 y colleagues and I have successfully used the Fugo blade to remove a large nevus along the limbus of a 2-year-old patient.
y colleagues and I have successfully used the Fugo blade to remove a large nevus along the limbus of a 2-year-old patient.
TECHNIQUE
Anesthesia
Administer general anesthesia.
Surgical Technique
- At 2 mm away from the nevus, puncture the conjunctiva with a 100- µm Fugo blade. Through this opening, introduce a 30-gauge cannula and inject saline to balloon the conjunctiva and lift it from the surface of the sclera. Using a cannula instead of a needle prevents subconjunctival bleeding (Fig. 11.1).
- Make an incision in the ballooned conjunctiva with the same Fugo blade tip about 1 mm from the edge of the lesion. If the conjunctiva flattens out before the incision can be completed, lift it away from the sclera with a forceps and then cut. Do not touch the sclera.
- Touch any blood vessel coursing toward the lesion seen in the subconjunctival tissues with a 600- µm Fugo blade tip set at low energy.
- Life the nevus and dissect it toward the limbus with a 100- µm Fugo blade tip until the limbus comes in to view. Once again, touch any visible blood vessel with a 600- µm tip set at low energy.
- Use corneal scissors to excise the conjunctiva carrying the nevus, right up to the cornea. The nevus can be removed completely with this technique. A small portion of pigment might still be visible.
- To make certain that no nevus tissue is left, momentarily touch the suspected area of the limbus with the 600- µm tip.
- Undermine the incised conjunctiva with scissors. Bring the conjunctiva forward and suture it to the sclera. Some bare sclera is inevitable at the end of the surgery, but it will be covered up during the postoperative period.
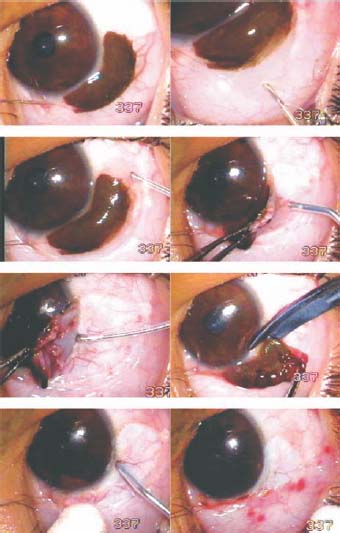
Figure 11.1. Excision of a large limbal nevus. The conjunctiva is ballooned and incised with a 100- µm tip around the lesion. The 600- µm tip ablates the underlying blood vessels. The nevus-carrying conjunctiva is excised with the scissors. The remnant of the nevus is ablated with the 600- µm tip. The undermined conjunctiva is brought forward and sutured to the sclera, leaving some bare sclera.
Summary
A limbal nevus can be removed using forceps, scissors, and bipolar cautery, but at the risk of excessive tissue trauma. Excision of a nevus using the Fugo blade can be done with finesse, precision, and little or no tissue trauma.
Suggested Reading
Kellan R, Fugo RJ. Device increases safety, efficiency of cataract surgery. Ophthalmol Times. 2000;25:7–9.
Roy FH. Course for Fugo blade is enlightening, surgeon says. Ocular Surg News. 2001;19:35–38.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


