 oon after I entered the field of phaco-emulsification, I began hearing about the problems surgeons had managing a difficult type of cataract called “posterior polar cataract,” which consisted of typical concentric rings around the central lenticular opacity (onion ring). Review of the literature revealed that standard treatment was to perform a regular 5.5-mm circular central capsulorrhexis and not to perform hydrodissection. In the subsequent months I treated many such cases with equal success (avoiding posterior capsule rupture) and failure (posterior capsule opening with or without the lens dropping into the vitreous). I wondered what was lacking in my technique and concluded that scarcity of working area led to failures. So I increased the size of the capsulotomy in one direction, the direction of sculpting. What resulted was a complete absence of posterior capsule ruptures and nucleus drops, not only in posterior polar cataracts but also in cases with preexisting ruptures. More importantly, surgical time was cut in half. I extended my experience with long oval capsulotomy to hard cataracts and found it to be equally effective.
oon after I entered the field of phaco-emulsification, I began hearing about the problems surgeons had managing a difficult type of cataract called “posterior polar cataract,” which consisted of typical concentric rings around the central lenticular opacity (onion ring). Review of the literature revealed that standard treatment was to perform a regular 5.5-mm circular central capsulorrhexis and not to perform hydrodissection. In the subsequent months I treated many such cases with equal success (avoiding posterior capsule rupture) and failure (posterior capsule opening with or without the lens dropping into the vitreous). I wondered what was lacking in my technique and concluded that scarcity of working area led to failures. So I increased the size of the capsulotomy in one direction, the direction of sculpting. What resulted was a complete absence of posterior capsule ruptures and nucleus drops, not only in posterior polar cataracts but also in cases with preexisting ruptures. More importantly, surgical time was cut in half. I extended my experience with long oval capsulotomy to hard cataracts and found it to be equally effective.
Two difficult situations for a phaco-emulsification surgeon are posterior polar cataracts and white cataracts. A posterior polar cataract is a dense, white, rounded opacity situated on the central posterior capsule that typically consists of concentric rings around the central opacity. It has an inherent tendency to present with posterior capsule rupture either during surgery or even before it as a preexisting posterior capsular rent. Osher and colleagues (1990) reported a 26% (8 of 31 eyes) incidence of posterior capsule rupture during surgery in eyes with a posterior polar cataract.1
To prevent posterior capsular rupture, various measures have been suggested in the literature, including slow-motion phaco-emulsification with low aspiration flow rate, a low level of vacuum and infusion pressure; viscodissection to immobilize epinucleus and cortex; and inside-out delineation.
Large Oval Capsulotomy
I use a large oval capsulotomy or capsulorrhexis from the 12 o’clock periphery to the 6 o’clock periphery to treat all cases of posterior polar cataract. This technique has all but eliminated posterior capsule rupture. Several advantages to this type of capsulotomy are:
- It guards against accidental increase of in-the-bag pressure during water-powered procedures.
- It increases the working area so that sculpting can be done in the entire length of the nucleus, which aids easy division.
- It facilitates easy removal of lens fragments with the bimanual help of the phaco probe and the chopper without any rotatory movement (which needs to be avoided).
- Shorter sides of the rhexis function like a tamponade to the forward-bulging vitreous mushroom.
- The maneuverability while performing a posterior circular central capsulorrhexis is improved because of the greater working area.
- Large oval capsulotomy gives a stronger grip to optic capture of the 6-mm intra-ocular lens to be implanted in the sulcus in case in-the-bag implantation appears risky.
- Plenty of space between the optic edge and capsulotomy edge means a vitrectomy probe can be introduced without tilting the intra-ocular lens.
The large oval capsulotomy is useful when the diagnosis of a pre-existing posterior capsule rupture is suspected or established. To illustrate the utility of large oval capsulotomy, I have chosen an even more complicated case than a posterior polar cataract. In this case, pre-existing posterior capsular rupture was suspected.
TECHNIQUE
Anesthesia
The patient was given peribulbar anesthesia with pressure on the eyeball to make the globe soft.
Surgical Technique
- Make two ports, one side port at the 1 o’clock position and a second phaco port at 11 o’clock.
- Stain the anterior capsule with trypan blue for better visibility, then fill the anterior chamber with visco-elastic material.
- Use a Fugo blade to make a large oval capsulotomy in a vertical direction (Fig. 19.1).
- Start phaco-emulsification of the nucleus. At the end of it, you will see a rent in the posterior capsule, through a gap in the cortex. Withdraw the phaco-emulsification probe.
- Extend the phacoemulsification incision (Fig. 19.2).
- Use dry aspiration in the capsular bag to clear the cortex.
- Perform a small anterior vitrectomy.
- Implant a posterior chamber intra-ocular lens inside the capsular bag. In our case, the edge of the posterior capsular tear and the anterior capsulotomy were visible.

Figure 19.1. A long vertically oval capsulotomy is made with the Fugo blade. The nucleus is removed. When the torn posterior capsule becomes visible through the cortex, phaco-emulsification is stopped.
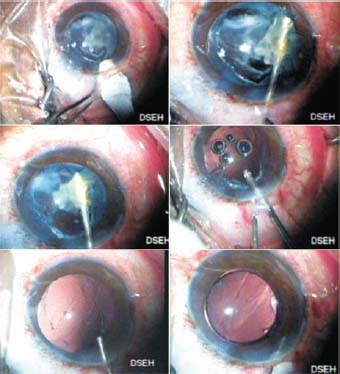
Figure 19.2. The main incision is enlarged and the area is aspirated manually. When the vitreous appears, a vitrector is used. The posterior chamber intra-ocular lens is implanted in the bag. The long posterior capsular rent is visible under the intra-ocular lens.
During our procedure there was no extension of the posterior capsular tear. The long oval Fugo blade capsulotomy prevents pressure build-up inside the capsular bag. It also allows the phaco-emulsification process to be done along a greater length of the nucleus than would be allowed if the capsulotomy was a standard circular 5.5 mm.
Large Round Capsulotomy in a White Cataract
Fugo blade capsulotomy makes it simple to make a large capsulotomy. No capsulotomy is extended toward the periphery, which could threaten the posterior capsule (Fig.19.3).
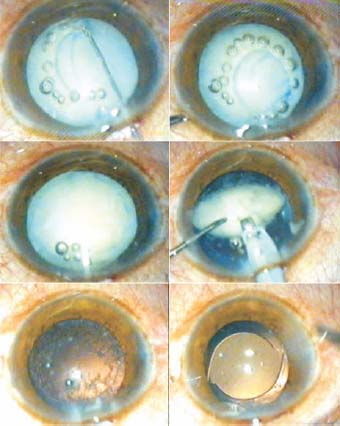
Figure 19.3. A dense white cataract. A large Fugo blade capsulotomy makes it easy to bring out and perform phaco-emulsification on the hard lens. The lens matter is aspirated. A posterior chamber intra-ocular lens has been implanted, without covering the anterior capsule.
It is commonly taught that Elschnig pearls develop as a result of anterior epithelial cell migration from under the anterior capsule onto the posterior capsule. If this is true, then why do we preserve the anterior capsule? If preservation of the anterior capsule has something to do with holding the optic tight and pushing it back against the posterior capsule to prevent after-cataract formation, why does the credit for a postoperative clean posterior capsule go to certain type of lens design? I think that an intra-ocular lens with a square edge prevents posterior capsular opacification even in the absence of a leatherlike anterior capsule.
Summary
Large oval capsulotomy using the Fugo blade has several advantages. With a large capsulotomy, the phobia about posterior polar and hard cataracts is gone. Risk to the integrity of the superior or the inferior margin of capsulotomy during phaco-emulsification is reduced to nothing. With an increased working area and increased gutter length, the bimanual force applied in opposite directions to break the segments is reduced, which helps safeguard weak zonules. Despite the use of high phaco power to emulsify stonelike cataracts, the incidence and severity of striate keratitis have been reduced.
Reference
1. Osher RH, Yu BC, Koch DD. Posterior polar cataracts: a predisposition to intraoperative posterior capsular rupture. J. Cataract Refract Surg. 1990;16:157–162.
Suggested Readings
Allen D, Wood C. Minimizing risk to the capsule during surgery for posterior polar cataract. J Cataract Refract Surg. 2002;28:742–744.
Anis AY. Understanding hydrodelineation: the term and the procedure. Doc Ophthalmol. 1994;87:123–137.
Consultation section: cataract surgical problem. J Cataract Refract Surg. 1997;23:819–824.
Emery JM, Little JH. Phacoemulsification and aspiration of cataracts, surgical technique, complications and results. St. Louis, Mo: Mosby, 1979:45–49.
Fine IH. Cortico-cleaving hydrodissection. J Cataract Refract Surg. 1992;18:508–512.
Fine IH, Packer M, Hoffman RS. Management of posterior polar cataract. J Cataract Refract Surg. 2003;29:16–19.
Gimbel HV, DeBroff BM. Posterior capsulorrhexis with optic capture: maintaining a clear visual axis after pediatric cataract surgery. J Cataract Refract Surg. 1994;20: 658–664.
Osher RH. Slow motion phacoemulsification approach. J Cataract Refract Surg. 1993;19:667.
Osher RH, Cionni R, Burk S. Intraoperative complications of phacoemulsification surgery. In: Steinert RH, ed. Cataract surgery: technique. complications. and management. 2nd ed. Philadelphia, Pa: Saunders, 2004:469–486
Vasavada AR, Desai JP. Stop, chop, chop, and stuff. J Cataract Refract Surg. 1996;22:526–529.
Vasavada AR, Irivedi R. Role of optic capture in congenital cataract and IOL surgery in children. J Cataract Refract Surg. 2000;26:824–831.
Vasavada AR, Raj SM. Inside-out delineation. J Cataract Refract Surg. 2004;30:1167–1169.
Vasavada AR, Singh R. Phacoemulsification with posterior polar cataract. J Cataract Refract Surg. 1999;25:238–245.
Vasavada AR, Singh R. Step-by-step chop in situ and separa- tion of very dense cataracts. J Cataract Refract Surg. 1998;24:156–159.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


