CHAPTER 210 Aspiration and Swallowing Disorders
Evaluation of Infants and Young Children with Suspected Dysphagia
Instrumental Evaluation
Videofluoroscopic Swallow Study
VFSS, sometimes referred to as a modified barium swallow study, may be useful in children suspected to have oropharyngeal dysphagia because it images the structures of the oral cavity, pharynx, and cervical esophagus during deglutition.1 VFSS may screen gastrointestinal structures distal to the cervical esophagus. The goals of VFSS are to provide information that helps determine whether anatomic or structural abnormalities are present; ascertain if coordination of the structures and functions of the upper aerodigestive tract supports safe and efficient bolus passage; and identify strategies that enhance the safety and efficiency of feeding, while minimizing the dysphagic problems. During VFSS, children ingest liquids or foods or both impregnated with barium contrast material to simulate functional feeding as closely as possible. Consequently, children must be ready, willing, and able to cooperate with VFSS.2,3
Flexible Endoscopic Evaluation of Swallowing
FEES is an extension of the routine flexible fiberoptic nasopharyngolaryngoscopy examination, and may be used to evaluate the structures and functions of the nasopharynx, oropharynx, and larynx during phonation, spontaneous swallows, and swallows of liquids and foods.4,5 FEES may be particularly useful in children who are nonoral feeders, who are unable to cooperate with VFSS, who have vocal fold dysfunction, or in whom their ability to handle their secretions is questionable.
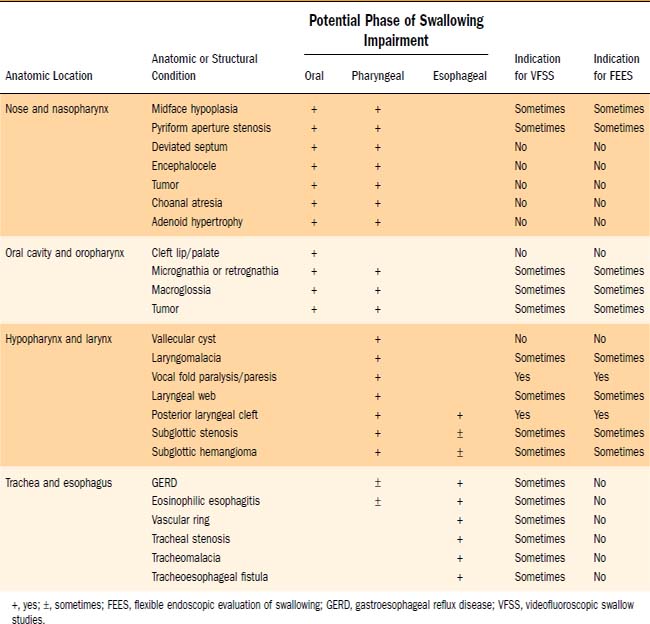
FEES may provide sensory information when the endoscope touches adjacent mucosa or structures. To standardize evaluations of responses to sensory input, calibrated air pulses have been administered endoscopically.6 The utility of FEES plus sensory air pulse testing (FEES-ST) has been shown during the evaluation and treatment of children with specific diagnostic conditions (e.g., type I laryngeal clefts) and during preoperative evaluations for pediatric airway reconstruction.7,8 Elevated laryngopharyngeal sensory thresholds have been documented in children with clinical diagnoses of recurrent pneumonia, neurologic disorders, and gastroesophageal reflux disease (GERD).6 Table 210-1 outlines the utility of using VFSS and FEES based on the anatomic or structural condition.
Four Anatomic Sites of Dysphagia
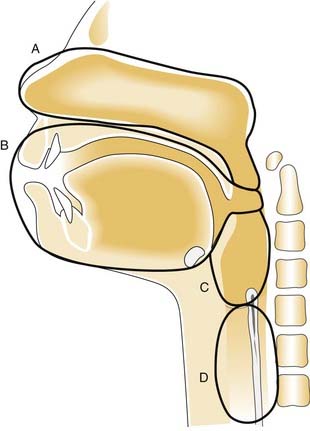
The four primary anatomic sites with anomalies of the aerodigestive tract that may adversely affect swallowing and contribute to dysphagia are the nose and nasopharynx, oral cavity and oral pharynx, hypopharynx and larynx, and trachea and esophagus (Fig. 210-1).
Nose and Nasopharynx
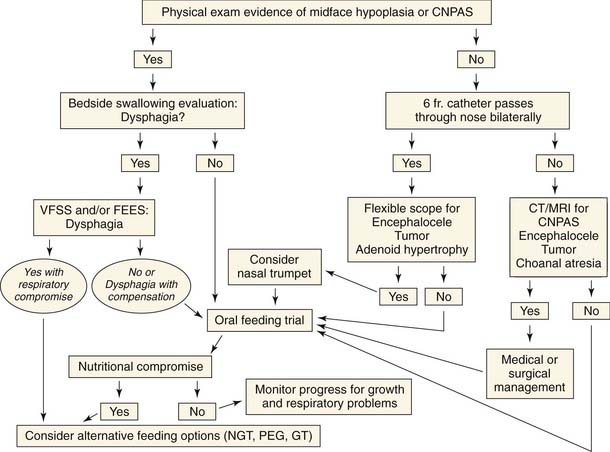
Anomalies of the nose and nasopharynx affect the oral and pharyngeal phases of swallowing. Dysphagia from anomalies of the nose and nasopharynx is secondary to upper airway obstruction and the caliber of the upper airway and the child’s ability to compensate while swallowing (Fig. 210-2). Bilateral disease has a more significant impact on airway patency and swallowing than unilateral disease.
Any cause of nasal airway obstruction can lead to feeding difficulties, particularly during infancy when nasal airflow is an important component of breathing and feeding. Nasal obstruction can result from myriad conditions, including midface hypoplasia, congenital nasal pyriform aperture stenosis, septal deviation or hematoma, chronic or acute rhinitis, congenital midline nasal masses (including dermoids, encephaloceles, and gliomas), nasal or nasopharyngeal tumors, choanal atresia, and adenoidal hypertrophy. These children frequently have difficulty coordinating feeding and breathing, and may have failure to thrive or recurrent aspiration.9
Unilateral nasal disease may not be detected for years and is often associated with unilateral nasal congestion or rhinorrhea. Bilateral disease has a more significant impact on airway patency and swallowing than unilateral disease and is usually recognized soon after birth because the child commonly has severe respiratory difficulties with cyclical cyanosis relieved by crying.10 These children are also unable to feed effectively, and may have coughing and choking with cyanotic spells when attempting to eat. Diagnostic evaluation often starts with attempted passage of a 6F feeding tube through the nares. A thorough evaluation with flexible fiberoptic endoscopy and imaging should be carried out if nasal obstruction is suspected. Figure 210-2 outlines the evaluation for children with dysphagia that is suspected to originate from the nose and nasopharynx.
Oral Cavity and Oral Pharynx
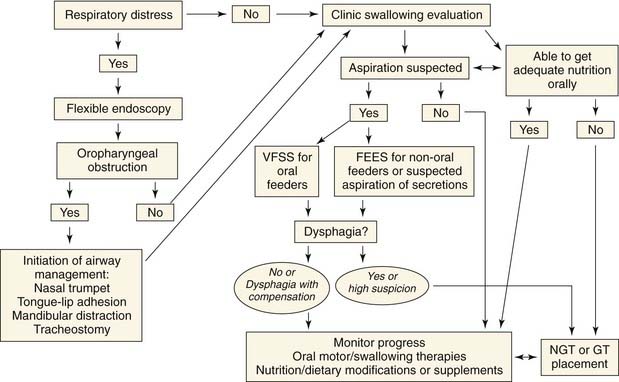
Anomalies of the oral cavity and oral pharynx may affect the oral and pharyngeal phases of swallowing, and many have the potential for upper airway obstruction. The respiratory issues should be evaluated and stabilized before initiating the feeding efforts or evaluations for suspected dysphagia (Fig. 210-3).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


