Purpose
To describe the relationship of lung disease and function with early age-related macular degeneration (AMD) in a population-based study.
Design
A population-based, cross-sectional study of 12 596 middle-aged participants from the Atherosclerosis Risk in Communities Study.
Methods
Lung function was assessed by spirometry. Physician diagnosis of asthma and lung disease was ascertained from a standardized questionnaire. AMD signs were graded from fundus photographs according to the Wisconsin grading protocol.
Results
Among the study population, 587 (4.7%) had early AMD, 638 (5.1%) had asthma, and 581 (4.6%) had lung disease. After adjusting for age, gender, smoking, and hypertension, each 1-L increase in predicted forced expiratory volume in 1 second (odds ratio [OR], 1.27; 95% confidence interval [CI], 0.89 to 1.80), forced vital capacity (OR, 1.18; 95% CI, 0.93 to 1.51), and peak expiratory flow rate (OR, 1.12; 95% CI, 0.95 to 1.33) were not significantly associated with early AMD. Forced expiratory volume in 1 second-to-forced vital capacity ratio (second quartile OR, 1.61; 95% CI, 0.88 to 2.93, third quartile OR, 1.65; 95% CI 0.90 to 3.03; fourth quartile OR, 1.28; 95% CI 0.68 to 2.40) was not associated significantly with early AMD. Similarly, asthma (OR, 1.06; 95% CI, 0.86 to 1.27) and other lung diseases (OR, 1.08; 95% CI, 0.90 to 1.29) were not associated with early AMD.
Conclusions
Our data do not support a cross-sectional association between lung disease and risk of early AMD.
Age-related macular degeneration (AMD) is a leading cause of irreversible blindness in the United States, affecting more than 8 million Americans. Despite ongoing research, the pathogenesis of AMD remains incompletely understood. Cigarette smoking is a modifiable risk factor that has been associated consistently with AMD. Aside from age, smoking, and genetic factors, few risk factors have been found to be associated with this condition in epidemiologic studies.
Two population-based studies reported poorer lung function and a history of chronic lung disease (e.g., emphysema) to be associated with the risk of AMD. More than 3 decades ago, the Framingham Eye Study first observed a significant association between decreased vital capacity and a history of lung infection with prevalent cases of AMD. Two subsequent case-control studies failed to replicate this relationship. More recently, the Beaver Dam Eye Study provided new data demonstrating that participants with emphysema at baseline were more likely to develop retinal pigment epithelial (RPE) depigmentation, a sign of early AMD (odds ratio [OR], 2.5; P = .006), and late AMD (OR, 3.0; P = .04) over a 15-year period. In addition, a history of mild respiratory symptoms, such as cough, phlegm, and wheezing, was associated with the 5-year incidence of exudative AMD and progression of AMD. These associations were shown to be independent of smoking and other risk factors Furthermore, in an earlier cross-sectional study, Klein and associates reported poorer lung function to be associated with the prevalence of AMD. These findings suggests that lung disease and poorer lung function could contribute to AMD risk, possibly via mechanisms related to inflammation and hypoxia. In the Atherosclerosis Risk in Communities (ARIC) study, we examined the cross-sectional relationship between lung disease or function and early AMD in a large population-based sample of white and black persons in the United States.
Methods
Study Population
The ARIC study is a population-based study of 15 792 persons 45 to 64 years of age selected from 4 United States communities. Of the baseline participants, 14 346 returned for the second examination (1990 through 1992) and 12 887 returned for the third examination (1993 through 1995). At second examination, lung function was assessed in participants using a spirometry; predicted force-expiratory volume in 1 second (FEV 1 ; in liters), predicted force vital capacity (FVC; in liters), predicted peak expiratory flow rate (in liters), and percentage predicted FEV 1 -to-FVC ratio (%). Lung disease variables were collected through physician-administered questionnaires; asthma and lung disease (defined as chronic bronchitis, emphysema, or spirometrically detected chronic obstructive pulmonary disease) were identified according to the Global Initiative on Obstructive Lung Disease classification.
At the third examination, early AMD was recorded using retinal photography and included soft drusen, pigmentary change, or both. Potential confounders included age, gender, race, smoking, hypertension, and the examination center.
Study Number
Our study was based on the 12 887 ARIC participants who returned for the third examination, excluding 291 participants, leaving 12 596 participants in the current study. Exclusion criteria included race neither white nor black (n = 213), incomplete data for lung function assessment (n = 29), ungradable retinal photographs (n = 32), and late AMD (n = 17). Late AMD was excluded as an outcome because the numbers available were too small for meaningful analyses.
Retinal Photography and Age-Related Macular Degeneration Grading
The assessment of AMD in the ARIC study has been reported previously. In brief, a 45-degree nonmydriatic retinal photograph centered on the region of the optic disc and the macula of 1 randomly selected eye was obtained after 5 minutes of dark adaptation. Graders, masked to the subject’s identity, evaluated the photographs for AMD based on a simplified version of the Wisconsin AMD grading system. The presence of soft drusen, RPE depigmentation, increased retinal pigment, pure geographic atrophy, and signs of exudative macular degeneration were determined. Soft drusen was defined as those having a diameter larger than 63 μm. Early AMD was defined as the presence of either soft drusen alone, RPE depigmentation alone, or a combination of soft drusen with increased retinal pigment, RPE depigmentation in the absence of late AMD, or both. Late AMD was defined as the presence of exudative AMD or pure geographic atrophy. Quality control procedures, based on repeated assessment of 520 photographs, showed weighted κ values of 0.67 to 0.81 for intragrader comparisons and 0.55 to 0.92 for intergrader comparisons.
Lung Function Assessment
Lung function was measured according to a standard protocol, with the use of a Collins Survey II volume-displacement spirometer (Warren E. Collins, Braintree, Massachusetts, USA). The technicians were trained and certified, and their performance was monitored closely by the staff of the pulmonary function reading center. During at least 5 forced expirations, the technician attempted to obtain 3 acceptable spirograms at least 2 of which had similar results (within 5%) for FEV 1 and FVC. At the reading centre, the technician observing the volume-time spirograms correlated these findings with the acceptability and reproducibility of the spirograms as indicated by the computer program. The largest FEV 1 and the largest FVC on any of the acceptable tests were used. Sex-specific predicted values for FEV 1 and FVC, adjusted for age and height, were computed from the equations of Crapo. For black persons, equation-derived predicted FEV 1 and FVC were multiplied by 0.88.
Definitions of Other Variables
At baseline and second visits, all participants had comprehensive examinations to assess cardiovascular risk factors. Blood pressure was computed from the average of the second and third readings using a standardized Hawksley random-zero instrument. Hypertension was defined as systolic blood pressure of 140 mm Hg or more, diastolic blood pressure of 90 mm Hg or more, or self-reported use of antihypertensive medication. Cigarette smoking status was obtained from standardized questionnaires with the following questions: (1) Have you ever smoked cigarettes? and (2) Do you now smoke cigarettes? Persons were categorized as current smokers if they answered yes to questions 1 and 2, former smokers if they answered yes to question 1, and never smokers if they answered no to question 1. Never and former smokers were classified further as exposed to environmental tobacco smoke if they reported being in close contact with smokers for more than 1 hour per week.
Statistical Analysis
Odds ratios (ORs) and 95% confidence intervals (CIs) were reported for the association between lung function (predicted FEV 1 -to-FVC ratio [%] quartiles, predicted FEV 1 [in liters], predicted FVC [in liters], and predicted peak expiratory flow rate [in liters]) and lung disease (physician-diagnosed asthma or lung disease) and early AMD. Lung function and disease exposures were analyzed for the entire cohort first. Interaction with gender was explored using the likelihood ratio test. Two models were created: model 1 was adjusted for age and gender, and model 2 was adjusted further for race, smoking, hypertension, and study site. Interaction with race for the association across predicted FEV 1 -to-FVC ratio quartiles and early AMD was tested in both models. The analyses were stratified further by race because of an interaction between race and lung function variables on the odds of AMD and the purposeful oversampling of blacks in the study design. Two models were created: model 1 adjusted for age and gender, and model 2 adjusted further for smoking, hypertension, and study site. Stata IC version 10.0 (StataCorp LP, College Station, Texas, USA) was used for all analyses.
Results
Table 1 shows the baseline demographic characteristics of the ARIC study sample by age, with a cutoff at 57 years. There were significantly larger proportions of male, female, and black persons in the younger age group. Younger participants also were more likely to be current smokers. The mean FEV 1 -to-FVC ratio was higher among younger study participants ( P < .001). The prevalence of lung disease early AMD and hypertension was higher within the older age group ( P < .001).
| Age (years) | P Value a | ||
|---|---|---|---|
| 46 to 57 (n = 6801) | 58 to 70 (n = 5795) | ||
| Gender, no. (%) | < .001 | ||
| Female | 3953 (56.4) | 3053 (43.6) | |
| Male | 2848 (51.0) | 2742 (49.0) | |
| Race, no. (%) | < .001 | ||
| Black | 1736 (25.5) | 1101 (19.0) | |
| White | 5065 (74.5) | 4694 (81.0) | |
| Smoking status, no. (%) | < .001 | ||
| Never smoker | 2814 (41.4) | 2323 (40.1) | |
| Former smoker | 2436 (35.9) | 2408 (41.6) | |
| Current smoker | 1540 (22.7) | 1058 (18.3) | |
| Hypertension, no. (%) | < .001 | ||
| Yes | 1961 (28.9) | 2288 (39.7) | |
| No | 4819 (71.1) | 3482 (60.4) | |
| Asthma, no. (%) | .80 | ||
| Yes | 349 (5.2) | 289 (5.0) | |
| No | 6424 (94.7) | 5495 (94.9) | |
| Lung disease, no. (%) | < .001 | ||
| Yes | 250 (3.7) | 331 (5.7) | |
| No | 6522 (96.2) | 5445 (94.1) | |
| Early AMD, no. (%) | < .001 | ||
| Yes | 231 (3.5) | 356 (6.3) | |
| No | 6456 (96.6) | 5295 (93.7) | |
| FEV 1 -to-FVC ratio %, mean (SD) | 77.6 (4.4) | 76.4 (3.9) | < .001 |
a Based on the chi-square test (for categorical variables) and t test (for continuous variables).
The mean percentage predicted FEV 1 -to-FVC ratio for the entire cohort followed a bimodal distribution (black persons, left normal curve; white persons, right normal curve), with a distinct distribution cutoff at approximately 75.0% ( Figure ).
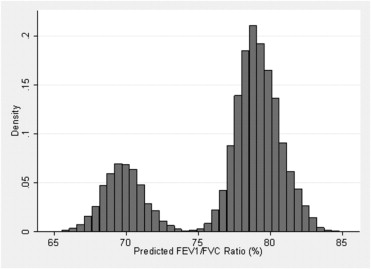
Table 2 shows an association between predicted FEV 1 -to-FVC ratio and early AMD in both models for the entire cohort ( P = .001 and .05, for likelihood ratio test). After adjusting for age and sex, there was a strong association between predicted FEV 1 -to-FVC ratio and early AMD (OR second quartile, 1.49; 95% CI, 1.14 to 1.94; P = .004; OR third quartile, 1.54; 95% CI, 1.18 to 2.00; P = .001). Attenuation of this association (OR second quartile, 1.61; 95% CI, 0.88 to 2.93; P = .12; OR third quartile, 1.65; 95% CI, 0.90 to 3.03; P = .10) is noted after further adjusting for race, study center, smoking, and hypertension, indicating confounding. Race is most likely the strongest confounder, whereby center could well represent a proxy for race. In addition, individual predicted lung function measures of FEV 1 , FVC, and peak expiratory flow rate were not significantly associated with early AMD. Similarly, there was no association between physician-diagnosed lung disease (OR, 1.08; 95% CI, 0.90 to 1.29) and physician-diagnosed asthma (OR, 1.06; 95% CI, 0.86 to 1.27) with early AMD for the entire cohort. There was no association between all measures of lung function and disease and early AMD among blacks and whites, respectively, after adjusting for confounders (data not shown).



