Bone, Cartilaginous, and Jaw Lesions that May Be Sampled with Upper Aerodigestive Tract Biopsies
Numerous bony, cartilaginous, and odontogenic lesions can involve the upper aerodigestive tract. Some can involve all sites, but many show an obvious predilection for the alveolar ridge or the extension into the paranasal sinuses. This is not surprising as odontogenic epithelium and rests occur throughout these sites. Furthermore, bony or other lesions involving the thin bones surrounding the sinonasal tract can easily extend into the sinuses and present as expansile masses. A discussion of all the lesions of the craniofacial bones is far beyond the scope of this monograph, however, and here we present the lesions that we have encountered most frequently in the upper aerodigestive tract biopsy specimens.
CHONDROID AND OSSEOUS METAPLASIA
Chondroid and osseous metaplasia occur throughout the upper aerodigestive tract and must be distinguished from neoplasia. These metaplastic lesions typically develop in areas of chronic inflammation.1 Metaplasia is especially prone to occur secondary to ill-fitting dentures or in areas of redundant or “flabby” alveolar ridge tissue. Most lesions have bone with overlying hyaline and fibrocartilage that blend into the surrounding fibrous tissue (Fig. 12.1, e-Fig. 12.1). The chondroid tissue is typically bland and resembles normal, mature cartilage. In rare cases, cellular atypia may raise concerns of chondrosarcoma. Chondroid metaplasia of the true or false vocal cord can also occur and, as was discussed in Chapter 1,
cartilaginous nodules are normally seen in the anterior portion of the thyroarytenoid ligament. Finally, cartilaginous or osseous metaplasia often develops in sarcomatoid carcinomas and one should exclude a concomitant malignancy when either is present.
cartilaginous nodules are normally seen in the anterior portion of the thyroarytenoid ligament. Finally, cartilaginous or osseous metaplasia often develops in sarcomatoid carcinomas and one should exclude a concomitant malignancy when either is present.
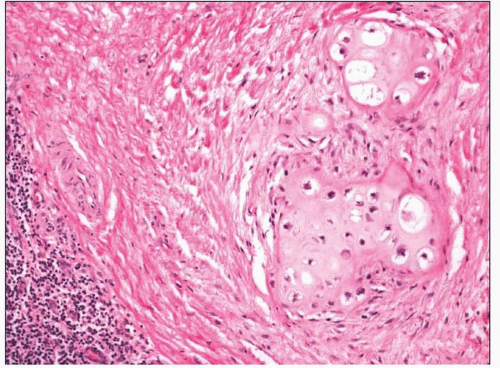 FIGURE 12.1 Chondroid metaplasia seen in peritonsillar fibrous tissue. |
CHONDROMA AND OSTEOMA
Chondromas are much less common than well-differentiated chondrosarcomas and one should be wary about making this diagnosis.2 In the upper aerodigestive tract, “chondroma” may best be used for small, circumscribed lesions that are fully excised. Indeed, it may be more prudent to diagnose lesions nonspecifically as well-differentiated chondroid neoplasms when only a small portion of mature-appearing cartilaginous tissue is seen in a biopsy specimen. Chondromas are composed of central, well-circumscribed hyaline cartilage devoid of cytologic atypia with rare or absent mitotic figures (e-Fig. 12.2). They are surrounded by a thin layer of fibrous tissue. These lesions are benign and should generally not recur after resection.
Osteomas can develop throughout the upper aerodigestive tract, often associated with adjacent bone. A unique osteoma, referred to by some as a “choristoma,” occurs in the dorsum of the tongue, most commonly in young to middle-aged women.3 These vary in size but generally do not grow more than 2 cm. They are usually well circumscribed and are composed of dense, mature, laminated bone (Fig. 12.2, e-Fig. 12.3). They do not recur after resection.
 FIGURE 12.2 A well-circumscribed osteoma of the tongue made of mature bone. |
GIANT CELL REPARATIVE GRANULOMA
Giant cell reparative granuloma may be central and entirely located within mandible or maxilla.4,5 Sometimes it involves the nasal cavity or paranasal sinuses and can be sampled as a nasal or sinonasal mass. These lesions are thought to be reactive and secondary to trauma, hemorrhage, or inflammation, although a neoplastic origin cannot be excluded. Patients are typically younger than 30 years. Histologically, aggregates of giant cells are seen within a fibrovascular stroma, often associated with hemorrhage (Fig. 12.3, e-Fig. 12.4). The giant cells tend to be smaller, with fewer nuclei than those seen with true giant cell tumors. It has been noted that they histologically resemble solid aneurysmal bone cysts.
GIANT CELL TUMOR
Unlike giant cell reparative granuloma, true giant cell tumors are rare within the head and neck. When they arise here, they are most frequently reported in the sphenoid and temporal bones or within the larynx.6,7 Within the larynx, these tumors present in adults over a wide age range and are much more common in men. Most have arisen from the thyroid or cricoid cartilage, and patients typically present with hoarseness or obstruction. Tumors average approximately 4 cm in greatest dimension and are grossly infiltrative, sometimes with associated hemorrhage or cystic degeneration. Microscopically, the lesions are identical to those more often seen in the long bones and are composed of innumerable giant cells
admixed with macrophages and fibroblasts (Fig. 12.4). The giant cells have numerous (often >20) bland nuclei, similar to those of the surrounding epithelioid to spindled mononuclear cells. Mitotic figures are often noted. Patients with laryngeal giant cell tumors do well, and the tumors do not
recur after resection or other treatment. Malignant and aggressive giant cell tumors of the sphenoid have been reported; however, some of these may actually represent giant cell-rich osteosarcoma, as they have been noted in patients with Paget’s disease and in children.7
admixed with macrophages and fibroblasts (Fig. 12.4). The giant cells have numerous (often >20) bland nuclei, similar to those of the surrounding epithelioid to spindled mononuclear cells. Mitotic figures are often noted. Patients with laryngeal giant cell tumors do well, and the tumors do not
recur after resection or other treatment. Malignant and aggressive giant cell tumors of the sphenoid have been reported; however, some of these may actually represent giant cell-rich osteosarcoma, as they have been noted in patients with Paget’s disease and in children.7
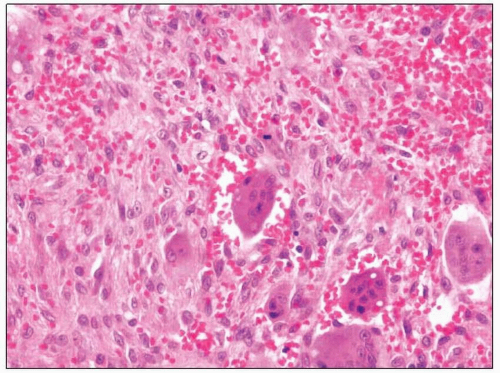 FIGURE 12.3 Giant cell reparative granuloma is characterized by numerous multinucleated giant cells within a hemorrhagic stroma. |
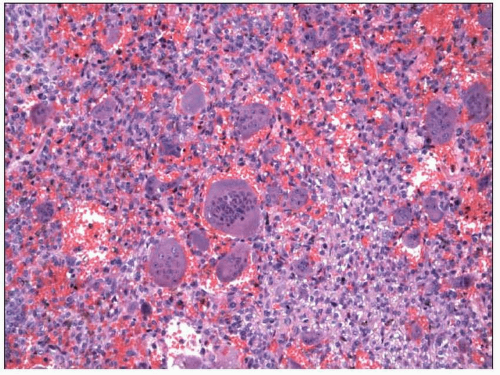 FIGURE 12.4 Large, multinucleated cells are present diffusely throughout this laryngeal giant cell tumor. |
FIBRO-OSSEOUS/CEMENTIFYING LESIONS (FIBROUS DYSPLASIA, OSSIFYING/CEMENTIFYING FIBROMA, ETC.)
Fibro-osseous lesions frequently develop within the bones of the jaw. They sometimes involve the sinonasal structures or extend from the alveolar ridge (these are mentioned briefly in the discussion on fibroma in Chapter 11). As such, they sometimes must be diagnosed with biopsy samples from the upper aerodigestive tract.
Fibrous dysplasia typically presents centrally within the jaw bones but may also involve the sinonasal tract.8 Depending on its primary site of growth, it can present with facial swelling, visual impairment, or sinonasal obstruction. When the lesions involve multiple noncontiguous bones, the disease is considered polyostotic and McCune-Albright syndrome should be excluded. These lesions typically present in children and young adults and may appear lytic, sclerotic, or mixed, depending on the age of the lesions. These are typically benign and stop growing with skeletal maturation. Classically, fibrous dysplasia is composed of intermixed, irregular fragments of woven bone with a cellular stroma. The woven bone is typically not lined by osteoblasts, and the cellular stroma is composed of bland spindled cells (Fig. 12.5, e-Fig. 12.5). Some osteoblastic rimming
and lamellar bone formation can be seen and one should not use those features to exclude a diagnosis of fibrous dysplasia.
and lamellar bone formation can be seen and one should not use those features to exclude a diagnosis of fibrous dysplasia.
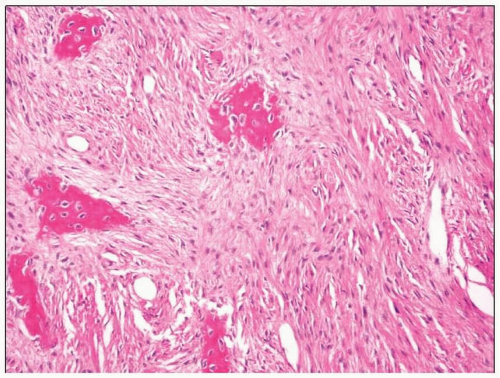 FIGURE 12.5 Woven bone admixed with a cellular stroma typifies fibrous dysplasia. |
Ossifying fibromas, like most fibrous dysplasias, are also usually centrally located in the jaw bones. They, too, may extend into the sinonasal tract, especially certain variants such as juvenile psammomatoid ossifying fibroma.8,9 and 10 Whereas juvenile psammomatoid ossifying fibromas often occur (as the name implies) in adolescents and in young adults (although they also occur in older adults), conventional ossifying fibromas occur in patients who are, on average, in their fourth decade of life. These lesions have variable radiolucency and density, depending on the proportion of the lesion that is bony. These lesions are also benign, although juvenile psammomatoid ossifying fibroma has been noted to be locally aggressive.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


