Fig. 54.1
Schematic horizontal section of the human eye
The optical system of the human eye comprises two optical elements: the cornea and the crystalline lens. The cornea is a quasi-transparent vault-shaped tissue at the front of the eye. It has no blood vessels and is composed of five main layers: epithelium, Bowman’s membrane, stroma, Decemet membrane, and endothelium. The cornea provides 85 % of the power refraction, as the larger index of refraction change occurs in the air-cornea interface. The normal cornea is best fit by a prolate conicoid (steeper at the center than along the periphery). The average radius of the anterior corneal surface curvature is 7.87mm and that of the posterior corneal surface is 6.40 ± 0.28 mm [3]. The average reported corneal conic constants are 0.82 and 0.62 for anterior and posterior surfaces, respectively [3]. The average corneal central thickness is 550 nm [4]. The refractive index changes across layers, with an effective index of refraction of 1.3771 at 598.3 nm [5].
The crystalline lens is a biconvex transparent element that increasingly opacifies with age; it is composed of multiple layers of long fiber cells that originate from the equator and stretch toward the poles of the lens, forming suture patterns at the point where they meet. The lens is covered by an elastic membrane, known as the lens capsule. The anterior and posterior lens surfaces are typically described as having an aspheric prolate shape, with average radii of curvature and conic constants, respectively, of 11.76 mm and −4 for the anterior surface, and 5.96 and −3 for the posterior surface [6]. The typical lens thickness is calculated (in mm) as 2.93 + 0.0236 × age (in years) [7] in the unaccommodated state. The young crystalline lens can change its shape to focus on near and far objects. The lens capsule is attached via the zonular fibers (mostly around the lens equator) to the ciliary body and ciliary muscle. When the ciliary muscle contracts, the apex of the ciliary body moves toward the lens equator to release tension on the zonular fibers, and the capsule molds the lens into an accommodated form. With accommodation, the lens surfaces become steeper and lens thickness increases. Another interesting optical feature of the crystalline lens is that the index of refraction is not constant but rather has a gradient distribution (both radially and axially) typically ranking from 1.36 in the nucleus to 1.44 at the surface [8]. The gradient refractive index (GRIN) results in a higher equivalent index (and therefore power) and typically in a more negative spherical aberration in the lens, which compensates for the positive spherical aberration of the cornea. The capability of the lens to shape upon an accommodative effort is lost with age (due to increased stiffness of the lens material). With age, the lens also undergoes shape changes due to its continuous growth throughout life and changes in the GRIN distribution.
In addition to the cornea and the lens, another important element in the anterior segment of the eye is the iris, a thin circular aperture responsible for controlling the diameter of the pupil, and therefore the amount of light entering the eye. Pupil diameter is controlled by ambient illumination, tends to contract upon accommodation of the crystalline lens, can be pharmaceutically controlled, and tends to decrease with aging.
Over the last two decades, there have been several developments in optical technology that have extended our ability to image and evaluate the anterior segment of the human eye. One of the most substantial developments in this field is the application of optical coherence tomography (OCT) to image and quantify morphologic structures of the human eye; this noncontact and noninvasive optical method is very well suited for biomedical applications [9–11]. OCT has found many applications in medicine and clinical practice, primarily because it offers noninvasive and noncontact imaging with relatively high sensitivity; this allows the detection of weakly diffusive, back-reflected light. In OCT applications, the measured thickness of the optically sectioned (coherence-gated) transverse layer is about an order of magnitude thinner than that achievable with scanning laser ophthalmoscopic (SLO) instruments. OCT also offers improved sensitivity due to additional filtering and amplification of the oscillatory interferometric signal. Optical coherence tomography has been most widely applied to retinal imaging [12–15]. This method was initially commercialized by Zeiss with three generations of retinal OCT devices (OCT1, OCT2, and Stratus OCT). Later, another time-domain OCT instrument was introduced to ophthalmology clinics – an en-face OCT/SLO device (OTI) that offers a unique combination of the two abovementioned imaging modalities [16–18]. At that time, it was rare to obtain in vivo three-dimensional images of the entire structure of the eye, primarily due to the physical and technical limitations of the TdOCT method that influenced measurements of time, sensitivity, and resolution.
Introduction of Fourier domain detection in OCT has opened new frontiers in OCT ophthalmic applications. Most importantly, the resultant substantial speed improvement enables rapid image acquisition, helping to reduce artifacts due to patient motion. Thus, it is currently possible to perform high-speed in vivo three-dimensional volumetric imaging over large scales within a reasonable time limit and without reducing system sensitivity [19–22]. Fourier domain OCT (FdOCT) had the additional advantage of making the system sensitivity independent of the axial resolution (i.e., the resolving power of the imaging system in the direction of the propagation of the probing light beam) [14, 21, 23–27]. There are currently more than seven commercially available FdOCT instruments dedicated for retinal imaging; the functionality of most of them can be extended to cornea imaging, but only in the limited range of 2–3 mm.
The application of OCT to the anterior segment imaging is particularly of interest, since this could potentially provide substantial complementary information regarding the large-scale architecture of the cornea and the crystalline lens, or on small portions of tissue imaged with high spatial resolutions comparable to regular microscopy. The latter could be used for ophthalmic diagnoses, including detailed monitoring of the Bowman’s membrane, corneal epithelium, stroma, capsule of the crystalline lens, intraocular lens surface, conjunctiva, or the corneoscleral junction. Meanwhile, large-scale imaging, covering a depth of 6 mm and 12 mm × 12 mm of the transverse range, can provide morphometric parameters, including the corneal thickness and topography, iridocorneal angle, and orientation of intraocular lens [28, 29]. Additionally, remarkable advances in the field of refractive surgery have created requirements for more accurate imaging and measurements of corneal curvature and topography [30]. Three commercially available instruments are exclusively dedicated to diagnoses of the anterior segment; each of them have an imaging light with a 1,300-nm central wavelength, which allows visualization of the whole anterior segment, from limbus to limbus and from the front corneal surface to the posterior surface of the crystalline lens [19]. This spectral bandwidth also ensures improved safety due to the high water absorption of 1,300-nm radiation compared to 800-nm light wavelengths. One of the commercial instruments is the Visante OCT (Carl Zeiss Meditec) and the second is the SlitLamp OCT (Heidelberg Engineering); both use TdOCT. These systems can only collect a couple of thousand A-scans per second; therefore, acquiring an image in a reasonable amount of time allows only a sparse sampling. Quantitative analysis of the cornea can be affected by motion artifacts and imperfections in patient adjustment (in asterisk scan patterns). Substantial improvement of the imaging speed would allow increased sampling density and reduce the influence of motion artifacts, which can be crucial for improved repeatability and accuracy of the corneal topography. The other commercially available OCT device for anterior segment imaging is the SS-1000 Casia (Tomey), the only commercial instrument that uses state-of-the-art technology with swept-source OCT. Unfortunately, this instrument does not exploit the full potential of swept-source OCT, because its imaging speed is 30,000 optical A-scans/s, similar to that of commercially available retinal SOCT devices.
54.2 Technical Advantages and Limitations of Anterior Segment FdOCT Instruments
Compared to retinal imaging, imaging the anterior segment of the human eye requires substantially different measurement conditions and instrumentation. The table in Fig. 54.2 presents the main parameters cited from literature [31–33] that are important for optical imaging of the anterior segment of the human eye; they determine the requirements and limitations in dynamic range, the sensitivity and penetration depth of the optical imaging instrument. Careful analysis of these numbers will assist in choosing the optimal wavelength and imaging speed of the device. The most substantial restriction of OCT is the limited penetration depth of the probing light beam in biological tissues. Additionally, the multiple scattering of detected backscattered light substantially reduces the quality of reconstructed images. Therefore, OCT imaging is limited to applications in ocular anatomical structures that weakly scatter light with only a small amount of melanin or hemoglobin. In retinal imaging, the light has to travel through about 2.5 cm of ocular media (mostly through transparent tissues containing water, which strongly absorbs infrared radiation); thus, retinal OCT can only use wavelengths in the optical window of 400–1,100 nm. This limitation does not apply to anterior eye imaging. Typically, light in the near-infrared range (λ = 0.8–1.3 μm) penetrates well through optically transparent parts of the anterior segment, like the cornea, vitreous, and crystalline lens. However, penetration of the sclera (Fig. 54.2) and iris is still substantially limited. Typically, near-infrared light (700–1,300 nm) penetrates the sclera to a depth of approximately 1 mm. The iris has also low transmittance and high scattering, but it is difficult to determine their absolute values due to high individual variability of the melanin concentration.
The most important challenge in anterior segment imaging is that data must be collected from a much larger volume than for retinal OCT. To obtain all information about the entire corneal architecture, including the corneoscleral junction and the corneal apex, a volume of approximately 15 mm × 15 mm transversally and 5 mm in depth must be scanned. Thus, if a relatively high scanning density is maintained, along with high axial resolution, a substantially greater amount of data will be captured with the acquisition system and stored in the hard drives. For example, three-dimensional reconstruction of the anterior segment with a voxel size of 20 μm × 20 μm × 3 μm and 10-bit analog-to-digital conversion requires collection of 4.5 GB of data. In practice, this information must also be acquired during a short enough time to minimize the negative impact of sample motion; this concern sets the fundamental speed requirements for the imaging devices to sample at the order of magnitude of gigasamples per second. Such requirements are highly demanding for the state-of-the-art technology, both regarding optical detection with the digitalization and transfer to PC. To meet the abovementioned specifications, an ideal OCT device should run with more than 500,000 A-scans/s to collect high-resolution volumetric data from the entire anterior segment within 1 s.
One feature that makes OCT attractive as a diagnostic tool is that it can perform imaging with resolutions comparable to that of histopathology. Longitudinal (axial) OCT resolution is determined by the central wavelength and spectral bandwidth of light. Another fundamental constraint is the limited lateral resolution, which is related to the finite numerical aperture (NA) of the optical system. This restriction has different effects on imaging, depending on whether OCT is used for imaging the fundus or the anterior segment of the eye. When imaging the retina, the natural optics of the eye limits the available NA and, for beams larger than 2–3 mm, introduces severe distortions of the wavefront, thus substantially degrading the lateral resolution of OCT devices. When imaging the anterior segment of the eye, the restricted optical performance obliges a trade-off between the lateral resolution and the measuring range [34]. Fourier domain OCT systems – those using parallel detection with a spectrometer (SOCT, SdOCT) or serial detection with swept source – have the broadest range of applications. Each type of FdOCT can be optimized for specific applications within the limits of the currently available detector technology and wideband light sources. It has been demonstrated that both types of high-speed FdOCT instruments can provide complementary information about the morphology and architecture of the anterior segment [34, 35].
54.2.1 Parallel Registration by FdOCT Using Spectrometer (SOCT, SdOCT)
Spectral OCT (SOCT) is especially well suited to imaging small portions of anterior segment tissue with high spatial resolutions, comparable to regular microscopy [36]. In fact small software and hardware modifications enable the conversion of a commercially available retinal system into an anterior segment imaging OCT instrument. However, in such case, the ergonomics of commercially available retinal OCT systems is not optimal. This configuration has already been optimized for ultrahigh-resolution retinal OCT imaging at 800 nm in laboratory setups or prototype instruments [19, 37, 38]. One of the examples of such ergonomic prototype device has been developed and introduced by Optopol Technology. Figure 54.3 shows examples of high-quality anterior segment imaging using SOCT Anterius instrument.
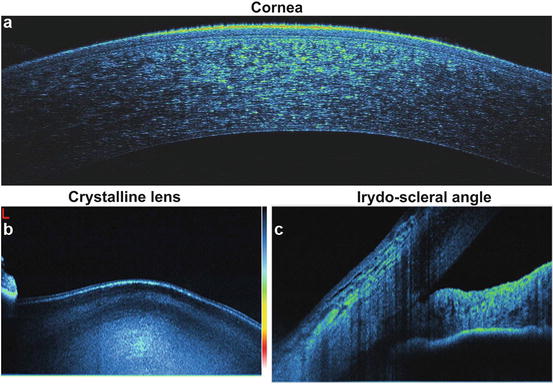
Fig. 54.3
High-quality cross-sectional imaging of the anterior segment of the human eye in vivo with 800-nm SOCT instrument (3 μm in tissue): (a) cornea, (b) corneoscleral angle, and (c) anterior part of the crystalline lens (Courtesy of Tomasz Bajraszewski, R&D Optopol Technology. Images obtained using the prototype SOCT Anterius instrument)
Despite limited imaging range of 800 nm high-resolution SOCT instruments, it has been demonstrated that this technology has a potential to become a powerful, noninvasive clinical corneal imaging modality that can enhance diagnosis and surgical treatments. Figure 54.4 shows examples of high-quality corneal imaging using laboratory SOCT instruments, which may be helpful in understanding clinical pathologic features related to the various corneal diseases including corneal scars and keratitis, bullous keratopathy, epithelial defects, granular corneal dystrophy, and Fuchs endothelial dystrophy [36, 39, 40].
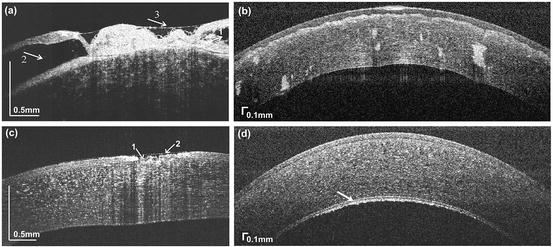
Fig. 54.4
High-quality corneal OCT imaging of pathologic cases. (a) End-stage bullous keratopathy; irregular thickness and reduplication of the epithelium, intraepithelial vesicles (1), bullae between the epithelium and Bowman layer (2), and tear film levels in the epithelial hollows (3). (b) granular corneal dystrophy with deposits in posterior anterior stroma. (c) corneal changes shortly after foreign body removal with epithelial defects (1) and tear fill levels in the hollows of the surface (2). (d) advanced Fuchs’ endothelial dystrophy; arrow indicates thickened Descemet’s membrane (Image reprinted from B. J. Kaluzny, et al. Cornea 25, 960–965, 2006 and Cornea 27, 830–832, 2008, copyright Lippincott Williams & Wilkins 2006 [36, 39])
High-resolution SOCT also improves visualization of structures and their relationship to incisional and refractive corneal procedures like penetrating keratoplasty, phacoemulsification, Descemet membrane stripping, endokeratoplasty, corneal implantation for keratoconus, and laser in situ keratomileusis [36, 41]. Figure 54.5 shows examples of high-resolution imaging of cornea after radial keratotomy and penetrating keratoplasty visualizing various postoperative corneal changes like scars, change of the corneal architecture, or the morphology of donor-host corneal junction [36].
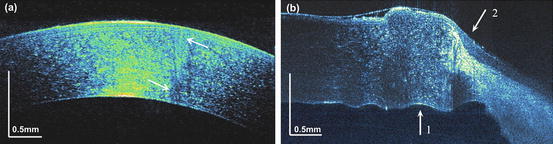
Fig. 54.5
OCT corneal imaging in incisional and refractive corneal procedures. (a) Scar after radial keratotomy 8 years after surgery; region of scar is indicated by arrows. (b) Eye surface 2 years after penetrating keratoplasty, (1) donor tissue and (2) host tissue (Image reprinted from B.J. Kaluzny et al., Cornea 25, 960–965, 2006, copyright Lippincott Williams & Wilkins 2006 [36])
In the regular clinical practice, SOCT images of corneal abnormalities may enhance slitlamp biomicroscopic examination, and they can be especially useful in the preoperative and postoperative clinical treatment of patients undergoing cataract surgery. Figure 54.6 shows examples of high-quality and high-resolution imaging of anterior segment showing changes in Descement membrane morphology, corneal incision, intraepithelial vesicles, and posterior capsule opacification – all effects are secondary to the cataract surgery.
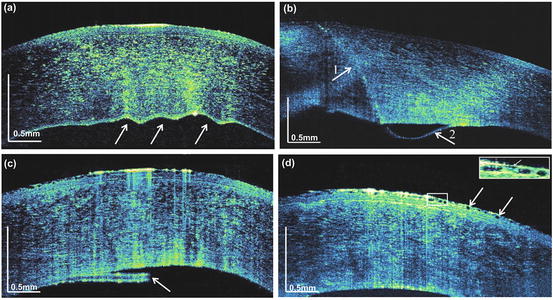
Fig. 54.6
OCT imaging of corneal changes after cataract surgery. (a) Folds of Descemet membrane (arrows), first day after surgery. (b) Corneal incision (arrow 1) and detachment of the thin posterior layer of the cornea (arrow 2), first day after surgery. (c) Partial removal of Descemet membrane (arrow), third day after surgery. (d) Intraepithelial vesicles caused by edema (arrows), third day after surgery; smallest resolved object (insert, arrow) is 25 mm wide and 5 mm deep (Image reprinted from B. J. Kaluzny et al., Cornea 25, 960–965, 2006, copyright Lippincott Williams & Wilkins 2006 [36])
Large-scale architecture of the cornea and the crystalline lens can be also imaged using SOCT [34]. However, the SOCT instrument is much less flexible and more demanding than swept-source OCT device. This is mainly because SOCT technique has fundamental and technological limitations in imaging range and sensitivity, especially when the imaged sample has substantial curvature. In such cases, the combination of depth-dependent sensitivity drop-off [19] and fringe washout [42] effects will have a radical negative impact on image quality. Additionally, SOCT setup has limited options for adjusting the axial resolution and measurement range; these parameters depend on the design of the spectrometer and spectral range of the light source. Using a CMOS camera in the spectrometer improves the system’s flexibility compared to CCD-based systems. In such a configuration, CMOS sensors usually enable programmable changes of the number of active pixels, which can improve the measurement speed. Unfortunately, reducing the number of active CMOS camera pixels without changing the configuration of the optical elements in the spectrometer results in truncation of the spectrum (Fig. 54.7). Consequently, the axial resolution and sensitivity decrease together with the reduction of pixel number. The last column in the right panel of Fig. 54.7 shows the effective sensitivity values, considering both the shortening of the signal integration time and the truncation of the spectrum.
Fig. 54.7
Spectrum of the light source used in the spectrometer-based FdOCT system. Areas of interest where the camera has captured 4,096, 2,048, and 1,024 pixels are indicated by red, blue, and green rectangles, respectively. The resolution decreases from 6.9 to 15.4 μm and the sensitivity drops by 4 dB if calculated for a given constant exposure time (T exp ) of 40 μs (Image reprinted with permission from OSA, I. Grulkowski, et al., Opt. Express 17, 4842–4858, 2009 [34])
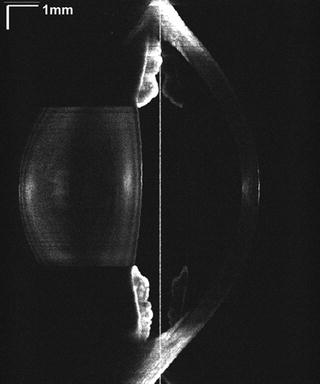
As presented in [34], even with all of these obstacles, it is possible to obtain high-quality cross-sectional OCT images of the entire cornea with an optimized OCT setup. In this case, high-speed imaging (118,000 A-scans/s) of the cornea and the crystalline lens simultaneously required very careful adjustment of the focal plane of the imaging lens and accurate positioning of the sample in respect to the zero optical path delay (OPD). This procedure helped to compensate the sensitivity roll-off of 20 dB over 5 mm. Figure 54.8 shows OCT images of the healthy eye of the same subject registered for different parameters, including sampling density, registration speed, and position in reference to zero OPD. According to the table in Fig. 54.7, the images were obtained with different sensitivities of 89 dB and 97 dB and axial resolutions 15 μm and 7 μm. Both systems had the same values of transverse resolution Δx (27 μm) and the confocal parameter ς (3.6 mm). Even with the relatively low axial resolution in Fig. 54.8 compared to that from Fig. 54.3, the architecture of the cornea, anterior surface of the lens, and irido-scleral angle are well reconstructed in Fig. 54.8b.
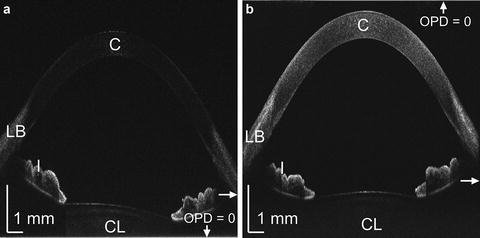
Fig. 54.8
2D OCT imaging of the cornea and anterior chamber using spectrometer-based Fourier detection: (a) single-line exposure time, 8.5 μs; repetition rate, ∼117,000 A-scans/s; 10,000 × 1,024 pixels; 15 mm and (b) single-line exposure time, 53 μs; repetition rate, ∼19,000 A-scans/s; 10,000 × 4,096 pixels; 15 mm. Structural elements are visible, including the cornea (C), limbus (LB), iris (I), and crystalline lens (CL). Position of zero optical path difference (OPD = 0) is indicated. Horizontal arrows show the position of the focal plane of the imaging lens (Image reprinted with permission from OSA, I. Grulkowski, et al., Opt. Express 17, 4842–4858, 2009 [34])
54.2.2 Serial Registration by FdOCT Using Swept-Source Technology (SS-OCT, OFDI)
As mentioned above, an ideal OCT anterior segment imaging system should combine two functionalities: providing high-quality and high-resolution cross-sectional images and having a programmable mode for measuring larger volumes. One of the most important technological advantages of the swept-source OCT setup is more flexibility and robustness in the opto-mechanical design, which can make swept source more advantageous in commercialization. Another important advantage of swept-source OCT device is the substantially lower sensitivity roll-off, which enables more optimal use of the entire measurement range. Moreover, some swept-source OCT devices are more flexible in the rapid adjustment of axial resolution and measurement range. Operating in different programmable regimes requires controlling the spectral span of light generated by the source; this can be done, for example, by flexible driving of the optical filter in the laser cavity. Unfortunately, not all designs of high-speed tunable light sources enable such control. The three major concepts behind achieving high-speed tuning differ in the method used for wavelength selection inside the laser cavity of the wavelength-swept source: one is based on a fast rotating polygonal mirror [43, 44], another based on a diffraction grating on a mechanically resonant galvo-scanner [45], and the third uses a Fabry-Perot tunable filter (FP-TF) [46, 47]. Only the third solution is able to switch between different modes by changing the amplitude of the FP-TF driving signal: the lower the amplitude of the driving signal, the narrower the wavelength scanning range. In principle, it is possible to choose any value for the axial resolution, limited only by the spectral bandwidth of SOA (highest resolution) or by the laser mode stability (lowest resolution). Gora et al. have demonstrated examples of bimodal operation of swept-source OCT [35]. The high speed of the swept-source OCT system enables high-definition imaging of large volumes, as well as high-accuracy reconstruction of certain portions of the anterior segment morphology, like the irido-scleral angle (Fig. 54.9).
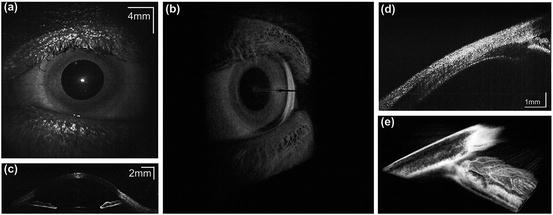
Fig. 54.9
Swept-source OCT imaging of the anterior segment of the human eye in vivo with single-line exposure time of 5 μs. (a) En-face view. (b) 3D rendering reconstructed from a 1,200 × 300 × 1,024 voxel dataset, with the size of the imaged volume 20 mm × 20 mm × 6 mm. (c) Representative cross-sectional image. (d) Cross-sectional image of the iridocorneal angle. (e) 3D rendering generated from the 3D data set (1,000 × 500 × 1,024 voxels) (Image reprinted with permission from OSA, M. Gora, et al., Opt Express 17, 14880–14894, 2009 [35])
The main limitation in the development of swept-source OCT technology is set by technological problems in developing swept sources for 800 nm and the visible range. Use of shorter optical wavelengths helps in optimization of the system performance in terms of image quality and the resolution. Also the speckle pattern can be reduced more effectively for shorter wavelengths. Finally in swept-source lasers, additional phase jitter can occur since the phase of registered interferometric signal is changed by mechanical filtering of optical frequency components in the laser cavity. One of the future challenges is in fast data processing and new algorithms for image processing, which can deliver more reliable and clinically significant information. Also high-speed systems provide huge amount of data which should be managed online.
54.2.3 Main Constrains of Anterior Segment FdOCT Method and Technology
One of the main objectives of high-quality and high-resolution in vivo anterior segment imaging is to achieve accuracy similar to that in microscopy. It is especially important for imaging of Bowman’s layer, the epithelial and endothelial tissue layers in the cornea, endothelium, and the capsule of the crystalline lens. However, a careful look at any magnified OCT cross-sectional image reveals that high spatial frequency intensity modulations are superimposed on the reconstructed structure; this modulation is called speckle noise, or a speckle pattern [48]. This “speckle noise” deteriorates OCT image quality and resolution and it occurs always when scattering samples are imaged.
Speckles result from random phases of backscattered light reflected from a rough surface or tissue with scattering structures that are smaller than the focused beam. This stochastic intensity distribution will depend on two factors: irregularities in the imaged tissue and diversity in the phase of detected light. The latter is based on the spectral bandwidth of the light and the NA of the collecting optical system. One important parameter that defines the speckle field is the speckle size. The average speckle spot size will increase with decreases in NA and spectral bandwidth. Thus, the NA of the collecting optics determines the angular range of scattered light that can be collected by the optical system: the greater the range, the smaller the average speckle size. Similarly, the NA of the device determines the lateral resolution of OCT; increasing NA leads to improved lateral resolution and reduced average speckle size. The electromagnetic field generates a different speckle pattern for each optical frequency component, resulting in additional modulation of the signal as a function of optical wavelength; moreover, after the Fourier transformation is applied, it also causes an intensity modulation in the axial direction. Therefore, two effects – transverse and axial – cause the speckle pattern in cross-sectional OCT images.
One of the main objectives of high-quality OCT imaging with micrometer resolution is to effectively reduce the contrast of speckles. Unfortunately, the presence of speckles is fundamentally related to the formation of the OCT image. In most cases, speckle noise reduction is achieved by averaging multiple images with variable, uncorrelated speckle patterns. Uncorrelated speckle patterns that originate from the same structure can be obtained by tracking speckles in space, over time, or by polarization diversity [49–51]. There are several ways to collect uncorrelated speckle patterns, such as compounding optical frequencies with two incoherent interferometer signals that use two light sources with different central wavelengths [52], applying light with orthogonal polarization states, using a partially spatially coherent light source [53, 54], angular compounding [55–59], inducing mechanical stress to the sample [60], or changing the position of the focusing objective [61]. The most common way of de-correlating the speckle pattern for in vivo imaging is the random spatial compounding method. In this method, a set of two- or three-dimensional images is acquired, with the expectation that the object’s natural instability (bulk motion) will cause a small dither in the scanning beam on the object and that this will induce strong variability in the speckle pattern [62–65]. This method has been combined with an eye tracker system in the Spectralis OCT instrument that was brought to the market by Heidelberg Engineering [66]. However, this technique is not fully controlled and can depend on the stability of patient fixation. An eye tracker is used to minimize randomness [67, 68], but the accuracy of this type of device is less than 50 μm [69].
Szkulmowski et al. recently published a study that applied speckle averaging in anterior segment imaging with the spatial compounding technique; this technique is insensitive to sample bulk motion and allows precise control of lateral resolution [70]. The authors used a scanning protocol with a resonant scanner that applied fast beam deflection in the direction perpendicular to the tomogram lateral dimension. This scanning protocol reduced the time interval between the A-scans to be averaged to the repetition interval of the acquisition system. As a result, the averaging algorithm did not require sophisticated data processing to align tomographic images, it is nearly immune to bulk motion in the investigated sample, and it allows precise control of lateral shifts in the scanning beam on the object. The authors also demonstrated a method for optimizing the dithering amplitude using the contrast-to-noise value. Figure 54.10 shows examples of high-resolution and high-quality FdOCT imaging with reduced speckle contrast. Corneal imaging shows a slight change of the imaging contrast within the epithelial layer, forming two layers of different reflectivity; the Bowman layer is also visible with reasonable contrast, which is less clearly distinguishable in images without reduced speckle contrast. The reconstruction of the stroma in the posterior section of the cornea reveals a more homogeneous layer close to the endothelium, possibly indicating the presence of Descemet’s membrane. It is also possible to distinguish the tear film, probably because the image was taken right after the eye blink, at the moment when the tear film was relatively thick. Speckle reduction also improves cross-sectional imaging of the crystalline lens, where the lens capsule and epithelium are clearly distinguishable. Furthermore, the internal structure of the lens is reconstructed, providing substantial new information about the refractive index distribution within the lens.
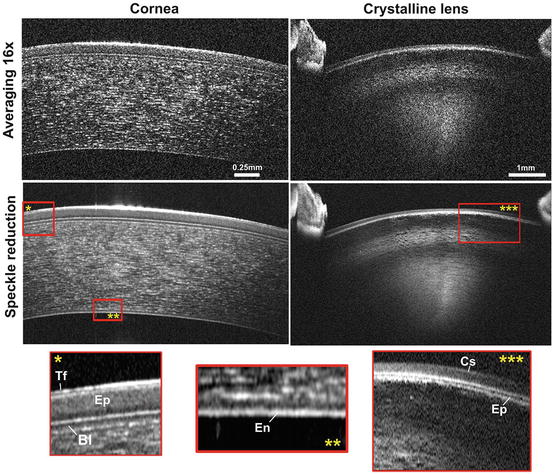
Fig. 54.10
Speckle reduction in OCT images. Axial resolution: 4.2 μm in tissue, imaging range 2.5 mm (cornea) and 7 mm (crystalline lens), imaging speed 200,000 lines/s. Speckle contrast was reduced by precise control of the orthogonal dither of the scanning beam set to 110 um (Image reprinted with permission from OSA, M. Szkulmowski, et al., Opt. Express 20, 1337–1359, 2012 [70])
This method can only be used for objects with specific morphological symmetry, due to the trade-off between reduced speckle contrast in two dimensions (cross-sectional image) and resolution in the third coordinate (perpendicular to the plane of the cross section). Several technological considerations also limit the construction of highly efficient, high-resolution spectrometers and interferometers. Ultimately, improved speckle reduction might require the introduction of novel techniques that remain to be discovered. However, there is a high probability that future state-of-the-art OCT technology will be free from speckle noise.
One of the main technological constraints of anterior segment FdOCT is limited axial imaging range. It is mostly caused by a combination of two fundamental technological limitations in Fourier detection scheme: sensitivity roll of due to the limited spectral resolution of the detection system (or instantaneous linewidth in swept source) [19] and additional presence of coherence noise and complex conjugate terms in the FdOCT signal [71]. As it was mentioned before, the sensitivity roll-off may be minimized by using swept-source OCT instruments [72]. However, the second effect is more fundamental and it cannot be solved by a development of better components or a careful design. For relatively thin objects like a retina, it is possible to design OCT instrument to set the total measurement range at least twice larger than the thickness of the measured sample. In such case, there is the possibility of separating the coherence noise components and complex conjugate images from the object’s structure reconstruction via a proper selection of the optical path difference between the reference mirror and the first surface of the examined object [12]. However, this procedure may often fail in the case of the anterior segment imaging where measured object has usually significant curvature. In this case, in order to avoid complex conjugate terms and extend the imaging range, it is necessary to introduce a substantial modification to FdOCT technique, which enables to reconstruct complex representation of measured signal and differentiate between complex conjugate signal components. This modified technique is called complex FdOCT [71]. Complex FdOCT technique requires the optical path difference (OPD) between the arms of the OCT interferometer to be varied (either a constant rate or discreet steps synchronized with the detection system) during the acquisition of the interferometric signal. Constant OPD change introduces a carrier frequency for every wavenumber along the time axis. Then an application of two-dimensional Fourier transformation will translate the wavenumber-time space to the depth-velocity space. As a consequence, both complex conjugate images are separated and shifted in opposite directions along v axis. Filtering procedure of negative values of v is equivalent to application of Hilbert Transformation, which in turn provides the complex representation of the real signal. An example of application of a technique of complex conjugate image removal based on the FdOCT using spectrometer has been demonstrated by Grulkowski et al. [45]. Authors demonstrated imaging of the entire anterior segment of the human eye including the cornea, anterior chamber angle, iris, and the entire crystalline lens (Fig. 54.11).