 itrectomy is mandatory when the vitreous presents in the anterior chamber during the course of cataract surgery. It is also done when a planned posterior capsulorrhexis is performed in pediatric patients. A manual vitrector does this job superbly, combining saline irrigation and vitrectomy simultaneously. Irrigation from the same port increases the amount of vitrectomy needed, so irrigation from a second port is preferred. The end point of vitrectomy is a matter of judgment. Most often the vitreous is cut much more than initially planned.
itrectomy is mandatory when the vitreous presents in the anterior chamber during the course of cataract surgery. It is also done when a planned posterior capsulorrhexis is performed in pediatric patients. A manual vitrector does this job superbly, combining saline irrigation and vitrectomy simultaneously. Irrigation from the same port increases the amount of vitrectomy needed, so irrigation from a second port is preferred. The end point of vitrectomy is a matter of judgment. Most often the vitreous is cut much more than initially planned.
My colleagues and I have used the Fugo blade to perform a small anterior vitrectomy with great ease, as illustrated in the following example.
CASE STUDY
Case: Congenital Fibrovascular Cataract
The 2-year-old had a congenital fibrovascular cataract. The central dense fibrovascular mass was invaded by many blood vessels from the ciliary body. The surgery was done as described below.
Surgical Technique
- Fix an iris claw intraocular lens in place.
- Keep the anterior chamber deep by injecting methylcellulose from the side port, and gently insert the Fugo blade under the intraocular lens. Ablate the periphery of the cataract along with invading blood vessels with plasma energy. In our case, during this process, a large hyaloid vessel was revealed. We cut this vessel too by carrying the ablating tip behind the fibrovascular mass into the vitreous (Fig. 35.1).
- When the fibrovascular mass is freed from all sides, pull it out through the incision. In our case, many vitreous strands were attached to the mass as it was brought out. We cut the strands with the Fugo blade outside the incision line.
- We saw vitreous strands coming out from under the upper edge of the intraocular lens and sticking to the iris and the incision line.
- To visualize the vitreous in the anterior chamber, the particulate form of steroid, dilute triamcinolone was used to irrigate the anterior chamber. Triamcinolone adheres to the vitreous and highlights it (Fig. 35.2).
- While keeping the anterior chamber deep with visco-elastic material, introduce the Fugo blade under the outlined vitreous, keeping the cutting tip parallel to the iris. Short, sweeping movements of the activated tip cut the vitreous strands instantly.
- Deal similarly with the fine strands on the iris; this produces no injury to the iris.
- Perform an iridectomy with a Fugo blade and close the incision line.
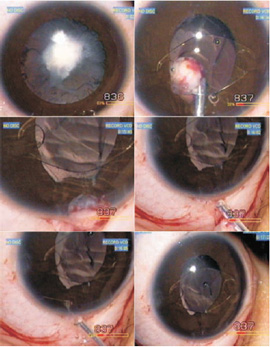
Figure 35.1. The central fibrovascular mass invaded by blood vessels from all sides is cut with a Fugo blade after fixing an iris claw lens. The hyaloid vessel is cut and the fibrovascular mass is removed. The vitreous strands attached to the mass are cut with the Fugo blade outside the incision line.
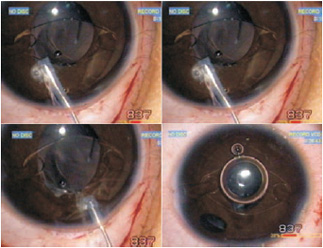
Figure 35.2. The vitreous strands in the anterior cham- ber are highlighted with triamcinolone and cut with the Fugo blade.
Summary
This case illustrates how even a bare-minimum anterior vitrectomy can be performed with the Fugo blade. The procedure requires no aspiration and therefore no traction. The only requirement is clear visualization of the aberrant vitreous, which can be accomplished with triamcinolone irrigation.
Adequate minimum anterior vitrectomy can also be done through the posterior capsulotomy, also without the need for aspiration and traction. Merely touching with and moving the activated Fugo blade tip removes the vitreous.
Suggested Reading
Singh K, Singh SK, Singh IR, et al. Applications of the Fugo blade. Trop Ophthalmol. 2007;7:28–36.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


