9 Benign Maxillary Sinus Masses The maxillary sinus may harbor any of a large number of benign lesions with a different array of etiologies. Being a relatively large cavity within the craniofacial skeleton, long periods may pass before any symptoms manifest themselves. Frequently, patients only present when their lesions have filled the cavity, causing pressure symptoms or spread into surrounding areas such as the nasal cavity. Many pathologies in this area share common presenting symptoms, but some have unique features. The goal of this chapter is to present a detailed overview of these lesions’ characteristics, their diagnosis, and treatment. Benign lesions of the maxillary sinus can be conveniently divided into nonneoplastic and neoplastic (Table 9.1). Nonneoplastic lesions represent a range of inflammatory conditions with varied etiology, some not well understood. Neoplasms can originate from any of the tissues that form the architecture of the maxillary sinus. These include the mucosa, salivary glands, mesenchyme, vessels, muscle, dentition, and bone. They are uncommon tumors: Some are very rarely encountered. Many of these pose significant diagnostic problems requiring a low threshold of suspicion and histopathologic expertise. Lesions of the maxillary sinus affect a wide age range from children to the elderly and some have either sex predilection. Lesions such as fibrous dysplasia have a tendency to stabilize, but others are slowly progressive. Many of the maxillary sinus lesions are initially asymptomatic and only cause symptoms when they reach larger dimensions. They share a common presentation similar to rhinosinusitis such as unilateral nasal obstruction, rhinorrhea, and local discomfort. Some symptoms are more common with certain lesions such as epistaxis in hematomas and hemangiomas. Lesions such as mucoceles and most tumors can lead to expansion of the sinus with the resultant facial swelling. When symptoms due to pressure occur, they can lead to epiphora, diplopia, proptosis, and loose dentition, but paresthesias are rarely encountered. Palatal and gingival swellings are sometimes encountered with salivary gland and odontogenic tumors, respectively. Computed tomography (CT) is the most commonly used modality. Although most lesions share common features of radiopacity in the sinus, some show specific features that are sometimes diagnostic. This is often true for mucoceles, antrochoanal polyps, Wegener granulomatosis, antrolithiasis, and odontogenic and fibroosseous tumors (see below). Magnetic resonance imaging (MRI) can often be helpful in differentiating fluid from soft tissue and contrast enhancement is useful in delineating tumors. Panoramic maxillary x-rays (orthopantomogram [OPG]) can give supplementary information particularly with odontogenic tumors.
 Differential Diagnosis
Differential Diagnosis
 Diagnosis
Diagnosis
Clinical Features
Imaging
Nonneoplastic | Neoplastic |
|---|---|
Mucosal cyst | Papillomas |
Antrochoanal polyp | Salivary gland tumors (pleomorphic adenoma, oncocytoma) |
Fungal disease (covered in chap 5) | Mesenchymal tumors (fibroma, lipoma, myxoma) |
Mucocele | Vasiform tumors (hemangioma, aneurysmal bone cyst, hemangiopericytoma) |
Cholesterol granuloma | Tumors of muscle origin (leiomyoma, rhabdomyoma) |
Hematoma | Odontogenic tumors (see also Table 9.3) |
Eosinophilic angiocentric fibrosis | Fibroosseous lesions (osteoma, ossifying fibroma, fibrous dysplasia, osteoblastoma) |
Granulomatous deposits in sarcoidosis and Wegener granulomatosis | Neuroectodermal tumors (schwannoma, neurofibroma) |
Antrolithiasis |
|
Additional Tests
When suspected, blood serology for granulomatous disease (angiotensin converting enzyme [ACE] and cytoplasmicstaining antineutrophil cytoplasmic antibodies [cANCA]) and clotting factors in case of hematomas are done. Some tumors occasionally represent part of a syndrome, which should be suspected and investigated. These include osteoma in Gardner syndrome, fibrous dysplasia in McCune–Albright syndrome, and neurofibromas in type 1 neurofibromatosis (NF1; see below).
 Surgery
Surgery
Surgery is the main treatment of the majority of maxillary sinus lesions except when they are asymptomatic and nonprogressive such as small osteomas and fibrous dysplasia, respectively (see below). Most lesions can be excised through an endoscopic approach with other approaches available for extensive, awkwardly positioned, or recurrent lesions. The surgeon should always be prepared to change the approach to get the optimum result and this must be part of the informed consent.
Endoscopic Resection
Standard endoscopic sinus surgery techniques are often sufficient to excise maxillary sinus lesions.1 A large middle meatal antrostomy should be fashioned to obtain sufficient access. Angled instruments, specifically designed for the maxillary sinus are invaluable. We also use combinations of 30- and 45-degree rigid endoscopes for removal and 70-degree for final inspection. Occasionally, the antrostomy can be extended inferiorly through to the middle portion of the inferior turbinate if more access is needed. This can also be combined with an inferior antrostomy to access the floor such as in some cases of antrolithiasis. An endoscopic medial maxillectomy is sometimes necessary such as in cases of extensive inverted papilloma of the medial maxillary wall.2,3 This involves removal of the inferior turbinate and medial wall down to the nasal floor with varying degrees of resection for the bone of pyriform aperture (see Video 9.1). The endoscopic resection can also be combined with an anterior antrostomy (Caldwell–Luc approach) when access to the floor and lateral wall is required.
Anterior Antrostomy
Although the use of a Caldwell–Luc approach has considerably declined in the management of chronic rhinosinusitis, it still has a definite role in the management of benign maxillary lesions.4 We often use it in combination with the endoscopic approach to improve access. A standard gingivobuccal incision is made at the canine fossa after infiltrating the area with 1:80,000 epinephrine and 2% lignocaine. The incision starts at the level of the canine tooth and ends at the first molar, and is carried down to the bone. After retracting the periosteum, a cutting bur is used to drill a window in the bone and then the mucosa of the sinus cavity is opened. The window should be 1 to 2 cm inferior to infraorbital rim and 1 to 2 cm superior to the gingivobuccal sulcus to avoid injuring the infraorbital nerve and dental roots. The gingivobuccal flaps are kept retracted and instruments and/or endoscopes can be introduced through antrostomy. Closure of the soft tissue at the end of the procedure is achieved with a continuous absorbable suture.
Midfacial Degloving
This approach is ideally suited for extensive lesions because it allows direct access to the maxillary sinus, nasal cavity, and infratemporal fossa while avoiding external incisions.5,6 Complications are infrequent and can generally be avoided by applying meticulous techniques. The procedure is in essence an extension of bilateral gingivobuccal incisions with the inclusion of the nasal dorsum through intercartilaginous and transfixion incisions. First 1:80,000 epinephrine and 2% lignocaine are infiltrated into the gingivobuccal sulcus, intercartilaginous area, and columella. A bilateral gingivobuccal incision is made down to bone running from maxillary tuberosity to tuberosity. The periosteum and soft tissue of the cheek are raised, as for Caldwell–Luc approach, exposing the infraorbital nerves and orbital margin. Intercartilaginous incisions are made as in rhinoplasty and connected to transfixion incision at the caudal end and anterior septum separating it for the medial crura. The incision is continued across the floor of the nose to join the intercartilaginous incisions laterally. Elevation of the nasal soft tissue envelope all the way laterally to the maxillary bones now allows complete degloving of the middle third of the face. At the end of the procedure, closure is achieved with absorbable suture and a nasal plaster is used.
Lateral Rhinotomy and Medial Maxillectomy
Lateral rhinotomy allows direct access to the lateral nasal wall and maxillary sinus.7 With meticulous techniques an innocuous scar and minimal morbidity is achievable. It has the advantage of being extendable superiorly to gain access to the orbit and frontal sinus if needed. The incision site is infiltrated with epinephrine and lignocaine as above. The curvilinear skin incision begins just below the medial aspect of the brow and extends inferiorly midway between the medial canthus and nasion. It is then carried over just anterior to the nasomaxillary sulcus and alar groove to end in the nasal vestibule. The incision is deepened to the bone then the periosteum is retracted after achieving hemostasis. The medial canthal ligament and lacrimal sac are detached laterally. An osteotomy along the frontal process of the maxilla can then be made using a saw or osteotome. Incising the nasal mucosa and retraction of the bone laterally then allows access into the nasal cavity and lateral nasal wall. A medial maxillectomy can satisfactorily be done through this approach by removing bone at the pyriform aperture from anterior to posterior. Closure of the periosteum is achieved with absorbable sutures after reattaching the medial canthal ligament. Skin closure is done with fine Prolene (Ethicon, Somerville, NJ) sutures.
 Other Treatments
Other Treatments
In general, surgery is not indicated in active granulomatous disease and the treatment is medical. Bisphosphonates have been used for the treatment of fibrous dysplasia in some centers (see below).
 Outcomes
Outcomes
A complete cure can be achieved with a large number of benign lesions of the maxillary sinus. Some lesions are more aggressive and some have higher recurrence rates than others. These will be outlined in the rest of the chapter.
 Specific Lesions
Specific Lesions
Nonneoplastic
Mucosal Cyst
Mucosal cysts of the maxillary sinus are common with an incidence between 12.4 and 35.6% detected on radiography.8–10 They are broadly classified into secretory and nonsecretory cysts.11 Obstruction of mucosal glands leads to the formation of secretory cysts, which are less common. The more common nonsecretory cysts are presumably caused by an accumulation of exudates in the sinus mucosa lifting the epithelial lining. The etiologic factors behind cyst formation remain unknown. One study showed high levels of immunoglobulins, complement, and antiproteases in cyst aspirates consistent with an inflammatory process.12 Levels of immunoglobulin E (IgE) and eosinophils were not raised, suggesting that allergy was not a significant factor. Oral flora was cultured from cyst fluid suggesting a possible dental cause. In another study, dental disease has been found in up to 50% of patients’ mucosal cysts.9 The majority of mucosal cysts originate in the floor of the maxillary sinus.9 They are mostly unilateral, but can be bilateral in 10 to 20% of cases.13,14 They are usually seen as homogeneous, domeshaped opacities on CT scanning and are usually a chance diagnosis on sinus radiography (Fig. 9.1).10 Controversy still exists on the clinical importance of mucosal cysts. Some authors suggest they represent an inflammatory sinus disease; others disagree.9,10 The variation could be attributed to different patient populations chosen for studies and the methods of interpretation of results. A recent study of a large number of patients undergoing CT scanning for ophthalmologic conditions showed no statistically significant relationship to subjective rhinologic symptoms and objective measurements in the form of Lund–Mackay Scores.10 The mere presence of the cysts, in the opinion of the authors, is not in itself an indication for surgical intervention. When operating on patients with rhinosinusitis, mucosal cysts are often encountered and can be opened (Fig. 9.2). They express yellowish to green transparent fluid and can be removed via a middle meatal antrostomy.

Fig. 9.1 A coronal computed tomography scan showing a mucosal cyst in the left maxillary sinus. Note the typical domed surface and the origin at the floor of the sinus.
Antrochoanal Polyp
An antrochoanal polyp (ACP) is a benign lesion that originates from the mucosa of the maxillary sinus and grows into the nasal cavity to reach the choana. Although the first report of ACP was attributed to Palfyn in 1753, it was Killian who described the condition in detail in 1906.15 ACPs account for 4 to 6% of all nasal polyps with increased incidence of 33% in children.16,17 ACPs are usually unilateral with only a small number of reported cases with bilateral polyps.16 It has been suggested that most ACPs originate from the posterior antral wall. In a series of 37 cases, 38% originated in the posteromedial wall, 19% in the posterior wall, 8% in the anterior wall, 8% in the anteromedial wall, 8% in the floor, 5% in the lateral wall, 5% in the roof, 3% in the anterolateral wall, 3% in the posterosuperior wall, and 3% in the inferolateral wall.18 Mean age of presentation is 27 years and it is reported to be twice as common in males than females.18 However, some have reported no difference in incidence between males and females in a pediatric population.19,20 An ACP differs from nasal polyps in the fact that it is a solitary lesion that extends into the choana. Stammberger and Hawke21 found that 70% of ACPs emerge through an accessory ostium. Aydin et al studied 37 patients with ACP and found that 51% originated from an accessory ostium, 43% from the natural ostium, and 6% from both.18 Macroscopically, it has a cystic part filling the maxillary sinus and a solid part in the nasal cavity.22 Berg found similarity between both tissues and fluid content in ACP and maxillary mucosal cysts with the resultant hypothesis that ACP is the intranasal form of mucosal cysts. Microscopically, it has a central cavity surrounded by a homogeneous edematous stroma bearing few cells, while the polyp surface is covered with respiratory epithelium.
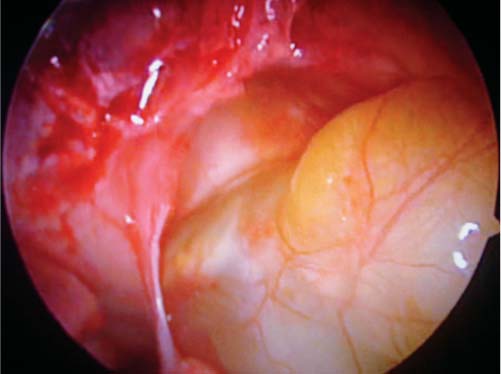
Fig. 9.2 An endoscopic view of a mucosal cyst in the left maxillary sinus seen through an antrostomy.
In contrast to nasal polyps, an ACP has less inflammatory infiltrate and significantly lower eosinophils while edema is essentially the same.23 An ACP also exhibits significantly higher fibroinflammatory changes with proliferation of fibroblasts and collagen, and a lymphocyte inflammatory infiltrate. It has been postulated that the latter is related to the long evolution of an ACP that leads to a scarring stage.16 The surface epithelium of an ACP is mostly intact in contrast to some disruption in nasal polyps.24
The molecular biology of an ACP has been studied by some authors. Urokinase type plasminogen activator (uPA), which is related to proliferative changes of the mucous membrane in inflammatory tissue, has been identified in ACP tissue extracts.25 Others reported that the expression of basic fibroblast growth factor (bFGF) and transforming growth factor (TGF) β was significantly higher in ACPs than in chronic rhinosinusitis and healthy mucosa.17 Some also showed increased expression of matrix metalloproteinase-9 (MMP-9), which is involved in mucous membrane inflammation, in ACPs, and nasal polyps compared with normal nasal mucosa.26 Clinical manifestations usually start with unilateral nasal obstruction, but other symptoms have been reported such as epistaxis, purulent rhinorrhea, postnasal drip, snoring, obstructive sleep apnea, dysphonia, and dysphagia.16,18
Nasal endoscopy reveals a smooth swelling originating in the middle meatus and extending posteriorly into the choana. Very large ACPs can be seen in the nasopharynx or even in the oral cavity. CT scanning shows a mass filling the maxillary sinus with opacification of the middle meatus and extension into the choana (Fig. 9.3). MRI shows a hypointense signal on T1 modality and enhanced signal on T2 modality.
The accepted management of ACPs is surgical removal. Simple avulsion is associated with high rates of recurrence because the maxillary portion is not removed.16 Endoscopic sinus surgery is used where a large middle meatal antrostomy is created to access the maxillary portion. A nasal snare can be tightened around the nasal portion close to the antrostomy and gradual “to and fro” movement can lead to the complete removal of the whole ACP. The cavity of the maxillary sinus is then inspected with angled endoscopes and any mucosal remnant is removed. For this, angled instruments or a curved microdebrider can be used (see Video 9.2). Some advocate the combined use of a Caldwell–Luc approach with an endoscopic procedure.16,18 We prefer to reserve the combined approach for recurrent cases.

Fig. 9.3 An axial computed tomography scan of a patient with a right antrochoanal polyp showing both maxillary and nasal components with a narrower part passing through an accessory ostium.
Mucocele
A mucocele is an epithelial-lined mucus-containing sac completely filling a sinus cavity. Its main feature is the capability of expansion by the process of bone resorption and new bone formation.27 As it expands, it becomes locally destructive and leads to the displacement of adjacent tissues. Maxillary sinus mucoceles are rare in comparison to frontal or frontoethmoidal mucoceles. They account for fewer than 10% of all mucoceles of the paranasal sinuses in the United States and Europe.28–31 However, they are more commonly reported in Japan, usually as a long-term sequel of Caldwell–Luc surgery.32 It has traditionally been thought that mucoceles develop as a result of obstruction of sinus outflow resulting in accumulation of mucus and buildup of pressure that gradually causes expansion and destruction.33 It has been shown that the obstruction in combination with superimposed infection cause the release of cytokines from lymphocytes and monocytes. The cytokine release stimulates fibroblasts to secrete prostaglandins and collagenases, which, in turn, stimulate bone resorption.34,35 The etiologic factors that lead to the formation of mucoceles have been attributed to previous surgery, trauma, inflammation, and tumors.28,31 The development of a mucocele is a slow process that can take many years. In one large series, the median interval for the development of maxillary mucoceles after Caldwell–Luc was 15 years.28 This was the longest when compared with mucoceles in other sinuses. Interestingly, 17 to 36% of patients with mucoceles do not have a history of any of the above.28,36
Symptoms and signs are caused by the expansion of the mucocele into the nose and surrounding structures. Patients can present with nasal obstruction, cheek swelling, upward displacement of the globe and proptosis.28,30,31 Endoscopic examination may reveal pus or occasionally prolapse of the medial sinus wall in the middle meatus. Busaba stated that a triad of a bulging medial wall, prolapsed middle meatal mucosa obliterating the middle meatus, and a streak of mucopurulent drainage in the middle meatal region is suggestive of a maxillary mucocele.30 CT scanning is the optimum diagnostic modality to show bone expansion and typically the bony outline becomes more rounded as the bone remodels in response to pressure within the sinus cavity (Fig. 9.4A).31 MRI is not always necessary, but will establish the fluid content of the mucocele.31
Traditional teaching emphasized the need for complete removal of the mucocele to prevent recurrence.28,29 It is now well established, however, that the majority of mucoceles can be managed endoscopically. Bockmühl suggested some contraindications to the endoscopic approach, which include far lateral (compartmentalized) or zygomatic bone maxillary mucoceles, the presence of a cutaneous fistula and in cases of associated malignancy.28 The authors perform a large middle meatal antrostomy of up to 2 cm in diameter to avoid restenosis and recurrence of the mucocele. If needed, a partial medial maxillectomy that involves excising the middle third of the inferior turbinate can be done. This would not cause damage to the nasolacrimal duct. It is not necessary to remove the mucosa of the mucocele cavity because it is known that the mucocele epithelium retains its respiratory nature and returns to normal appearance after surgery.34 Over a period of 3 to 6 months, bone remodeling with shrinkage of the expanded sinus walls occurs (Fig. 9.4B).
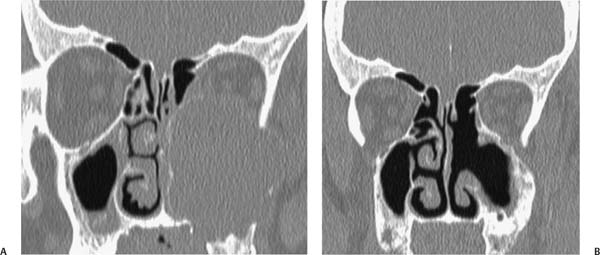
Fig. 9.4 (A) A coronal computed tomography scan of a large left maxillary mucocele showing extensive expansion, bone thinning, and pressure on the orbit. The patient presented with cheek swelling and nasal obstruction, but no diplopia due to the slow developing-disease process. (B) Same patient in Fig. 9.3A 6 months after drainage of the mucocele through a large middle meatal antrostomy. Note the return of the sinus cavity to its normal contours.
Cholesterol Granuloma
Cholesterol granuloma (CG) is a histologic term used to describe the coexistence of granulation tissue with cholesterol crystals and foreign body giant cells.37 The condition is well described in the temporal bone, but is rarely encountered in the paranasal sinuses.38 Within the small number of published cases, the maxillary sinus is most commonly involved.38,39 Only one case of bilateral maxillary sinus involvement has been reported.39 CG has been observed more in men, with 3:1 male to female ratio and an average age of 41 years. The disease duration varied from 6 weeks to 10 years.39 Only a small number of patients had a history of previous trauma or surgery.38,39
It has been suggested that a combination of factors leads to the formation of CG. These include disturbed ventilation in a bony cavity, impaired drainage, and hemorrhage.38–41 Impaired drainage would increase pressure in the sinus cavity, which, in turn, obstructs venous and lymphatic circulation and predisposes to mucosal hemorrhage. The insufficient lymphatic drainage would fail to eliminate lipid components in red blood cells and contribute to accumulation of cholesterol crystals. These act as foreign material that stimulates the granulomatous reaction in the sinus cavity.38,39,42
Patients with CG present with symptoms and signs resembling chronic rhinosinusitis.38,39 Most of the reported cases presented with nasal obstruction, postnasal drip, rhinorrhea, facial pain, or headaches. Rarely patients present with clear golden yellow rhinorrhea, which is considered suspicious of CG.39 CT shows a cyst-like opacity, which does not enhance with contrast. Bony erosion or expansion has been reported in a small number of cases.39,42 The lesion gives a very high signal on all MRI sequences. Therefore, the diagnosis is confirmed on histologic analysis of the removed tissue. This is characterized by a large number of clefts due to the dissolution of cholesterol crystal by alcohol used in staining the tissue.42 These are surrounded by foreign-body giant cells, and macrophages filled with hemosiderin embedded in fibrous granulation tissue.
Treatment is by surgical excision. Most cases are accessible endoscopically and can be completely removed through this route.43 The most frequent findings were cystic or partially cystic masses with bluish, yellowish, or brownish colors.39 It is important to remove the granulation tissue completely to prevent recurrence. A large middle meatal antrostomy and the use of angled instruments will facilitate the procedure. The sinus cavity is inspected with a 70-degree endoscope at the end of the operation to confirm complete removal.
Hematoma
Hematoma of the maxillary sinus is also known as organized hematoma or hemorrhagic pseudotumor.44–46 It is an uncommon cause of a maxillary sinus mass with only a small number of reported cases. A good number of reports come from Korea and Japan.45 Although some of the hematomas have been reported in patients with bleeding diathesis such as Von Willebrand disease, there are several patients who present with what appears to be a spontaneous etiology.45–47 Patients presenting with this condition belong to a wide age range, which probably reflects a varied pathology. It has been suggested that the condition develops in several stages. First a blood clot accumulates in the maxillary sinus secondary to facial trauma, operative bleeding, recurrent epistaxis, or bleeding diathesis. Second, the hematoma develops and because of poor ventilation and obstruction of drainage it transforms into an organized hematoma by means of neovascularization and fibrosis.45,46 Encapsulation of the blood clot by fibrous tissue prevents reabsorption of the hematoma. Further bleeding causes increasing pressure and progressive expansion, which leads to erosion of adjacent structures.46,47
The most common symptom at presentation is epistaxis followed by unilateral nasal obstruction and facial swelling.44,45 Symptoms due to pressure on adjacent structures such as proptosis and infraorbital hypoesthesia have been reported.48,49 Clinical examination shows aspects that are generally similar to those of other expansible nasal masses such as medialization of the lateral nasal wall with or without a mass in the middle meatus.44,45 CT scanning shows the hematoma as a nonenhancing soft tissue mass, which can be heterogeneous or homogeneous. It also demonstrates bony erosion if this has occurred (Fig. 9.5).44,45 The mass is nonenhancing on both T1-weighted and T2-weighted MRI sequences.46,49 Heterogeneous signal intensity on MRI represents different phases of blood products caused by rebleeding into the hematoma.47 Histologically, the hematoma has a peripheral wall that consists of dense fibrous tissue with spindle-shaped myofibroblast cells. The center of the hematoma consists of loose fibrous tissue, which is relatively acellular and contains some intact erythrocytes.44,45,49

Fig. 9.5 A coronal computed tomography scan of a patient with an organized hematoma in the left maxillary sinus showing expansion with bone remodeling.
Treatment is surgical and is accessible endoscopically. The authors have treated all cases of this condition via this route with no recurrence. A large middle meatal antrostomy is often all that is necessary combined with partial medial maxillectomy if needed (see Video 9.3). The hematoma appears as a well-circumscribed nodular mass with no apparent point of origin in the sinus wall (Fig. 9.6). After removal, inspection of the sinus cavity with angled scopes should be done to ensure complete removal.
Eosinophilic Angiocentric Fibrosis
Eosinophilic angiocentric fibrosis (EAF) is an uncommon inflammatory fibrotic lesion that affects the submucosa of the nose, larynx, and orbit.50,51 The pathologic process is manifested by predominantly eosinophilic perivascular inflammation and gradual replacement with progressive fibrosis.50–53 The condition was first described by Roberts and McCann in 1985; since then a small number of cases have been reported.53 EAF is found with a slightly higher incidence in young to middle-aged women than men.50 The etiology of EAF is unknown, but it has been closely linked to granuloma faciale due to similarities in histologic features.50–54 Some association with allergy and trauma has also been suggested, but has not been substantiated.50,51 The majority of the lesions involve the nasal septum and lateral nasal wall, with only a small number of reported cases involving the maxillary sinus. Similarly, the disease has very rarely been reported in the larynx and orbit.50

Fig. 9.6 A photograph of the maxillary hematoma just after removal from the sinus of the patient shown in Fig. 9.5.
EAF is slow growing and can take many years to manifest.50,51 Symptoms are nonspecific and can initially include nasal obstruction, rhinorrhea, epistaxis, and facial pain.50,53,54 Due to mass expansion the patients will later present with facial swelling.50,51 Involvement of the orbit can lead to periorbital edema and proptosis.50 Examination usually reveals thickening of the nasal septum with an intranasal mass.50,51
Imaging findings are usually nonspecific and include septal thickening, sinus opacification, and focal bone destruction.50,52 Histology is diagnostic due to the very specific features: perivascular fibrosis with collagen and reticulin fibers in an “onion-skin like” pattern.50–52 Single histology specimens may exhibit a spectrum of lesions from early inflammatory to late fibrotic lesions.50 Early lesions consist of an eosinophilic vasculitis without fibrinoid necrosis involving small blood vessels (capillaries and/or venules). Eosinophils predominate, but they are invariably accompanied by plasma cells and lymphocytes.50 There are no granulomas, foreign body-type giant cells or necrosis.50,52 Late lesions show dense fibrous thickening of the subepithelial stroma with obliterative perivascular onion-skin of collagen and reticulin fibers.50
Surgical resection appears to be the treatment of choice, but recurrences are common.50–52 The surgical approach is tailored to the extent of the lesion and lateral rhinotomy is often required.51 Medical treatment with various agents such as local and systemic steroids, dapsone, hydroxychloroquine, and azathioprine have been unsuccessful.50,51
Granulomatous Deposits in Sarcoidosis and Wegener Granulomatosis
Sarcoidosis is a chronic noncaseating granulomatous disease of unknown origin, principally affecting the respiratory tract.54 The multisystem nature of sarcoidosis was described by Boeck in 1899.55 The incidence of the condition is estimated between 1.2 and 19 per 100,000 in Caucasians; it is much higher in African Americans with a ratio of 12:1.56 There is a slight female preponderance with the age of presentation between the third and fifth decades.56–58 West Indians and Scandinavians appear to be more commonly affected than other racial groups.
There is predilection for lungs and hilar lymph nodes, which are affected in 90% of patients with clinical disease. The disease involves the nose and sinuses in only 1 to 4% of patients.56–59 A minority present with nasal symptoms without other systemic manifestations of the disease.56,58,60 Patients complain of nasal stuffiness, blood-stained discharge, crusting, and an offensive postnasal drip. Clinical manifestations include nasal crusting with friable submucosal yellowish granulomas involving the inferior turbinates and septum (Fig. 9.7). The inflammation may progress to cause septal ulceration and perforation, which occurs particularly in those who have had previous surgery. Saddling of the nose or skin manifestations (lupus pernio) are occasionally seen (Fig. 9.8). Although the sinuses are often involved in patients with nasal disease, it is extremely rare for patients to present with isolated maxillary sinus involvement without nasal symptoms. Only a small number of cases have been reported and certainly this reflects our experience.56,57 Nevertheless, the condition should be included in the differential diagnosis of maxillary sinus masses. Findings on CT scanning of the sinuses are nonspecific with uniform opacity and occasional bony erosion. Erythrocyte sedimentation rate (ESR), ACE levels, and chest radiography are worth considering in suspected cases. Biopsy only yields positive results when taken from areas with mucosal inflammation.61 Treatment is medical in a multidisciplinary approach and is tailored to the severity of the condition. This usually includes combinations of oral corticosteroids, macrolide antibiotics, methotrexate, and hydroxychloroquine and more recently infliximab according to the severity of the condition.62 Local nasal symptoms can be controlled by topical antibiotic ointments, nasal douching, and topical steroids, although the latter often worsens the bleeding episodes. Surgery is contraindicated in the presence of active disease because it will lead to further necrosis followed by excessive scarring and possible atrophic rhinitis. Endoscopic sinus surgery is generally only undertaken for the treatment of selected patients with secondary bacterial infections.63
Wegener granulomatosis is a multisystem disease of unknown etiology characterized by necrotizing granulomas of the upper and lower respiratory tracts, systemic vasculitis, and focal necrotizing glomerulonephritis. Wegener granulomatosis was first described by Klinger in 1932, and subsequently by Wegener in 1936 who established the classical triad of the condition.64,65 The incidence of this disease is difficult to quantify, but it is known to equally affect men and women between the ages 15 and 73 years. It has also been reported in children. The nose and sinuses are involved in 85% of patients, and nasal complaints are the most common presenting symptoms of all age groups.66 Patients present with nasal crusting, nasal obstruction, and epistaxis.66 Destruction of the intranasal structures including the nasal septum may follow, leading to nasal collapse. The destructive process is located initially in the midline, affecting the septum and turbinates, then spreads symmetrically to involve the maxillary and the rest of the sinuses.67 It is extremely rare for patients to present with an isolated lesion in the maxilla.68 Untreated, the disease may follow a relentless course, leading eventually to renal failure and significant mortality.62 A limited form of Wegener granuloma has also been described in the upper respiratory tract presenting with purely granulomatous form of the localized disease.67 It is unknown what proportion of these patients ultimately progress to classical, multisystem disease.66 A diagnosis of Wegener granulomatosis should be considered in patients who report levels of malaise, which are disproportionate to their upper respiratory tract symptoms and clinical findings.66 Serology for cANCA is positive in 95% of patients with generalized active disease and 60% of those with localized disease.66 In a patient without a history of previous sinonasal surgery, a combination of bone destruction and new bone formation on CT is virtually diagnostic of Wegener granulomatosis, especially when accompanied on MRI by a fat signal from the sclerotic sinus wall.67
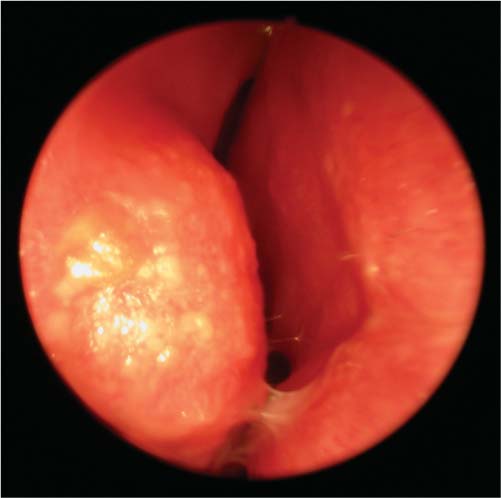
Fig. 9.7 An endoscopic photograph of the right nasal cavity in a patient with nasal sarcoidosis showing crusting, mucosal inflammation, and granulomas.
Like sarcoidosis, treatment is medical in a multidisciplinary approach with combination of high-dose systemic corticosteroids and a cytotoxic agent such as azathioprine, cyclophosphamide, or mycophenolate mofetil. Because of its greater side effects, cyclophosphamide is used mainly in patients with severe disease and in those with renal involvement. Immunoglobulin infusion and monoclonal antibodies, such as rituximab, are also being used. When the condition is controlled the medication can be reduced, but most patients require a maintenance low-dose corticosteroid. The nasal symptoms are managed as in patients with sarcoidosis. Reconstructive surgery is contraindicated when the disease is still in its active stage, but maxillary sinus exploration is sometimes undertaken in the presence of pain and opacification of imaging.

Fig. 9.8 Classical “lupus pernio” with purple skin discoloration and nodules.
Antrolithiasis
Antroliths are calcified bodies that are formed from a mineral salt deposition around a nucleus within the maxillary sinus cavity.69 They are synonymous with rhinoliths, which are reported within the nasal cavity. However, reports of antroliths are very infrequent compared with rhinoliths. It has been postulated that antroliths result from either endogenous or exogenous factors. Endogenous factors may include blood, mucus, or pus; exogenous factors include teeth and their roots or other foreign body material. It is assumed that these would initiate a foreign body reaction that would form the antrolith over a long period. The main components of antroliths are calcium phosphate, calcium carbonate, organic matter, and water.69 The lesions may also be covered by granulation tissue. The majority of cases reported in the literature had tooth extraction prior to the presentation. The patients can be asymptomatic and may present with symptoms of unilateral chronic maxillary sinusitis. On CT scanning, antroliths are radiopaque masses of varying sizes and shapes and irregular borders. They are usually surrounded by mucosal thickening and occasionally associated polyps or fluid level. Treatment is by surgical removal, which can generally be achieved through the endoscopic approach (Fig. 9.9) (see Video 9.4).
Neoplastic
Papillomas
Papillomas are the most common benign epithelial tumor found in the sinonasal region, accounting for up to 10% of all neoplasms in this area.70 Histologically, they are divided into inverted, cylindric, and everted.71 Everted and cylindric cell papillomas are true papillomas, lined by stratified squamous and microcyst-laden, columnar, and oncocytic epithelium, respectively.71 Inverted papillomas are polyps with marked, patchy squamous metaplasia in ductal and surface epithelium with extensive “inversion” of the epithelium into the underlying stroma.
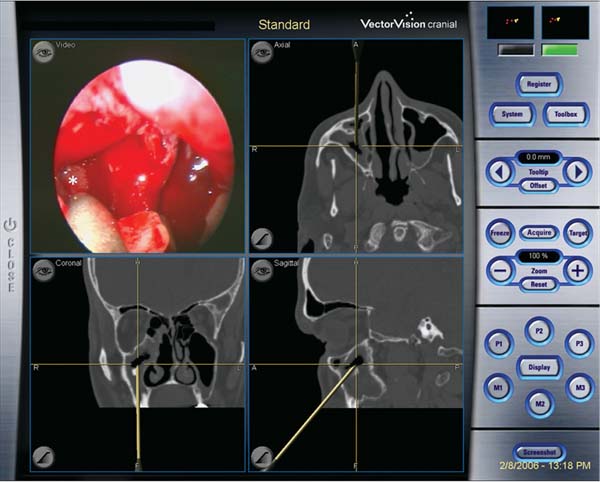
Fig. 9.9 An intraoperative screen shot from an image guidance system during removal of a right maxillary antrolith (asterisk) through a middle meatal antrostomy.
Everted papilloma more often arises on the nasal septum, whereas both inverted and cylindric papillomas mostly arise on the lateral nasal wall within the middle meatus. They most commonly extend into the maxillary sinus through an expanded natural ostium then to the ethmoids or frontal sinuses.70–73 It is not certain if some papillomas originate within the cavity of the maxillary sinus itself then spread into the middle meatus. The age presentation is from 35 to 60 years with male preponderance of 3.5:1.70,72 It appears to be more common in Caucasians compared with other racial groups. A viral etiology has been suggested with a link to papilloma viral subtypes 6, 11, 16, and 18.72 Patients generally present with obstructive nasal symptoms, rhinorrhea, and chronic rhinosinusitis.70,72 Inverted papilloma appears as a firm vascular polyp, which is sometimes mixed with normal nasal polyps. Cylindric papilloma appears as smooth fleshy polypoid mass and is much less common. The diagnosis is suggested on CT scans when there is a mass continuous from the middle meatus into the adjacent maxillary sinus, through an expanded maxillary ostium.73 The mass may contain areas of apparent calcification and there may be sclerosis of the walls of the sinus (Fig. 9.10).73 The main advantage of MRI is defining the extent of the tumor and differentiating it from adjacent inflammatory tissue.
Both a high recurrence rate and malignant transformation have been quoted repeatedly in the literature. A recurrence rate of up to 75% usually reflects inadequate excision whereas malignant transformation at rates from 0 to 53% suggests that the majority of these cases had squamous carcinoma ab initio. A recent review of the literature of over 200 cases calculated 7.1% synchronous carcinoma and 3.6% metachronous carcinoma.74
There is currently a growing body of evidence supporting endoscopic resection of these tumors.3,72,75 We believe that the approach that allows the most reliable total excision of the lesion is the most appropriate. In general, endoscopic excision (see Video 9.1), with or without medial maxillectomy, is suitable for most tumors except for those that invaded the lateral maxillary wall, frontal sinus, orbit, or skull base. Caldwell–Luc, lateral rhinotomy, or midfacial degloving are tailored to the individual lesion. It is most important that the resection is subperiosteal and that all sclerotic bone is removed—whatever the approach—to minimize recurrence. This is of the order of 10 to 15% irrespective of the approach in the larger series. Table 9.2 shows the overall recurrence rates based on our review of 31 series that included 1574 patients.

Fig. 9.10 A coronal computed tomography scan showing a inverted papilloma extending from the middle meatus into the maxillary sinus. Small areas of high density are seen within the maxillary component.
Salivary Gland Tumors: Pleomorphic Adenoma and Oncocytoma
Pleomorphic adenoma of the upper respiratory tract occurs almost exclusively in the nasal cavity with a very rare occurrence in the paranasal sinuses.76–78 There are only a very small number of reports of isolated tumors arising in the cavity of the maxillary sinus.76,77 Age presentation is usually between the third and sixth decade when occurring in the nasal cavity.78 Patients with maxillary pleomorphic adenoma present with facial swelling, nasal obstruction, and occasional palatal swelling.76,77 Bony expansion and erosion have been reported on CT scanning. Histology shows the typical feature of duct-like structures and myoepithelial cells within myxoid stroma.77 Surgical treatment is tailored to the extent of the tumor: both endoscopic and open approaches have been used. One series reported a high recurrence rate, highlighting the importance of complete excision via the most suitable route.76

Oncocytoma is exceedingly rare in the maxillary sinus.79 It is reported more frequently in the nasal cavity, but there is only a small number of cases in the literature.80 Oncocytoma is a term that describes a tumor composed of epithelial cells or myoepithelial cells with abundant granular eosinophilic cytoplasm. The peculiar appearance of these oncocytes is due to the large number of mitochondria in their cytoplasm as demonstrated on electron microscopy.80 The presentation is similar to pleomorphic adenoma, although oncocytomas can be more aggressive. Malignant transformation has also been reported. Surgical approach should be tailored to the extent of the tumor.
Mesenchymal Tumors: Fibroma, Lipoma, and Myxoma
These rare tumors may be encountered in the nose and sinuses and generally present prior to adulthood. Isolated tumors within the maxillary sinus are very rare. Fibromas result from progressive inflammation or fibroblastic proliferation of the nasal mucosa.81 They present as slow-growing, gray-white, smooth-surfaced masses producing obstructive nasal symptoms.
Lipoma is the most common soft tissue tumor in adulthood. It can be seen wherever there is adipose tissue. In contrast, intraosseous lipoma is a rare condition. The etiology of intraosseous lipoma is unknown, but infarction, ischemia, trauma, and irradiation may be contributing factors.82 Cases have been reported within the nasal cavity and very rarely in the maxillary sinus. The presentation is of a facial swelling and possible nasal obstructive symptoms.
Myxoma of the maxillary sinus is very rare, but has been reported more frequently than fibromas and lipomas.83 The age at presentation is between 2 and 15 years. They may be related to dental malformations or missing teeth, but may also occur without such abnormalities. Histologically, there is a myxomatous background surrounding a hypocellular proliferation of small stellate or spindle-shaped cells with regular nuclei and a variable amount of cytoplasm. They are locally aggressive with a high recurrence rate when locally excised.
Vasiform Tumors: Hemangioma, Aneurysmal Bone Cyst, and Hemangiopericytoma
These benign lesions originate from vascular tissue within the mucosa or bone of the nose and sinuses. Hemangiomas are said to represent 20% of benign nonepithelial tumors of the nasal cavity and paranasal sinuses.84 Mean age at diagnosis is 40 years and the most frequent presenting symptoms are nasal obstruction and epistaxis. Those that originate in the maxillary sinus have been reported less frequently.84 Both cavernous and capillary hemangiomas have been reported with no apparent difference in the pattern of presentation.84,85 CT scanning is nonspecific and show features of expansion similar to other benign conditions. The lesion can bleed profusely during surgical excision and preembolization has been suggested by some.85
Aneurysmal bone cysts (ABCs) are expansile lesions of unknown etiology that usually affect long bones and vertebrae of patients younger than 20 years. About 2% of ABCs are encountered in the head and neck region with the jaw being the most frequently involved site. An ABC of the maxillary sinus may be associated with other bone pathology such as fibrous dysplasia; isolated lesions have rarely been reported.86 They present with facial swelling and obstructive nasal symptoms in the age group between 5 and 23 years. Histologically, ABCs consist of multiple cavities filled with blood and serous fluid, which are separated by septa and surrounded by a rim of bone.86 The septa are composed of fibroblasts, myofibroblasts, giant cells, osteoid and woven bone and are not lined by endothelium. It is postulated that preexisting bone lesions may cause venous occlusion or an arteriovenous malformation; the consequent change in hemodynamics leads to the ABC formation.87 CT shows a multiloculated, heterogeneous contrast-enhancing mass surrounded by a thin rim of bone, which expands the maxillary sinus. Fluid-fluid levels may be seen on CT or MRI. ABCs have a “honeycomb” appearance on gadolinium-enhanced MRI studies.86 The cysts can be treated endoscopically, although the long-term prognosis of these lesions is unknown due to their rarity.
Hemangiopericytoma (HPC) is a rare vascular tumor derived from extracapillary cells (pericytes), which surround normal vascular channels. Less than one-third of HPC occur in the head and neck and 5% are located in the nasal cavity and paranasal sinuses.88,89 Sphenoid and ethmoid sinuses are involved more frequently than the maxillary sinus. It affects males and females equally and can occur at any age, but it most often develops after the second decade. The patients usually present with epistaxis and nasal obstruction with reddish submucosal nasal mass. CT and MRI show nonspecific features of a nasal mass. Histologically, they are characterized by sheets or randomly scattered ovoid or spindle-shaped cells with indistinct cytoplasm and large nuclei, distributed around normal vascular channels. HPC of the nose is considered benign, but some forms of the tumor affecting other sites are malignant. Late recurrence rates of 25 to 50% have been reported with systemic metastases in up to 10% of patients. Mortality has been reported as high as 50% after 5 to 20 years. Wide local excision is therefore recommended with long-term follow-up.
Tumors of Muscle Origin: Leiomyoma and Rhabdomyoma
Leiomyoma is a smooth muscle tumor that originates in areas of abundance of such muscle like the uterus. It is extremely rare for these tumors to present in the sinonasal tract because of the paucity of smooth muscle. Only a handful of cases of leiomyoma have been reported in the maxillary sinus.90 When present, it has been suggested that they originate from undifferentiated mesenchyme muscle elements in the wall of blood vessels or both. The presentation is of obstructive nasal symptoms and the tumors seem to be slow-growing and nonaggressive. The few reported cases did not seem to show any evidence of recurrences after excision.
Rhabdomyoma is a skeletal muscle tumor; hence, it is exceedingly rare in the nose and sinuses. Only a handful of historic case reports exist; they describe the rhabdomyoma’s benign behavior and low recurrence rate.91,92
Odontogenic Tumors
Odontogenic tumors are derived from the epithelial, ectomesenchymal, or mesenchymal components that are part of tooth development.93 They originate either within the maxillofacial skeleton (intraosseous) or within the gingival or alveolar mucosa overlying the tooth-bearing areas (extraosseous). Odontogenic tumors of the maxillary sinus are usually slow growing and have been associated with the noneruption of teeth. Patients usually present with swelling of the alveolar process along with nasal obstruction and epistaxis. Superior displacement of the globe has been reported with large odontogenic tumors. The location and behaviors of the tumors vary according to their subtype. Table 9.3 is adapted from the revised World Health Organization’s (WHO) classification of odontogenic tumors.94
Ameloblastoma is the most common odontogenic tumor. It originates from epithelial components of the embryonic tooth arrested developmentally prior to enamel formation. It is slow growing, locally invasive and has a high rate of recurrence if not treated effectively. Patients between the ages of 16 and 60 years are generally affected, with the region of the canine tooth and maxilla being the most common sites. They are often asymptomatic, but can present with a painless swelling of the cheek, gingiva, and palate that may reach a large size. Radiologically, ameloblastoma presents as a unilocular or multilocular radiolucency that may be associated with an impacted tooth. Treatment includes excision with a margin of uninvolved tissue. This is preferable to enucleation or curettage, which are associated with a high recurrence rate.93
Fibroosseous Lesions: Osteoma, Ossifying Fibroma, Fibrous Dysplasia, and Osteoblastoma
Fibroosseous lesions represent a class of bony abnormalities: osteoma, ossifying fibroma, fibrous dysplasia, and osteoblastoma. They are distinct but lie along a continuum from the most to the least bony content. They do have some similarities in appearance, but their clinical implications differ.
Osteomas are a frequent incidental finding in up to 3% of CT scans of the paranasal sinuses.95 Eighty percent occur in the frontal sinuses followed by the ethmoids; they are least found in the maxillary sinuses. Their etiology is still debated, with suggestions that they are either embryologic, or secondary to traumatic or an infective process. There is an association with Gardner syndrome, which is an autosomal dominant condition characterized by intestinal polyposis and pigmented skin lesions in addition to the osteomas.96 Maxillary sinus osteomas are slow growing and usually asymptomatic, but they may become symptomatic depending on the location and onset.97 Treatment is only required if they produce cosmetic problems or symptoms related to mass effect. Depending on their extent and location, this can be done via an endoscopic approach or an open procedure.
Ossifying fibroma (OF) is an expansible well-circumscribed lesion that continues to grow after sexual maturity and can attain dramatic proportions.95,98 Variants of ossifying fibroma include cementoossifying fibroma, which occurs in relation to dentition; psammomatoid ossifying fibroma and juvenile ossifying fibroma, which can be locally destructive.95 The vast majority is located in the posterior region of the mandible; those involving the maxillary sinus are uncommon.99 Patients usually present between the third and fourth decades and the lesion is more common in women.99 The most common presentation is of a painless cheek swelling, but involvement of the orbit or nasal cavity may be signified by proptosis, loss of visual acuity, epiphora, nasal obstruction, and epistaxis.95,99 Radiologically, the lesion is sharply circumscribed with an eggshell rim and central radiolucency (Fig. 9.11). This differentiates it from fibrous dysplasia, which has indistinguishable borders. The histologic features can be difficult to discriminate from those of fibrous dysplasia.98 Because of the progressive and locally destructive nature of OF complete surgical excision is recommended.
Epithelial Odontogenic Tumors | Mixed Epithelial and Mesenchymal Odontogenic Tumors | Mesenchymal Odontogenic Tumors |
|---|---|---|
Ameloblastoma | Ameloblastic fibromas | Odontogenic fibromas |
Calcifying epithelial odontogenic tumor (Pindborg tumor) | Odontoma Calcifying cystic odontogenic tumor (Gorlin cyst) | Odontogenic myxoma |
Adenomatoid odontogenic tumor |
|
|
Keratocystic odontogenic tumor |
|
|
Source: Data from Barnes L, Eveson JW, Reichart PA, Sidransky D, eds. World Health Organization classification of tumors: pathology and genetics of tumors of the head and neck. Lyon: IARC; 2005.
Fibrous dysplasia (FD) is a slow, progressive disorder where normal bone is replaced by fibrous tissue and immature woven bone.95,98 There are two main forms of FD: monostotic (70–85%) that involves only one bone, and polyostotic (15–30%) where multiple bones are involved. A variant of the polyostotic form is the McCune–Albright syndrome (precocious puberty, FD, and cafe-au-lait spots).95 The maxilla and mandible are the most commonly involved bones generally in the monostotic form. FD is a disease of young age where patients present in their first or second decade and is assumed to “burn out” as the patients reach skeletal maturity. The usual symptom is of painless facial deformity although other complaints such as loosening of teeth, nasal obstruction, or epistaxis have been encountered.100 CT scans show lesions with indistinct borders and an homogeneous “ground glass” appearance representing disorganized spicules of bone (Fig. 9.12).95 Histologically normal bone is replaced by fibrous tissue with varying degrees of osseous metaplasia. Diagnosis is undertaken on the combination of the clinical picture, radiology, and histology as the latter can be indistinguishable from ossifying fibroma. Treatment is conservative due to the expected natural cessation of the lesion, usually in the third or fourth decades. Where there are significant symptoms or severe deformity, recontouring of the affected bone can be undertaken. The lesions are usually very vascular and surgical intervention can be difficult. Some authors have showed regression of lesions on using the bisphosphonate pamidronate, but caution is needed as there are case reports of avascular necrosis.101,102
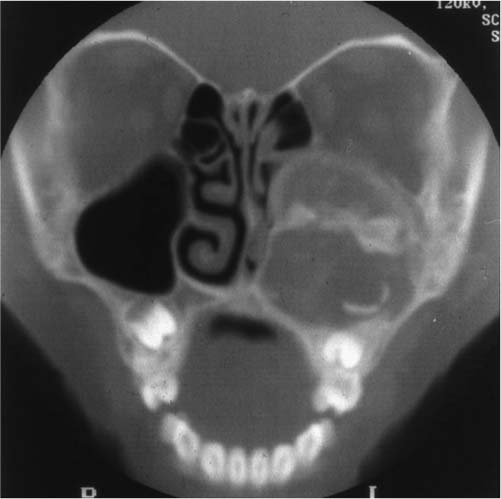
Fig. 9.11 A coronal computed tomography scan of a patient with ossifying fibroma in the left maxillary sinus.
Osteoblastoma is an uncommon neoplasm characterized by proliferation of osteoblasts forming bone trabeculae set in a vascularized fibrous connective tissue stroma.103 The tumor occurs predominantly in vertebrae and long bones and can affect craniofacial bones, with the mandible being the most commonly involved. It is reported less in the maxillary bone and rarely in the maxillary sinus.104 The majority of patients are under the age of 30 years and present with a facial swelling that is often painful.103 CT features range from radiolucent to radiopaque lesions and are often mistaken for other fibroosseous lesions (Fig. 9.13).103 Diagnosis is therefore mainly histologic and treatment is by surgical excision.
Neuroectodermal Tumors: Schwannoma and Neurofibroma
Schwannomas are benign peripheral nerve sheath tumors of which 50% occur in the head and neck region. They are very uncommon in the paranasal sinuses with only 4% estimated in this area; a very small number involve the maxillary sinus.105 The lesion slowly expands in the sinus cavity resulting in swelling, pressure symptoms, and bony necrosis. Cystic lesions that are associated with sudden bursts of worsening symptoms have also been reported.105 The patients mostly present with nasal obstruction, but other symptoms such as proptosis, epiphora, headaches, facial anesthesia, and epistaxis have been reported.106 CT scanning shows a homogeneous radiopaque mass with evidence of bone destruction. On MRI they appear as hyperintense well-demarcated masses. Histologically, they exhibit characteristic features of schwannomas and are typically positive to S100 protein. Treatment is by local excision via the most suitable approach.

Fig. 9.12 A coronal computed tomography scan showing a typical fibrous dysplasia affecting the right maxillary sinus. Note the “ground glass” appearance and the indistinct borders.
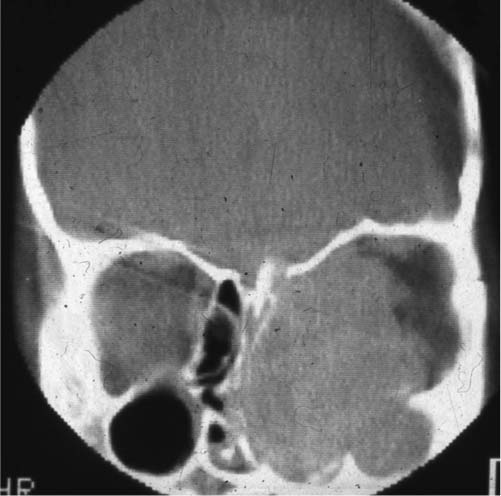
Fig. 9.13 A coronal computed tomography scan of a patient with a very large osteoblastoma in the left maxillary sinus.
Neurofibromas are heterogeneous peripheral nerve sheath tumors that arise from the connective tissue of the nerves, especially the endoneurium.107 They may occur as sporadic lesions but are much more common in association with neurofibromatosis type 1 (NF1). Neurofibromas of the maxillary sinus are exceedingly rare with only a small number of reported cases. As for schwannomas, they slowly grow and expand within the cavity of the sinus causing swelling, pressure symptoms, and bone necrosis. Presentation is similar to other expanding masses in the maxillary sinus. CT scanning shows a well-circumscribed mass with some bony erosion. On MRI, neurofibromas are usually isointense or of lower intensity than gray matter on T1-weighted images and are isointense or of higher signal on T2-weighted images.107 Histologically, they are differentiated from schwannomas by the lack of the palisade pattern of the nuclei and the lower tumor cell density. Treatment is by local excision.
 Conclusion
Conclusion
The maxillary sinus is a unique structure which can be involved in a large number of benign pathologies. Some are more aggressive than others and some have higher recurrence rates. A systematic approach to diagnosis with a high index of suspicion and an awareness of uncommon lesions is therefore essential. An armamentarium of surgical approaches is at our disposal; each is applicable to certain situations. The surgeon should be adept with these techniques and prepared to interchange between them to suit particular lesions. Finally, long-term follow-up is essential in many cases and should not be overlooked.
• The maxillary sinus may be affected by a variety of benign pathologies.
• Symptoms are mostly nonspecific and can be similar to maxillary sinusitis.
• Some lesions can lead to facial swelling.
• Imaging is helpful and can be characteristic in some cases, but diagnosis is often based on histopathology.
• Surgery is the mainstay of treatment in the majority of cases.
• Long-term follow-up is often necessary because of the high incidence of recurrence of some pathologies.



