Chapter 58 Auditory Implants for the Central Nervous System
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
General technical and theoretical considerations of central auditory implantation and stimulation have been reviewed elsewhere.1,2
PATIENT SELECTION
Patients originally received the ABI under a protocol monitored by the FDA. The criteria for implantation are listed in Table 58-1. The device originally was designed for patients with NF-2 manifesting bilateral vestibular schwannomas, although others with compromised auditory nerves were considered to be eventual ABI candidates. At least 90 per cent of NF-2 patients exhibit bilateral eighth nerve neuromas.3 An unpublished review of patients with NF-2 seen at the House Ear Clinic revealed that two thirds had bilateral internal auditory canal–cerebellopontine angle (CPA) tumors alone or with one other tumor as the only central nervous system manifestation of their disease. The patients were young (average age, 28 years). With improvements in medical care and surgical techniques, the life span of most of these patients has been significantly prolonged. Restoration of even rudimentary auditory function can enhance their quality of life and ability to function in a hearing world. Our results have shown that the multichannel ABI has the potential of offering even greater benefit.
TABLE 58-1 Criteria for Implantation
| Evidence of bilateral seventh and eighth cranial nerve tumors |
| involving the internal auditory canal or cerebellopontine angle |
| Language competency |
| Age 12 years or older |
| Psychologic suitability |
| Willingness to comply with research follow-up protocol |
| Realistic expectations |
The management of bilateral acoustic neuromas should be highly individualized.4 Hearing preservation remains an ideal goal in the management of these tumors in patients with NF-2, and early identification and treatment have permitted this in a number of cases. An intact auditory system is highly desirable in preference to an artificial means of restoring hearing. Therefore, preserving as much of the patient’s own hearing as possible is paramount. Patients meeting the criteria listed in Table 58-2 may be considered and observed accordingly. The availability of the ABI provides an alternative to a desperate attempt to preserve nonserviceable hearing when large tumors are removed and hearing conservation is unlikely.
TABLE 58-2 Criteria for Observation in Auditory Brainstem Implant Candidacy in Patients with Neurofibromatosis Type 2
| Second tumor in an only-hearing ear |
| Any tumor in a hearing ear that measures >2 cm in the largest diameter (hearing preservation unlikely with removal) |
| Short life expectancy due to other tumors, medical problems, or advanced age |
| Serviceable hearing with a tumor that shows no significant growth by sequential magnetic resonance scans and stable hearing by serial audiograms |
DEVICE
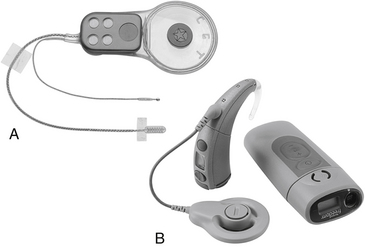
The ABI hardware has evolved through a number of modifications since the original ball electrode was inserted by Drs. William Hitselberger and William House in 1979.1,5 Significant design changes have involved transitioning from a percutaneous connector to a transcutaneous coil link to the implant, converting from ribbon electrodes to .7-mm-diameter disk electrodes, and fabrication of a semiflexible silicone electrode carrier (2.5 × 8.5 mm) with a specialized mesh backing to stabilize placement. The first 25 ABI recipients were fitted with a single-channel sound processor and a 2-or 3-electrode array. From 1992 until about 2000, the electrode array used in most patients employed eight platinum disks in a perforated silicone and mesh carrier connected to an implantable receiver/stimulator. From about 2000 to the present, the 21 electrode Nucleus ABI24 (see Fig. 58-1) has been used. The external device in the 8 electrode patients consisted of a post-auricular microphone, a transcutaneous transmitter coil, and a sound processor (Spectra Model, Cochlear Corporation). Signal-processing strategies have evolved in an effort to improve performance.6 Present patients receive a 21-electrode array (Fig. 58-1A and B) interfaced with the Freedom post-auricular sound processor and ear-level or body-worn controller (Cochlear Corporation, Englewood, CO).
Since 2003, use of a hybrid ABI array consisting of a version of the present surface electrode and a 10-electrode penetrating array also has been studied in an FDA clinical trials. Implementation of this system in laboratory animals originally demonstrated the capability for improved microstimulation of auditory neurons7 and possibly improved perceptual performance in humans.
ANATOMIC CONSIDERATIONS
The target of the ABI electrodes is the cochlear nucleus complex—dorsal and ventral cochlear nuclei. In humans, the cerebellar peduncle that forms the base of the pons covers the auditory nuclei. This means that the nuclei are not visible to the surgeon and must be located from surface landmarks. Figure 58-2 illustrates the major structures of the pontomedullary junction region with the translabyrinthine approach surgical field of view within the dashed lines. The terminus of the sleeve-like lateral recess forms the foramen of Luschka. Just inferior to the foramen is the root of the glossopharyngeal (ninth) nerve. Superior to the foramen lie the root entry and exit zones of the vestibulocochlear and facial nerves. This area is frequently distorted by the tumor.
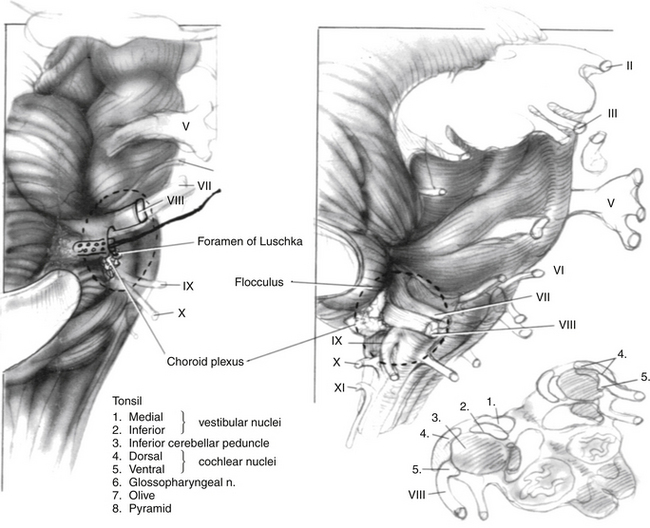
The cochlear nuclei come closest to the surface of the brainstem within the medial and superior aspect of the lateral recess.8,9 The main target for stimulation is the ventral cochlear nucleus, which forms the main relay for cochlear nerve input and the greater part of the ascending auditory pathway. Placement of the electrodes within the recess has resulted in the fewest side effects and preserves auditory stimulation even though some part of the electrode array lies adjacent to the dorsal cochlear nucleus.2 Also, the disadvantage of lack of exposure is partially offset by positional stability provided to the electrode carrier by the limited space in the lateral recess.
SURGICAL CONSIDERATIONS
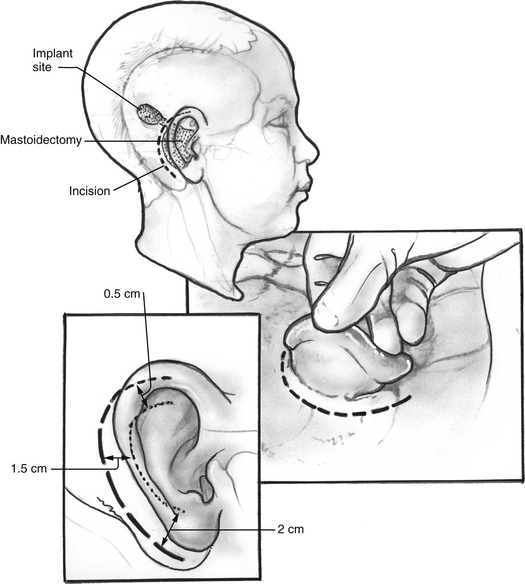
The surgical approach for tumor removal in ABI cases at HEI has been exclusively via translabyrinthine craniotomy (see Chapter 50). The translabyrinthine route has been found to provide the most direct access to the lateral recess and surface of the cochlear nuclei.10 Until the actual placement of the device, the surgery proceeds as in any other translabyrinthine acoustic neuroma excision, with the following exceptions. Electrodes are placed for recording electrically evoked auditory brainstem responses (EABRs) and for monitoring cranial nerves VII and IX. The postauricular incision used is shown in Figure 58-3. It is important that the incision not cross the receiver/stimulator package.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


