macular hemorrhage (asterisk) and neovascular tissue (arrow) on the optic nerve
For any patient with diagnosed DR, fluorescein angiography should be considered to assess the presence of retinal neovascularization, peripheral ischemia, or macular edema. Because the detection of diabetic macular edema with conventional ophthalmoscopy in cataract patients may be complicated, optical coherence tomography (OCT) provides a rapid noninvasive test that can more accurately identify possible macular neuroepithelial degeneration and the presence of macular edema (Figs. 20.3 and 20.4). OCT also enables the detection of other macular alterations in DM patients, such as vitreomacular traction syndrome or the epiretinal membrane. However, any of these alterations could represent a contraindication for cataract surgery and may influence surgical technique choice.
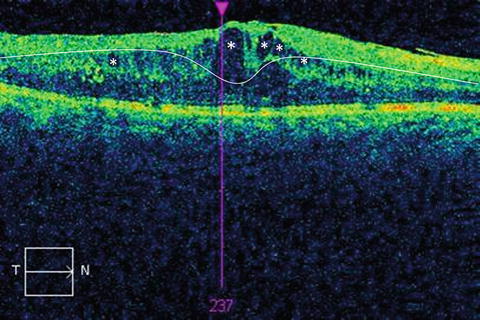
Fig. 20.3
Optical coherence tomography axial macular scan of a patient with diabetic macular edema showing intraretinal cysts (asterisk) and increased macular thickness. White line shows normal macular thickness and shape
Fig. 20.4
Optical coherence tomography macular map of a patient with diabetic macular edema. Each of the colors that appear in the macular map represent a certain retinal thickness
20.4 Preoperative Treatment
Poor prognoses after cataract interventions on diabetic patients are due to postsurgical eye complications from this disease [15, 21]. To avoid such complications, it is important, whenever possible, to treat the ocular alterations (mainly retinal) associated with DM. The main therapeutic tools available include laser photocoagulation and the intravitreal administration of anti-VEGF drugs.
The prognosis of patients with active DR undergoing cataract treatment improves significantly with previous laser photocoagulation treatment [22]. An analysis of previous studies comparing the long-term visual outcomes between treated and untreated patients indicates that it is advisable to conduct appropriate laser treatment of DR before performing cataract surgery [4, 11].
Potent drugs that are currently available can help to stop the progression of DR when administered to the vitreous humor of the patient. Such drugs (Avastín®, Eylea®, Lucentis®, and triamcinolone acetonide) can also be combined with laser treatment to obtain better control of DR before cataract surgery [23].
20.5 Surgical Procedure and Additional Treatments
Once cataract treatment in diabetic patients has been indicated, one of the following three situations will be found:
20.5.1 Patient with Cataracts Without Significant Diabetic Retinopathy
Patients with a healthy retina that require only cataract treatment should receive conventional cataract surgery similar to nondiabetic patients.
20.5.2 Cataracts and Diabetic Macular Edema
Macular edema is the accumulation of fluid in the macular neuroepithelium and is the main cause of loss of vision in patients under 50 years of age in developed countries (Figs. 20.1, 20.2, and 20.4). Fluorescein angiography can be used to detect macular fluid extravasation. Although the opacity resulting from cataracts may hinder the detection of macular thickening during conventional funduscopic examination, the OCT approach permits an accurate measure of such thickening. Various studies have shown a potential relationship between cataract surgery in diabetic patients and postsurgical macular edema, for which some authors have recommended performing cataract surgery only when the condition is advanced and not operating on patients with an initial cataract to avoid the risk of macular edema [14, 16]. However, other authors have suggested carrying out the surgery before the macular edema is detected given that functional recovery after surgery is less successful when it is present [12, 20]. The ideal approach would be to definitively treat the macular edema before cataract surgery; however, in many cases, this condition is recurrent, and treatment may take months or years using combined laser and intravitreal anti-VEGF injection therapies [24].
Currently, with the existence of different drugs that show efficacy in the treatment of macular edema, its presence does not modify the indications for cataract surgery, and this condition can be treated simultaneously via intravitreal anti-VEGF injection and cataract surgery [25].
20.5.3 Cataracts and Vitreoretinal Alterations That Require Surgical Treatment
In cases where cataracts are diagnosed together with other alterations that require treatment, the typical approach is to combine both procedures. The most common surgical technique in these cases is phacoemulsification with a standard lens implant. However, we must consider that any retinal surgery (vitrectomy) performed in a patient over 50 years of age will cause lens opacification. As a result, when patients of this age group require vitrectomy, lens extraction is carried out during the same surgical procedure even though no significant cataract is present at that moment; this approach avoids a second operation a few months later when the cataract would develop. The cataract extraction surgical technique in these patients is the same as in patients without DM (phacoemulsification with standard lens implant), with the exception of patients with anterior tractional retinal detachment or a high degree of severity of the retinopathy [26].
The main vitreoretinal alterations that may accompany cataracts in diabetic patients and require vitrectomy include vitreomacular traction syndrome, epiretinal membrane, vitreous hemorrhage, and tractional retinal detachment.
Vitreomacular traction syndrome is a disease caused by the abnormal adherence between the vitreous and the retina. Specifically, the macula is pulled by the vitreous layer adhered to it, which leads to structural alterations that are frequent in diabetic patients [27].
An epiretinal membrane displays an abnormal growth of cells over the macular surface, which forms a tissue layer that can create traction over the macula, thereby altering its structure and producing vision loss [28].
Vitreous hemorrhage is a frequent complication of proliferative DR, which generally indicates active disease.
Tractional retinal detachment is typically a manifestation of advanced proliferative DR and consists of the separation of the retinal neuroepithelium and the retinal pigmented epithelium due to traction from the fibrous tissue.
20.6 Surgical Technique
As discussed previously, the surgical treatment of cataracts in diabetic patients is, with the exception of the abovementioned cases, similar to that of non-diabetic patients [31]. In this section, we briefly describe the standard cataract surgical technique.
The cataract procedure is performed in most situations using only topical anesthesia. After the instillation of a few drops of anesthetic, the conjunctival sac, the ocular surface, and the periocular region are cleaned with povidone-iodine. Then, the eyelashes are isolated from the surgical field using sterile plastic material.
The first step of the operation consists of a corneal incision of approximately 1.8–2.4 mm, through which the entire procedure will be carried out. Secondly, an opening of the anterior capsule of the lens is formed, through which saline is injected for hyperhydration and rotation of the lens (hydrodissection and hydrodelamination). Then, the phacoemulsifier is introduced through the incision and the anterior capsule of the lens. This device emits ultrasound energy to produce liquefaction of the lens, which is aspirated. Once the lens capsule is empty, an intraocular lens is introduced into the crystalline sac.
As mentioned previously, the inflammatory reaction resulting from cataract surgery may favor the progression of DR, and it is therefore important to perform this operation with the least possible trauma [32]. Thus, it is essential to shorten surgical time and minimize the energy of phacoemulsification especially in medium-hard cataracts. Cataract surgery in a hypermature lens will involve a considerable increase in the surgical aggression delivered to the eye, with an increase in postoperative inflammation and a higher risk for progression of DR or other complications.
Another peculiarity of cataract surgery in DM patients is their higher incidence of retraction of the lens capsule after the operation (Fig. 20.5) [33]. The proliferation of remaining epithelial cells from the lens and the inflammatory environment are two factors that may play an important role in increasing the opacity and postsurgical contraction of the crystalline sac common in such patients [34, 35].
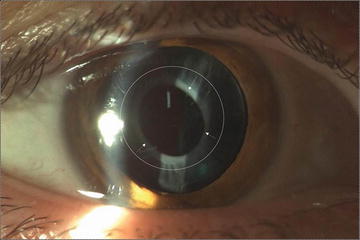
Fig. 20.5
Anterior segment image of a patient with opacification and retraction of the anterior lens capsule (anterior capsule phimosis). The dotted line shows the original perimeter of the capsulorhexis performed during surgery. This retraction (arrows) may be difficult for future retinal examinations or treatments
The specific aspects that must be taken into account when performing cataract surgery in a diabetic patient are the following [36]:
6.1
Surgical trauma should be avoided. As described earlier, surgical trauma may favor macular edema; it can accelerate the course of DR and favor contraction and opacification of the lens capsule. Additionally, the corneal endothelium receives greater damage in diabetic patients and demonstrates a poor recovery of postoperative edema following traumatic surgery [37].
6.2
Corneal epithelium protection. The ocular surface is altered in diabetic patients, which leads to poor healing of the surgical wound and an increase in the incidence of postoperative epithelial erosions [38]. In some patients, these erosions may become complicated and develop into true persistent epithelial defects with a difficult resolution (Fig. 20.6). To ensure protection of the corneal epithelium, hydration of the surface of the eye during surgery, avoiding traumatic maneuvers and applying topical ointments in cases of intraoperative de-epithelization are important. This is especially important for the combined treatment of cataracts and vitrectomy [39].
6.3




Iris management. There is a higher incidence of poor dilation or intraoperative miosis in diabetic patients [40]. In advanced retinopathies, the combination of rubeosis and poor dilation may produce intraoperative hemorrhages of the anterior chamber (Fig. 20.7).
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
