2 Anatomy of the Temporal Bone
The temporal bone actually consists of four fused parts—the squamous, tympanic, mastoid, and petrous bones.
 Squamous Bone
Squamous Bone
The squamous part of the bone represents the major part of the lateral surface of the bone. Above the level of the zygomatic process, the vertical portion of the squamous bone extends upward to cover part of the temporal lobe of the brain. The zygomatic process is actually part of the squamous portion of the bone. It originates anterior to the external auditory canal at the level of the junction of the vertical and horizontal parts of the squamous bone. The root of the zygomatic process shows an initial swelling known as the posterior zygomatic tubercle. Traced anteriorly, the root thins out to form the glenoid fossa for the articulation of the head of the mandible, and then thickens again to form the anterior zygomatic tubercle. The zygomatic process then thins out and flattens as it separates from the squamous bone and ends by articulation with the zygomatic bone. Posterior to the external auditory canal, the zygomatic process can be traced as a somewhat faint line, the supramastoid crest, indicating the level of the middle cranial fossa. The squamous bone then extends inferiorly in its retromeatal portion, forming the flattened lateral part of the mastoid process. The squamous part of the temporal bone also forms the superior parts of both the anterior and posterior walls of the bony external auditory canal. On the posterosuperior border of the canal, the spine of Henle can be seen. The squamous part of the temporal bone also forms the superior parts of both the anterior and posterior walls of the bony external auditory canal. On the posterosuperior border of the canal, the spine of Henle can be seen.
 Tympanic Bone
Tympanic Bone
The gutter-shaped tympanic bone forms the inferior wall and major parts of the anterior and posterior walls of the bony external auditory canal. Two sutures between the elementary structures that form the temporal bone appear in the canal. The tympanosquamous suture is located anterosuperiorly, and the tympanomastoid suture posteroinferiorly. Connective tissue enters into these suture lines, and sharp dissection may be required during meatal skin elevation. The temporomandibular joint is located just anterior to the canal and is separated from the canal only by a thin bony shell. The lateral border of the tympanic bone is roughened for the attachment of the cartilaginous part of the external auditory canal, which forms the outer two-thirds of the canal. The inferior edge of the tympanic bone expands to form the vaginal process where the styloid process lies.
 Mastoid Process
Mastoid Process
The mastoid process can be seen at the posterior and inferior border of the temporal bone, protruding anteroinferiorly to variable levels, depending on the pneumatization of the mastoid. The process serves as the anterior part of the attachment of the sternocleidomastoid muscle. On its medial surface lies the digastric groove, from which the posterior belly of the digastric muscle originates. On the posteromedial end of the groove, an impression of the occipital artery can be seen. The stylomastoid foramen, from which the main trunk of the facial nerve exits the temporal bone, can be seen at the anterior border of the digastric ridge posterior to the styloid process.
The temporal component of the jugular foramen can be seen anteromedial to the stylomastoid foramen and medial to both the tympanic bone and the styloid process. From the lateral border of the foramen, the jugular spine of the temporal bone can be seen extending into the foramen toward its occipital counterpart and separating the foramen into the what are known as the vascular and nervous compartments. Through the fossa and at a more superior level, the dome of the jugular bulb can be seen. Posteriorly lies the small canal for the passage of Arnold’s nerve (the auricular branch of the vagus nerve), while anteriorly the end of the groove of the in ferior petrosal sinus can be seen lateral and anterior to the opening of the cochlear aqueduct. The foramen of the internal carotid artery is separated from the anterior border of the jugular foramen by a thin wedge of bone called the jugulocarotid spine, through which a canal for the passage of Jacobson’s nerve (the tympanic nerve) to the tympanic cavity lies.
 Petrous Bone
Petrous Bone
The most prominent feature of the medial aspect of the temporal bone is the petrous part. Shaped like a pyramid, this part protrudes in an anteromedial direction, with the base located laterally and formed by the semicircular canals, vestibule, cochlea, and carotid artery. The apex of this bone forms part of the anterior foramen lacerum. Through the apex, the internal carotid artery exits the petrous bone to the anterior foramen lacerum, where it curves superiorly on its way to the cavernous sinus. The end of the bony part of the eustachian tube, the isthmus, is also located in the apex anterior to the carotid opening and just medial to the spine of the sphenoid. The superior surface of the petrous bone forms part of the middle cranial fossa. It begins from the arcuate eminence and ends at the foramen lacerum. The groove of the greater petrosal nerve can be seen coursing close to the bone near the anterior border of this surface; in 10% of cases, the nerve can be traced posteriorly into a dehiscent geniculate ganglion. The bisection of the angle formed by this groove and the arcuate eminence marks the position of the internal auditory canal. Near the foramen lacerum, the impression of Meckel’s cavity can be seen. The posterior border of this surface is marked by the groove for the superior petrosal sinus, which separates the superior and posterior surfaces.
The posterior surface of the petrous bone forms part of the posterior cranial fossa. The opening for endolymphatic duct and sac can be seen at the lateral end of this surface. This opening represents an important landmark for the posterior semicircular canal in procedures using the retrosigmoid approach. The most important feature of the posterior surface is the internal auditory meatus.
 The Middle Ear
The Middle Ear
The Tympanic Membrane
The conically shaped tympanic membrane is tilted anteroinferiorly. As a result of this, the anteroinferior bony wall is longer than the posterosuperior one, and the anterior tympanomeatal angle is more acute than the posterior. The anterior angle is often obstructed by a bony protrusion of the anterior wall. Adequate visualization of this angle is the key to successful tympanic membrane reconstruction. The tympanic membrane is composed of three layers. Laterally, it is covered with an epidermal layer, and medially with a mucosal layer. Between these two layers, there is a fibrous layer, the laminapropria. The tympanic membrane is divided into two parts. The pars tensa, located inferior to the lateral process of the malleus and the anterior and posterior malleal folds, represents the majority of the tympanic membrane. The lamina propria thickens in the periphery of the pars tensa to form the tympanic annulus. The tympanic annulus is attached to a groove on the bony canal, called the tympanic sulcus. The pars flaccida is located superior to the lateral process of the malleus and is delineated superiorly by a bony notch in the superior canal wall, called the Rivinus notch. Medial to the pars flaccida and lateral to the neck of the malleus is Prussak’s space, in which epitympanic cholesteatomas start to invaginate medially from the pars flaccida.
The Ossicular Chain
The malleus. The manubrium of the malleus is firmly attached to the tympanic membrane. Its tip corresponds to the umbo of the tympanic membrane, which is the bottom of its conical shape. The lateral process is located at the superolateral end of the manubrium. Due to its proximity to the superolateral canal wall, meticulous care should be taken not to touch this process with burrs during canalplasty. The head of the malleus is located in the attic, and its neck connects the head and the manubrium. The tendon of the tensor tympani muscle attaches to the medial surface of the neck. Contraction of the muscle pulls the ossicle medially, and the resulting tension on the tympanic membrane limits sound transmission to the inner ear to some extent. The head of the malleus is supported by the superior and anterior suspensory ligaments.
The incus. The anterior surface of the body of the incus forms an articulation with the head of the malleus. The short process of the incus projects posteriorly. The short process is lodged in the fossa incudis. The long process projects into the tympanic cavity, and forms an articulation with the stapes at its lenticular process. The incus is supported by the malleus anteriorly and the posterior incudal ligament posteriorly.
The stapes. The smallest bone in the human body, the stapes, is located in the oval window. The head of the stapes forms an articulation with the incus. The stapedius muscle inserts onto the head and the posterior crus. The footplate is accommodated in the oval window, which opens into the vestibule. The connective tissue lying between the footplate and the edge of the oval window is called the annular ligament. Contraction of the stapedius muscle tilts the stapes and its footplate, and the resulting tension on the annular ligament limits sound transmission into the inner ear to some extent.
The Tympanic Cavity
The mesotympanum is a portion located just medial to the tympanic membrane. Superior to the epitympanum (attic), it is bordered by the tympanic segment of the facial nerve. A recess inferior to the tympanic membrane is the hypotympanum. The protympanum, located anteriorly to the tympanic membrane, has the tympanic orifice of the eustachian tube, just inferior to the semicanal of the tensor tympani muscle. A branch of the facial nerve, the chorda tympani, courses lateral to the long process of the incus and medially to the manubrium of the malleus after emerging from the posterior wall. The nerve contains sensory fibers for taste and secretory fibers innervating the submandibular and sublingual glands.
Medial Wall
The facial nerve (see below).
The cochleariform process. The cochleariform process lodges the tendon of the tensor tympani. It is located just medial to the neck of the malleus, anterosuperior to the oval window, and just inferior to the tympanic segment of the facial nerve. At this bony process, the tendon of the tensor tympani muscle makes a right angle and courses laterally to attach to the neck of the malleus.
The promontory. The promontory is a prominent eminence located anteroinferior to the oval window and anterior to the round window. It corresponds to the basal turn of the cochlea. The axis of the cochlea is directed anteriorly and laterally.
The oval window. The stapes footplate is lodged in this window to transmit mechanical energy to the scala vestibuli of the cochlea. The window edge and the stapes footplate are connected by connective tissue known as the annular ligament. The tympanic segment of the facial nerve runs just superior to the window, and near its posterior edge, the nerve turns inferiorly toward the stylomastoid foramen.
The round window. The round window is located in the round window niche, inferior to the oval window. The round window is the other opening of the labyrinth to the middle ear. With this window, the cochlear fluid packed into the bony structure is vulnerable to mechanical vibration. The round window membrane lies in the roof of the round window niche, and lies mostly in the horizontal plane. It is therefore difficult to see the membrane directly without removing the superior overhang of the niche.
Posterior Wall
The posterior tympanum contains deep recesses. The facial nerve running in the middle divides them into the tympanic sinus medially and the facial recess laterally.
The facial recess. The facial recess is bordered by the bony annulus laterally and the facial canal medially. This is the portion to be drilled for posterior tympanotomy in canal wall-up tympanoplasty. The facial recess is also subdivided into two segments by a bony bridge called the chordal crest that connects with the pyramidal eminence and the emergence of the chorda tympani called the chordal eminence.
The tympanic sinus. The sinus is located medial to the facial nerve. The posterior extension of the tympanic sinus is variable, and it may extend far medially to the facial nerve. Since direct visualization of its base is impossible in the majority of cases, eradication of disease from this sinus requires considerable experience. The tympanic sinus is subdivided into two segments, located superiorly and inferiorly, by a bony bridge known as the ponticulus, which connects the pyramidal eminence and the promontory. The tympanic sinus is bordered inferiorly by another bony bridge lying between the posterior wall and the round window niche, called the subiculum.
The Attic
A bony spur known as the cog extends vertically from the tegmen to a point just anterior to the head of the malleus. With this structure, the attic is divided into a posterior division and an anterior division, known as the supratubal recess. Cholesteatoma often advances into the recess, and the recess often becomes a site of residual disease if it is not fully opened during surgery. Since the cog is located superior to the facial nerve, with its tip pointing to it, the structure serves as one of the landmarks for the nerve. The floor of the anterior attic recess contains the postgeniculate portion of the facial nerve. An opening of the antrum called the aditus ad antrum is located posterior to the attic.
The Antrum
The antrum connects the mastoid air cells with the attic. It is located just posterior to the epitympanum, inferior to the middle fossa plate, and lateral to the labyrinth. Since the antrum is very consistent and there are no important structures lateral to it, the antrum serves as one of the most important landmarks in the initial stage of mastoidectomy. The prominence of the lateral semicircular canal is one of the most important landmarks for the facial nerve.
The Labyrinth
Semicircular Canals
The prominence of the lateral semicircular canal in the medial wall of the antrum slopes at about 30°, running from anterosuperior to posteroinferior. The bony capsule of the labyrinth is compact and hard, and more resistant to bone erosion. However, due to its proximity to the antrum, the lateral semicircular canal is the most vulnerable labyrinth to pathologies that erode the medial wall of the antrum, such as cholesteatoma. At the anterior end of the lateral semicircular canal lies the ampulla, which accommodates sensory cells and opens to the utricles. The ampulla is located in the medial wall of the posterior attic.
The other two semicircular canals are sited nearly perpendicularly to the lateral semicircular canal. The posterior semicircular canal lies just posterior to the lateral semicircular canal, and the posterior edge of the lateral semicircular canal points almost to the center of the posterior semicircular canal. The posterior semicircular canal courses nearly in parallel with the posterior fossa dura. Its ampulla is located at its inferior end, just medial to the mastoid segment of the facial nerve. The superior end of the posterior semicircular canal joins the superior semicircular canal, forming the common crus.
The superior semicircular canal is located just beneath the middle cranial fossa plate. Its ampulla is at the anterior end, just superomedial to the ampulla of the lateral semicircular canal. It courses nearly perpendicular to the long axis of the pyramis, which places the canal deeper and farther from the antrum posteriorly. The canal is therefore not seen in the majority of cases, and the entire canal may be exposed in limited cases in which intensive removal of perilabyrinthine cells is required, such as petrous bone cholesteatoma. In rare cases, the canal is dehiscent and is directly in contact with the middle fossa dura.
The ampullae of the superior and lateral semicircular canals are located in the medial wall of the posterior attic. If it is necessary to drill deeply into the medial wall of the attic, great care should therefore be taken not to open these two ampullae. The labyrinth is less resistant to an insult to the ampulla than to the semicircular canals.
Vestibule
The vestibule is a hollow space within the petrous bone that contains the utricle and the saccule. This space lies anterior to the semicircular canals, medial to the oval window, lateral to the fundus of the internal auditory canal, and posterior to the cochlea. Its posterior surface receives the five openings of the semicircular canals. Anteriorly, the ductus reuniens connects the vestibule to the scala vestibuli of the cochlea.
Cochlea
The cochlea, a spirally curved tube that forms two and a half turns, lies in front of the vestibule. It has a wide base and a narrow apex. The basal turn of the cochlea projects into the middle ear, forming the promontory bulge. The coils of the cochlea curve around a central cone of bone known as the modiolus, which arises from the fundus of the internal auditory canal and carries within it the fibers of the cochlear nerve. From the modiolus, a shelf-like bony projection known as the bony spiral lamina extends halfway into the cavity of the cochlear turns. The membranous spiral lamina or basilar membrane connects the edge of the bony spiral lamina to the lateral surface of the cochlear turns, thus dividing the space into two compartments—the scala vestibule superiorly and the scala tympani inferiorly.
 Internal Auditory Canal
Internal Auditory Canal
The internal auditory canal is a canal almost 1 cm in length that runs in a lateral direction from the cerebellopontine angle through the petrous bone. The meatus of the internal auditory canal can be seen in the posterior surface of the petrous bone. Its posterior border is formed by an acute angle, while the anterior border is more flat. The dura of the posterior cranial fossa continues into the internal auditory canal, lining the whole length, and ends by merging with the contained nerves as they enter their corresponding foramina. The long axis of the canal lies in line with the long axis of the external auditory canal.
At the lateral end of the internal auditory canal lies the fundus. The horizontal crest divides this area into a smaller upper zone and a larger lower zone. The upper zone is further divided by the vertical bar (“Bill’s bar”) into an anterior foramen for the passage of the facial nerve and a posterior one for the passage of the superior vestibular nerve. The cochlear nerve passes to the cochlea through a central canal surrounded by multiple small foramina located anteriorly in the lower zone of the fundus. The inferior vestibular nerve passes from the posterior part of this zone. Posteroinferior to this nerve lies the canal for the singular nerve, which supplies the ampulla of the posterior semicircular canal. In addition to these nerve, the canal also contains the internal auditory artery and vein, and a loop of the anterior inferior cerebellar artery may also be present.
The Carotid Artery
The carotid artery enters the temporal bone through the carotid foramen. It ascends vertically and emerges in the medial wall of the hypotympanum at the area just beneath the cochlea. It then turns anteromedially nearly at a right angle toward the petrous apex, forming a horizontal segment just posteroinferior to the eustachian tube and anterior to the cochlea. In 2% of cases, a bony shell separating the carotid artery and the eustachian tube is absent. The distance between the cochlea and the carotid artery ranges from 1 mm to 5 mm.
The Sigmoid Sinus and Jugular Bulb
The sigmoid sinus is a space lying between the inner and outer layer of the dura. Starting at the end of the transverse sinus, the sigmoid sinus curves downward and forward, leaving a deep impression on the inner surface of the mastoid bone. At its upper end, the superior sigmoid sinus receives the superior petrosal sinus. Near its middle, the mastoid emissary vein connects the sigmoid sinus to the posterior auricular vein. The sigmoid sinus ends at the posterior margin of the jugular foramen, where it expands to form the jugular bulb. This structure is located in the posterior and largest compartment of the foramen jugulare, connecting the sigmoid sinus and the internal jugular vein. The jugular bulb is located medial to the mastoid segment of the facial nerve and inferior to the semicircular canals. The distance from the facial nerve and the labyrinth varies, and the bulb is variably positioned in the hypotympanum. In some cases, the bulb is dehiscent in the hypotympanum. It should be remembered that the ninth to eleventh cranial nerves (the glossopharyngeal, vagus and accessory nerves) pass the skull base with this venous system.
 The Intratemporal Facial Nerve
The Intratemporal Facial Nerve
This part of the facial nerve (FN) is encased within a bony canal and is divided into three segments that are separated from each other by two genua.
Labyrinthine Segment
The labyrinthine segment is the thinnest and shortest segment of the FN. Its base runs from medial to lateral, from the fundus to the geniculate ganglion (GG). The borders of the narrow canal containing this segment are formed by the cochlea anteriorly, the superior semicircular canal posteriorly, the vestibule inferiorly, and a thin plate of bone separating the nerve from the middle cranial fossa dura superiorly. The GG is a swelling that marks the first genu of the FN and contains the cell bodies of all the sensory fibers of the FN. The thin plate of bone separating the geniculate ganglion form the middle cranial fossa dura may be absent in 10–15% of cases, putting the FN at risk during middle cranial fossa surgery. The first branch of the FN, the greater superficial petrosal nerve, leaves the anterior surface of the geniculate ganglion.
Tympanic Segment
Curving posteriorly at an angle ranging between 60 and 90°, the FN continues as the tympanic segment. This segment lies on the medial wall of the tympanum and protrudes into the cavity covered by a thin shell of bone. The beginning of this segment is marked by the cog superiorly and by the cochleariform process inferiorly. As the nerve passes posteriorly, it can be seen slanting inferiorly to assume an inferior position under the protrusion of the lateral semicircular canal on the medial wall of the middle ear. Underneath the nerve at this level lie the bulge of the promontory and the oval window. The incidence of dehiscence of the fallopian canal covering this segment is high, and in some series has been reported to be up to 50%. When the nerve reaches the level of the oval window, it starts to curve inferiorly, forming the second genu, which lies within the curvature of the lateral semicircular canal. Just before the nerve reaches the genu, the ampullae of the superior and lateralsemicircular canal lie medial to the FN, separated from it by a thin plate of bone.
Mastoid Segment
Medial to the short process of the incus, the nerve assumes a descending course starting the mastoid segment of the nerve. The pyramid, a bony protrusion that houses the stapedius muscle, lies few millimeters inferior to the short process of the incus, in contact with the anterior surface of the nerve. At this level (the pyramidal turn), the FN protrudes posterolateral to the lateral semicircular canal, putting the nerve at risk of injury during mastoid surgery. The descending or mastoid segment of the FN can be traced from the second genu to the anterior edge of the digastric ridge, where the stylomastoid foramen lies, marking the end of the intratemporal part of the FN. The relationship of this segment to the tympanic annulus is important in external auditory canal surgery. The posteromedial relationship of the FN to the annulus is more constant near the posterosuperior quadrant of the annulus. When the posteroinferior quadrant is reached, however, there is a high probability that the nerve may cross anterolateral to the plane of the annulus, making it susceptible to injury there.
The ampulla of the posterior semicircular canal lies medial to the midportion of this segment, forming a useful landmark in translabyrinthine surgery. The lower part of this segment is centered on the lateral surface of the jugular bulb, the superior extension of which determines the space available for a subfacial tympanotomy between the FN, jugular bulb, and inferior semicircular canal. The first muscular branch is the nerve to the stapedius. This nerve emerges from the anterior surface of the FN at the level of the pyramidal process. After branching out from the FN, it passes in a small canal within the pyramid to reach the stapedius muscle, which originates from within the pyramid. The chorda tympani is the branch that carries the secretomotor fibers to the sublingual and submandibular glands and the taste fibers from the anterior two-thirds of the tongue and the soft palate. The point of origin of this branch from the FN may lie anywhere between the lateral semicircular canal and the stylomastoid foramen. An origin from the extratemporal part of the FN has also been reported. In such instances, the chorda tympani travels back to enter the stylomastoid foramen. After originating from the FN, the chorda travels for a short distance within the posterior wall of the tympanic cavity and enters the tympanic cavity, passing in an anterior direction medial to the neck of the malleus, to exit through the tympanosquamous fissure (the gasserian fissure) at the anterior border of the tympanic membrane.
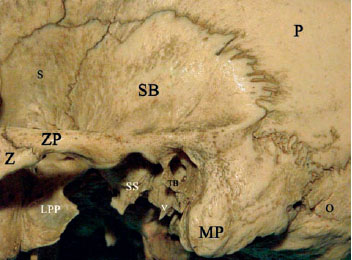
Fig. 2.1 Lateral view of the articulated temporal bone. P Parietal bone, LPP Lateral pterygoid process, MP mastoid process, O Occipital bone, S Greater wing of the sphenoid, SB Squamous bone, SS Spine of the sphenoid, V Vaginal process of the tympanic bone, Z Zygomatic bone, ZP Zygomatic process

Fig. 2.2 The lateral surface of a left temporal bone. AT Anterior zygomatic tubercle, F Glenoid fossa, H Spine of Henle, MP Mastoid process, PT Posterior zygomatic tubercle, S Vertical portion of the squamous bone, SP Styloid process, T Tympanic bone, V Vaginal process, ZP zygomatic process, * Roof of the external auditory canal (squamous bone),< Tympanosquamous suture line, > Tympanomastoid suture line
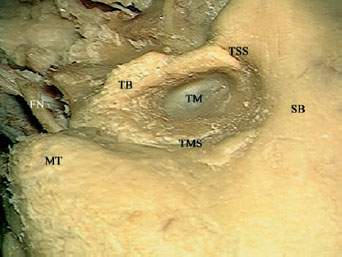
Fig. 2.3 A closer view of the external auditory canal and tympanic ring area. FN Facial nerve, MT Mastoid tip, SB Squamous bone, TB Tympanic bone, TM Tympanic membrane, TMS Tympanomastoid suture, TSS Tympanosquamous suture
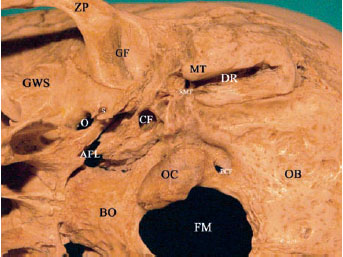
Fig. 2.4 An inferior view of an articulated temporal bone. AFL Anterior foramen lacerum, BO Basiocciput, CF Carotid foramen, DR Digastric ridge, FM Foramen magnum, GF Glenoid fossa, GWS Greater wing of the sphenoid, MT Mastoid tip, O Foramen ovale, OB Occipital bone, OC Occipital condyle, PCF Posterior condylar foramen, S Foramen spinosum,SMF Stylomastoid foramen, ZP Zygomatic process
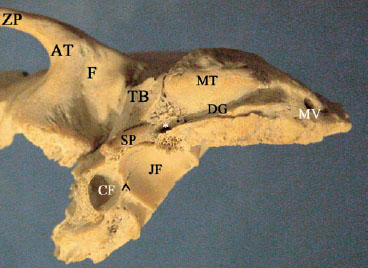
Fig. 2.5 An inferior view of a left temporal bone. * Stylomastoid foramen, ^ Jacobson’s nerve canal, AT Anterior zygomatic tubercle, CF Carotid foramen, DG Digastric ridge, F Glenoid fossa, JF jugular foramen, MT Mastoid tip, MV Mastoid emissary vein foramen, SP Styloid process, TB Tympanic bone, ZP Zygomatic process
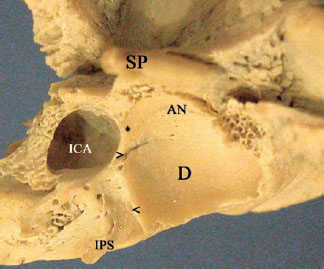
Fig. 2.6 A close-up view of the jugular foramen—carotid foramen area on the inferior aspect of a left temporal bone. * Jugulocarotid spine, < Cochlear aqueduct canal, > Jacobson’s nerve canal, AN Arnold’s nerve canal, D Dome of the jugular bulb, ICA Internal carotid artery canal, IPS Groove for the inferior petrosal sinus, SP Styloid process
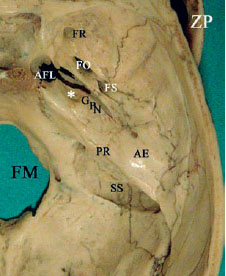
Fig. 2.7 A superior view of an articulated temporal bone. * Meckel’s cave impression, AE Arcuate eminence, AFL Anterior foramen lacerum, FM Foramen magnum, FO Foramen ovale, FR Foramen rotundum, FS Foramen spinosum, GPN Groove for the greater petrosal nerve, PR Petrous ridge, SS Sigmoid sinus sulcus, ZP Zygomatic process
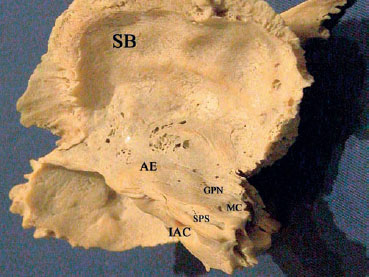
Fig. 2.8 A superior view of a left temporal bone. AE Arcuate eminence, GPN Groove for the greater petrosal nerve, IAC Internal auditory canal, MC Meckel’s cave impression, SB Squamous bone, SPS Superior petrosal sinus

Fig. 2.9 A view of the petrous apex component of the anterior foramen lacerum of a left temporal bone. * Canal of the tensor tympani muscle, ET Isthmus of the eustachian tube, ICA Internalcarotid artery canal
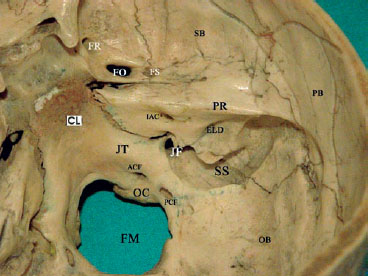
Fig. 2.10 A view of the posterior surface of an articulated temoral bone. ACF Anterior condylar foramen, CL Clivus, ELD Endolymphatic duct foramen, FM Foramen magnum, FO Foramen ovale, FR Foramen rotundum, FS Foramen spinosum, IAC Internal auditory canal, JF Jugular foramen, JT Jugular tubercle, OB Occipital bone, OC Occipital condyle, PB Parietal bone, PCF Posterior condylar foramen, PR Petrous ridge, SB Squamous bone, SS Sigmoid sinus groove
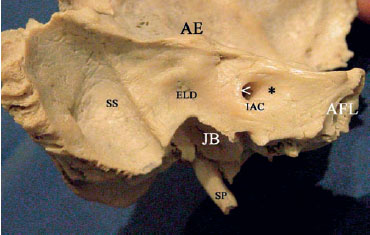
Fig. 2.11 A view of the posterior surface of a left temporal bone. * Anterior lip, < Posterior lip, AE Arcuate eminence, AFL Anterior foramen lacerum component of the petrous apex, ELD Endolymphatic duct foramen, IAC Internal auditory canal, JB Jugular bulb, SP Styloid process, SS Sigmoid sinus groove
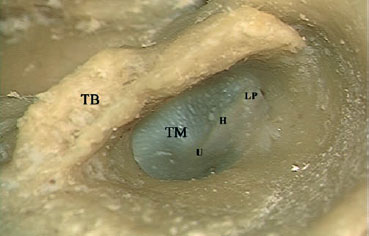
Fig. 2.12 A microscopic view of the left tympanic membrane. H Handle of the malleus, LP Lateral process of the malleus, TB Tympanic bone, TM Tympanic membrane, U Umbo
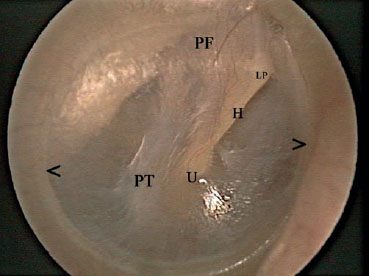
Fig. 2.13 A right normal tympanic membrane as seen by the endoscope. < > Annulus, H Handle of the malleus, LP Lateral process of the malleus, PF Pars flaccida, PT Pars tensa, U Umbo
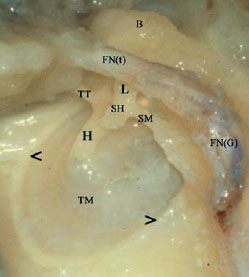
Fig. 2.14 A medial view of a right tympanic membrane. Note the membrane’s cone shape. < > Annulus, B Body of the incus, FN(G) Genu of the facial nerve, FN(t) Tympanic segment of the facial nerve, H Handle of the malleus, L Long process of the incus, SH Head of the stapes, SM Stapedius muscle, TM Tympanic membrane, TT Tensor tympani muscle
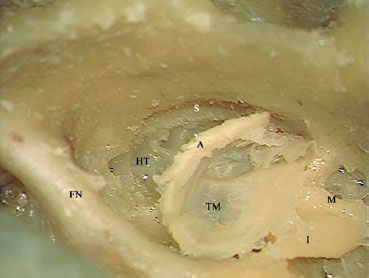
Fig. 2.15 In this left temporal bone, the annulus (A) has been detached from its sulcus (S) to show the relationship between the two. FN Mastoid segment of the facial nerve, HT Hypotympanum, I Incus, M Malleus, TM Tympanic membrane
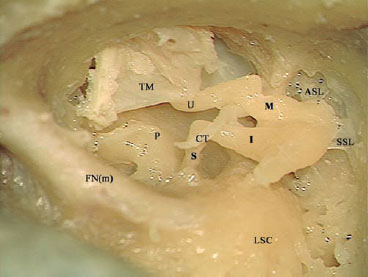
Fig. 2.16 A view of the articulated ossicular chain of the left ear. ASL anterior suspensory ligament, CT Chorda tympani, FN(m) Mastoid segment of the facial nerve, I Incus, LSC Lateral semicircular canal, M Malleus, P Pyramidal process, S Stapes, SSL Superior suspensory ligament, TM Tympanic membrane U Umbo
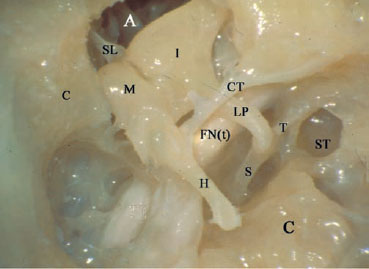
Fig. 2.17 Another view of the articulated ossicular chain. A Attic, C Cochlea, C Cog, CT Chorda tympani, FN(t) Tympanic segment of the facial nerve, H Handle of the malleus, I Incus, LP Long process of the incus, M Malleus, S Stapes, SL Superior suspensory ligament, ST Sinus tympani, T Tendon of the stapedius muscle
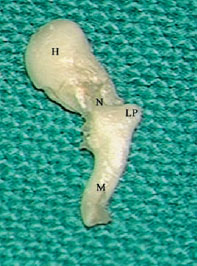
Fig. 2.18 A view of the lateral left malleus bone. H Head, LP Lateral process, M Manubrium or handle, N Neck
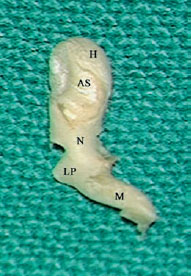
Fig. 2.19 A view of the medial surface of a left malleus bone. AS Articular surface, H Head, LP Lateral process, M Manubrium or handle, N Neck
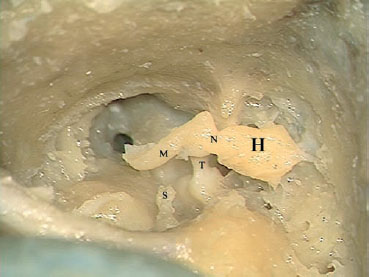
Fig. 2.20 A view of an articulated left malleus, showing the attachment of the tendon of the tensor tympani (T) to the medial aspect of the neck of the malleus (N). H Head of the malleus, M Manubrium or handle of the malleus, S Stapes head
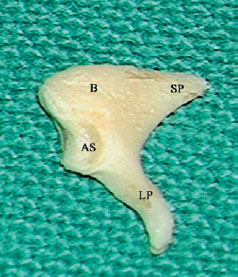
Fig. 2.21 A lateral view of a left incus bone. AS Articular surface, B Body, LP Long process, SP Short process
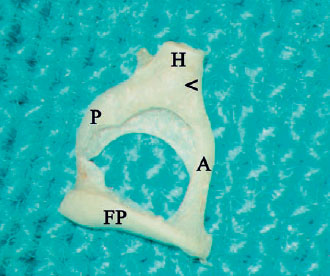
Fig. 2.22 A medial view of a left incus bone. ^ Lenticular process, AS Articular surface, B Body, LP Long process, SP Short process
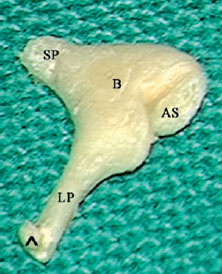
Fig. 2.23 A view of the stapes bone. ^ Tendon of the stapedius muscle, < Neck, A Anterior crus, FP Footplate, H Head, P Posterior crus
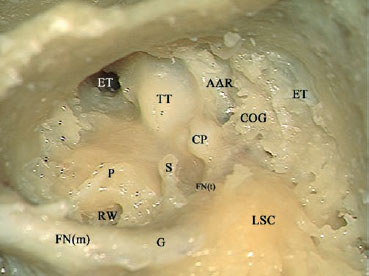
Fig. 2.24 A view of the tympanic cavity of a left ear after removal of the superior and posterior canal walls, the malleus and incus bones. AAR Anterior attic recess, COG Cog, CP Cochleariform process, ET (white) Epitympanum, ET (black) Eustachian tube, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, G 2nd genu of the facial nerve, LSC Lateral semicircular canal, P Promontory, RW Round window, S Head of the stapes, TT Tensor tympani muscle
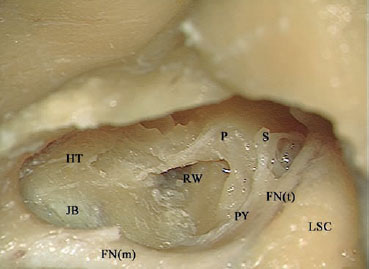
Fig. 2.25 In this left temporal bone, the anterior and posterior crura of the stapes (S) can be clearly seen. The air cells in the hypotympanic area (HT) have been partially drilled to show the relationship of the jugular bulb (JB) to the hypotympanum. FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, LSC Lateral semicircularcanal, P Promontory, PY Pyramidal process, RW Round window
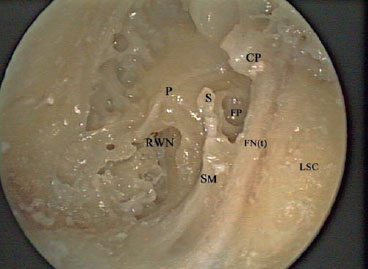
Fig. 2.26 An endoscopic view of a left middle ear. CP Cochleariform process, FN(t) Tympanic segment of the facial nerve, FP Footplate, LSC Lateral semicircular canal, P Promontory, RWN Round window niche, S Head of the stapes, SM Stapedius muscle running within the pyramidal process
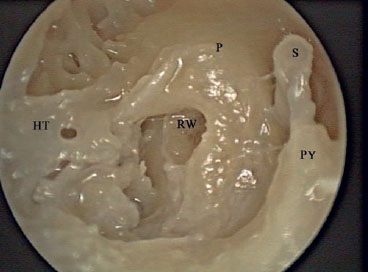
Fig. 2.27 An endoscopic view of the left middle ear, showing the mesotympanum and hypotympanum (HT). P Promontory, PY Pyramidal process, RW Round window, S Stapes
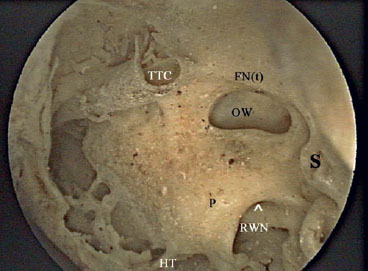
Fig. 2.28 An endoscopic view of a dried disarticulated left middle ear cleft. ^ The arrow shows the location of the round window, FN(t) Canal of the tympanic portion of the facial nerve, HT Hypotympanum, OW Oval window, P Promontory, RWN Round window niche, S Canal of the stapedius muscle within the pyramidal process, TTC Tensor tympani canal
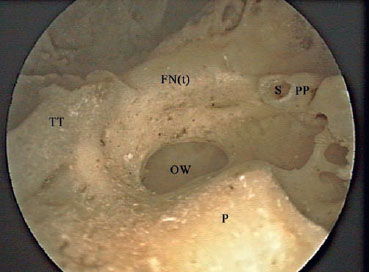
Fig. 2.29 An endoscopic view of a dried disarticulated left middle ear cleft. FN(t) Canal of the tympanic portion of the facial nerve, OW Oval window, P Promontory, PP Pyramidal process, S Canal of the stapedius muscle within the pyramidal process, TT Tensor tympani canal
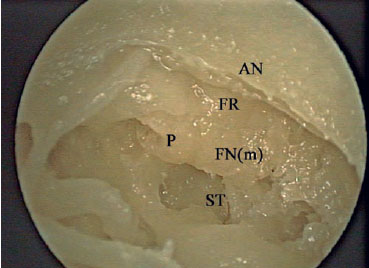
Fig. 2.30 An endoscopic view of the posterior wall of a left middle ear cleft. AN Annulus, FN(m) Mastoid segment of the facial nerve, FR Facial recess, P Pyramidal process, ST Sinus tympani
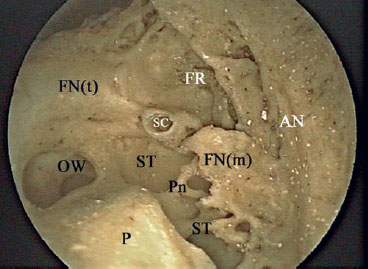
Fig. 2.31 An endoscopic view of the posterior wall of a dried disarticulated left middle ear cleft. AN Annulus, FN(m) Mastoid segment of the facial nerve, FN(t) Canal of the tympanic portion of the facial nerve, FR Facial recess, OW Oval window, P Promontory, Pn Ponticulus, SC Canal of the stapedius muscle within the pyramidal process, ST Sinus tympani

Fig. 2.32 Amicroscopic view of the sinus tympani (ST) area in a left ear. FN(t) Tympanic segment of the facial nerve, FP Footplate, P Pro montory, Pn Ponticulus, S Stapes
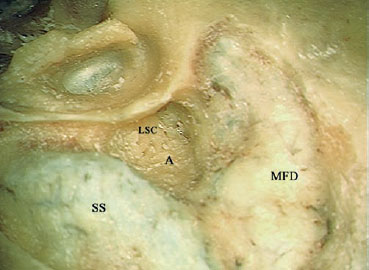
Fig. 2.33 A microscopic view of the antrum (A) of a left temporal bone. LSC Lateral semicircular canal, MFD Middle fossa dura, SS Sigmoid sinus
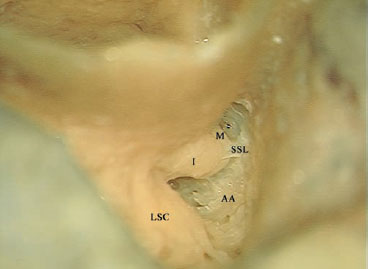
Fig. 2.34 A closer view, showing the aditus ad antrum (AA) in a left temporal bone. I Incus, LSC Lateral semicircular canal, M Malleus, SSL Superior suspensory ligament
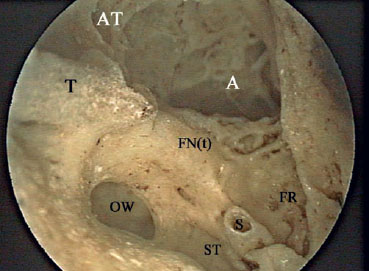
Fig. 2.35 An endoscopic view of the aditus ad antrum (A) in a dried dis articulated left temporal bone, as seen from the middle ear. AT Attic, FN(t) Canal of the tympanic portion of the facial nerve, FR Facial recess, OW Oval window, S Canal of the stapedius muscle within the pyramidal process, ST Sinus tympani, T Canal of the tensor tympani muscle
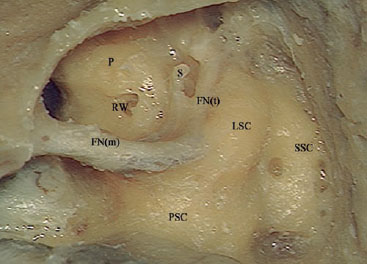
Fig. 2.36 In this left temporal bone, the superior semicircular canal (SSC), lateral semicircular canal (LSC), posterior semicircular canal (PSC), and cochlea have been identified to show their anatomy. FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, P Promontory, RW Round window, S Stapes
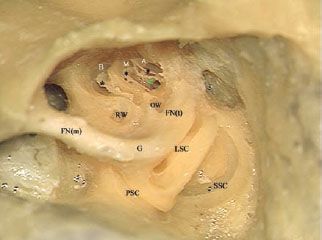
Fig. 2.37 The labyrinth has been opened. * Basilar membrane, < Modiolus, A Apical turn of the cochlea, B Basal turn of the cochlea, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segmentof the facial nerve, G Genu, LSC Lateral semicircular canal, M Middle turn of the cochlea, OW Oval window, PSC, Posterior semicircular canal, RW Round window, SSC Superior semicircularcanal, RW Round window, SSC Superior semicircular canal
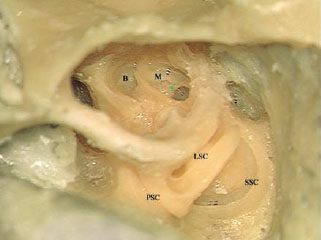
Fig. 2.38 The view after removal of the basilar membrane. < Modiolus, B Basal turn of the cochlea, LSC Lateral semicircular canal, M Middle turn of the cochlea, PSC Posterior semicircular canal, SSC Superior semicircular canal
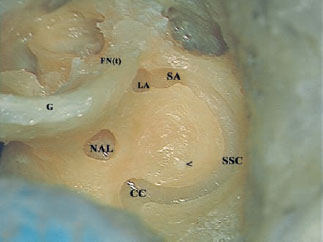
Fig. 2.39 In this view, the lateral and posterior semicircular canal have been drilled out. The intimate relationship between the ampullae of the lateral (LA) andsuperior (SA) canals and the tympanic segment of the facial nerve (FNt) can be appreciated. < Superior arcuate artery, CC Common crus, G Genu, NAL Nonampullated end of the lateral canal, SSC Superior semicircular canal
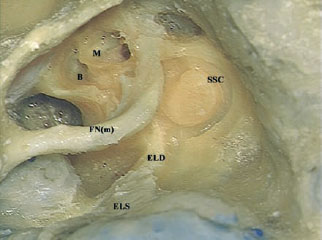
Fig. 2.40 The endolymphatic duct (ELD) of a left temporal bone can be seen passing from behind the posterior semicircular canal to the posterior fossa dura. B Basal turn of the cochlea, ELS Endolymphatic sac, FN(m) Mastoid segment of the facial nerve, M Middle turn of the cochlea, SSC Semicircular canal
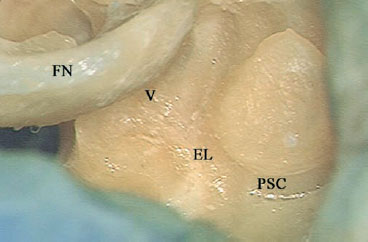
Fig. 2.41 The lower part of the posterior semicircular canal (PSC) has been drilled away here, and the endolymphatic duct (EL) can be followed proximally to the vestibule (V). FN Facial nerve
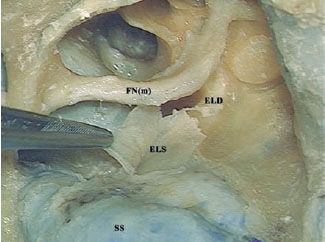
Fig. 2.42 The endolymphatic sac (ELS) has been opened. The intimate relationship between the sac and the posterior fossa dura can be appreciated. ELD Endolymphatic duct, FN(m) Mastoid segment of the facial nerve, SS Sigmoid sinus
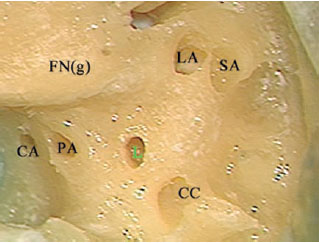
Fig. 2.43 The semicircular canals of a left temporal bone have been drilled out, and the five openings into the vestibule can be seen. CA Cochlear aqueduct, CC Common crus, FN(g) Facial nerve genu, L Nonampullated end of the lateral semicircular canal, LA Ampulla of the lateral semicircular canal, PA Ampulla of the posterior canal, SA Ampulla of the superior semicircular canal
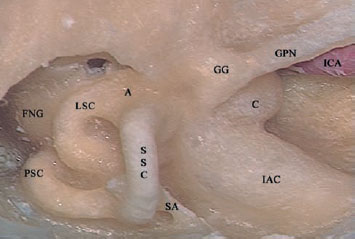
Fig. 2.44 A view of the inner ear components as seen from the middle cranial fossa of a left temporal bone. A Ampulla of the lateral semicircular canal, C Cochlea, FNG Facial nerve genu, GG Geniculate ganglion, GPN Greater petrosal nerve, IAC Internal auditory canal, ICA Internal carotid artery, LSC Lateral semicircular canal, PSC Posterior semicircular canal, SA Superior arcuate artery, SSC Superior semicircular canal
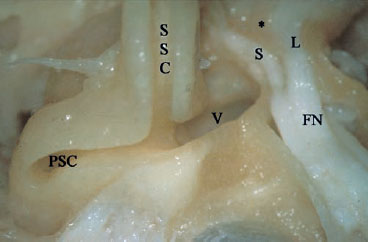
Fig. 2.45 A view from the middle cranial fossa of a left temporal bone, showing the superior semicircular canal (SSC) and posterior semicircular canal (PSC) as they join together, forming the common crus, to enter the vestibule (V). * Bill’s bar, FN Internal auditory canal segment of the facial nerve, L Labyrinthine segment of the facial nerve, S Superior vestibular nerve
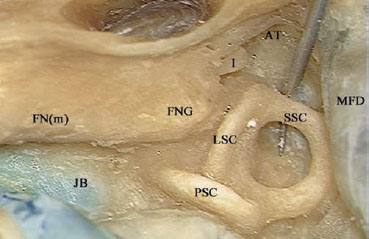
Fig. 2.46 A view of the labyrinth as seen from the mastoid cavity of a left temporal bone. The tip of the instrument is pointing to the superior arcuate artery. AT Attic, FN(m) Mastoid segment of the facial nerve, FNG Facial nerve genu, I Incus, JB Jugular bulb, LSC Lateral semicircular canal, MFD Middle fossa dura, PSC Posterior semicircular canal, SSC Superior semicircular canal
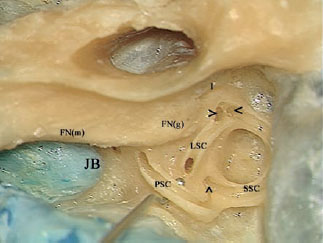
Fig. 2.47 The semicircular canals have been opened. Note the joint lateral (>) and superior (<) ampullae, and the union of the nonampullated ends of the superior and posterior semicircular canals into the common crus (^). The tip of the instrument is pointing to the nonampullated end of the lateral semicircular canal. FN(m) Mastoid segment of the facial nerve, FN(g) Facial nerve genu, I Incus, JB Jugular bulb, LSC Lateral semicircular canal, PSC Posterior semicircular canal, SSC Superior semicircular canal

Fig. 2.48 Via a retrosigmoid approach, the posterior (PSC) and superior (SSC) semicircular canals of a left temporal bone have been opened and followed to the common crus (CC) as it enters the vestibule (V).Note the endolymphatic duct (EL) passing posterior to the posterior canal and the common crus, serving as a landmark to their location in the retrosigmoid approach. Note also the high jugular bulb (JB) in this case. CA Cohlear aqueduct, F Facial nerve
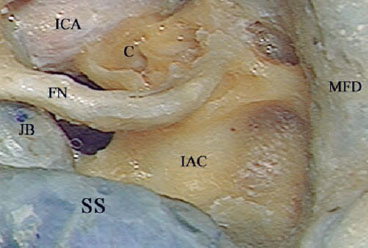
Fig. 2.49 Skeletonization of the internal auditory canal (IAC) of a left temporal bone has been started. The color of the canals’ dura can be seen through the bone. C Cochlea, FN Facial nerve, ICA Internal carotid artery, JB Jugular bulb, MFD Middle fossa dura, SS Sigmoid sinus
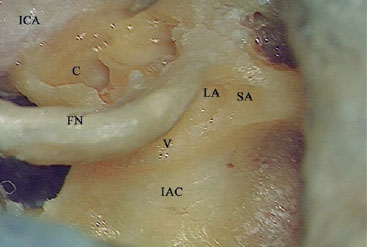
Fig. 2.50 A closer view, showing the relationship between the ampulla of the superior canal (SA) and the upper surface of the internal auditory (IAC). The superior canal ampulla serves as a landmark to the level of the upper surface of the internal auditory canal. C Cochlea, FN Facial nerve, ICA Internal carotid artery, LA Lateral canal ampulla, V Vestibule
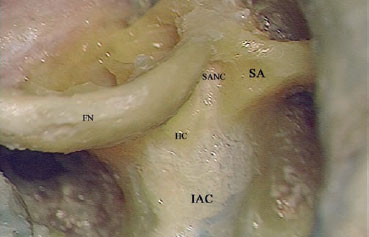
Fig. 2.51 The bone overlying the internal auditory canal (IAC) has been completely removed, and the superior ampullary nerve canal (SANC) has been followed into the ampulla of the lateral semicircular canal. FN Facial nerve, HC Horizontal crest, SA Ampulla of the superior canal
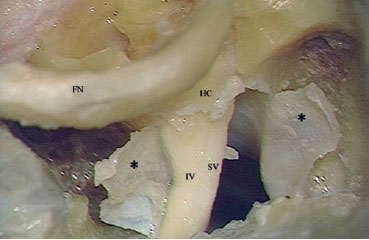
Fig. 2.52 The dura of the internal auditory canal (*) has been opened. The superior vestibular (SV) and inferior vestibular (IV) nerves can be seen lying posteriorly in the canal, separated by the horizontal crest (HC). FN Facial nerve
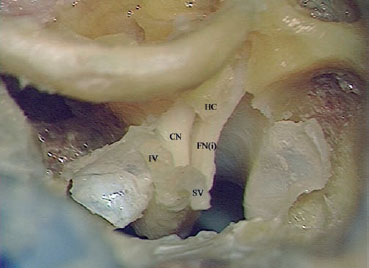
Fig. 2.53 The superior vestibular (SV) and inferior vestibular (IV) nerves have been dislocated from their entrances into the fundi and reflected posteriorly. The cochlear nerve (CN) and the internal auditory canal segment of the facial nerve (FNi) can be seen lying anteriorly, separated by the horizontal crest (HC).
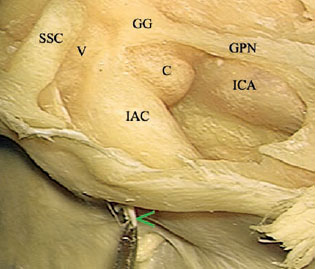
Fig. 2.54 From a middle cranial fossa view of a left temporal bone, the internal auditory canal (IAC) has been skeletonized. The relationship of the canal to the cochlea (C) and vestibule (V) can be seen. The canal can also be seen lying in the orientation of the bisection of the angle between the superior semicircular canal (SSC) and the greater petrosal nerve (GPN). < Acousticofacial bundle, GG Geniculate ganglion, ICAL internal carotid artery
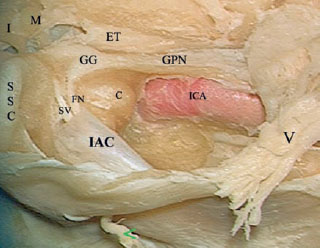
Fig. 2.55 The bone overlying the internal auditory canal has been removed and the dura of the canal has been removed near the fundus. The facial nerve (FN) can be seen entering its labyrinthine segment to form the geniculate ganglion (GG) more laterally. V Trigeminal nerve, < Acousticofacial bundle, C Cochlea, ET Eustachian tube, GPN Greater petrosal nerve, I Incus, IAC Internal auditory canal, ICA Internal carotid artery, M Malleus, SSC Superior semicircular canal, SV Superior vestibular nerve
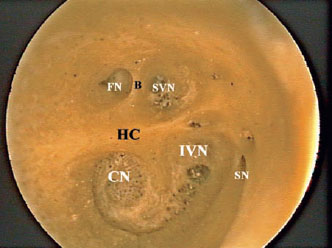
Fig. 2.56 An endoscopic view of the fundus of a right internal auditory canal. The opening of the fallopian canal for the passage of the facial nerve (FN) can be seen lying anterior to Bill’s bar (B). CN Cochlear nerve, HC Horizontal crest, IVN Inferior vestibular nerve, SN Singular nerve, SVN Superior vestibular nerve
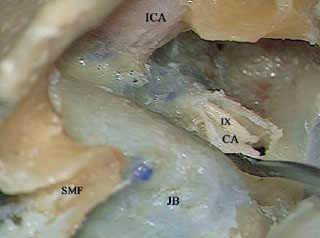
Fig. 2.57 After rerouting the facial nerve and drilling away the fallopian canal of a left temporal bone, the cochlear aqueduct (CA) has been opened. The proximity of the glossopharyngeal nerve (IX) can be well appreciated. Since the nerve lies just inferior to the cochlear aqueduct, the latter is used as a landmark to the nerve in the translabyrinthine approach, indicating the lower limit of drilling in order to avoid injury to the glossopharyngeal nerve. ICA Internal carotid artery, JB Jugular bulb, SMF Stylomastoid foramen
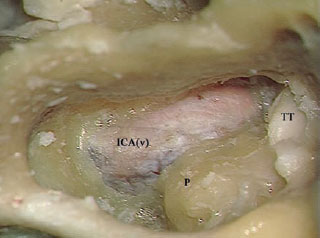
Fig. 2.58 In a left temporal bone, the hypotympanic air cells have been drilled out and the vertical segment of the internal carotid artery (ICAv) skeletonized. P Promontory, TT Tensor tympani
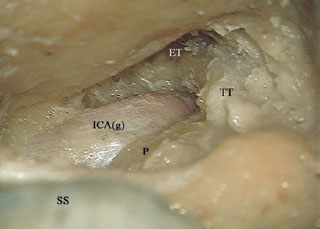
Fig. 2.59 The relationship between the genu of the internal carotid artery (ICAg), the promontory (P), and the eustachian tube (ET) can be appreciated. TT Tensor tympani muscle, SS Sigmoid sinus
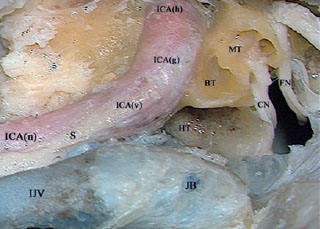
Fig. 2.60 The full length of the intratemporal internal carotid artery has been skeletonized. BT Basal turn of the cochlea, CN Cochlear nerve, FN Facial nerve, HT Hypotympanum, ICA(g) Genu of the internal carotid artery, ICA(h) Horizontal segment of the intratemporal internal carotid artery, ICA(n) Internal carotid artery in the neck, ICA(v) Vertical segment of the intratemporal internal carotid artery, IJV Internal jugular vein, JB Jugular bulb, MT Middle turn of the cochlea, S Sympathetic chain
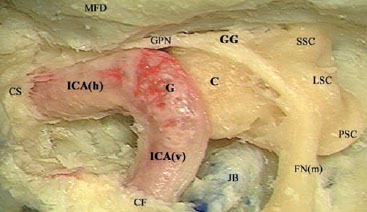
Fig. 2.61 All the bone surrounding the intratemporal internal carotidartery of a left temporal bone has been drilled out.C Cochlea, CF Carotid foramen, CS Cavernous sinus, FN(m) Mastoid segment of the facial nerve, G Genu, GG Geniculate ganglion, GPN Greater petrosal nerve, ICA(h) Horizontal segment of the internal carotid, ICA(v) Vertical segment of the internal carotid, JB Jugular bulb, LSC Lateral semicircular canal, MFD Middle fossa dura, PSC Posterior semicircular canal, SSC Superior semicircular canal
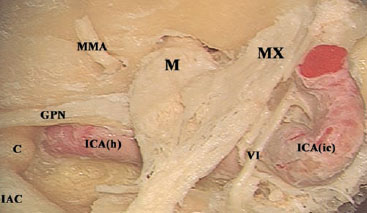
Fig. 2.62 The course of the horizontal segment of the internal carotidartery (ICAh), as seen from the middle cranial fossa of a left temporalbone. VI Abducent nerve, C Cochlea, GPN Greater petrosal nerve, IAC Internal auditory canal, ICA(ic) Intracranial internal carotid, M Mandibular nerve, MMA Middle meningeal artery, MX Maxillary nerve
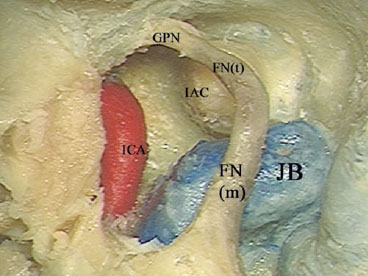
Fig. 2.63 Another case of a left transotic approach, with the bone in a vertical orientation. Note that the jugular bulb (JB) is very high in this case, and is almost lying in contact with the internal auditory canal (IAC). FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, GPN Greater petrosal nerve, ICA Internal carotid artery
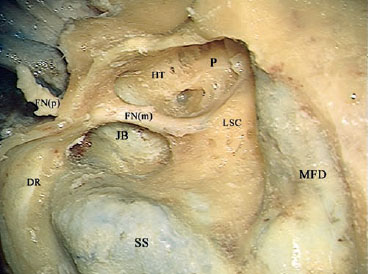
Fig. 2.64 In this left temporal bone, the sigmoid sinus (SS) has been skeletonized and followed to the jugular bulb (JB), which lies medial to the mastoid segment of the facial nerve (FNm). DR Digastric ridge, FN(p) Intraparotid portion of the facial nerve, HT Hypotympanum, LSC Lateral semicircular canal, MFD Middle fossa dura, P Promontory
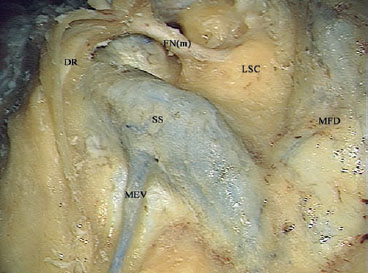
Fig. 2.65 The mastoid emissary vein (MEV) can be seen branching from the sigmoid sinus (SS). DR Digastric ridge, FN(m) Mastoid segment of the facial nerve, LSC Lateral semicircular canal, MFD Middle fossa dura

Fig. 2.66 The bone overlying the transitional zone from the jugular bulb (JB) to the internal jugular vein (IJV) has been drilled away. The hook can be seen underneath the fibrous band covering the exit of the bulb from the bone. The jugulocarotid spine of bone (<) can be seen lying between the internal carotid artery (ICA) and the jugular bulb. * The fibrous band covering the entrance of the internal carotid artery into the temporal bone.
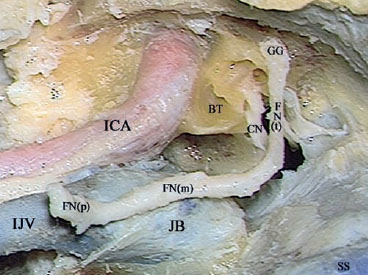
Fig. 2.67 The relationship of the mastoid segment of the facial nerve (FNm) to the jugular bulb (JB) after the removal of all the surrounding bone. BT Basal turn of the cochlea, CN Cochlear nerve, FN(p) Intraparotid segment of the facial nerve, FN(t) Tympanic segment of the fa cial nerve, GG Geniculate ganglion, ICA Internal carotid artery, IJV Internal jugular vein, SS Sigmoid sinus
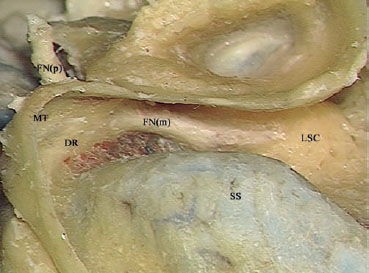
Fig. 2.68 In a left temporal bone, the digastric ridge (DR) has been identified. At its anterior end, the mastoid segment of the facial nerve (FNm) can be seen. FN(p) Intraparotid portion of the facial nerve, LSC Lateral semicircular canal, MT Mastoid tip, SS Sigmoid sinus
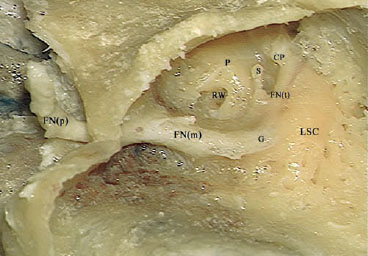
Fig. 2.69 The tympanic segment of the facial nerve (FNt) and its land marks can be seen. The cochleariform process can be seen lying at the anteroinferior end; the stapes can be seen inferiorly, and the lateral semicircular canal superiorly. CP Cochleariform process, FN(m) Mastoid segment of the facial nerve, FN(p) Intraparotid portion of the facial nerve, G Genu, LSC Lateral semicircular canal, P Promontory, S Stapes, RW Round window
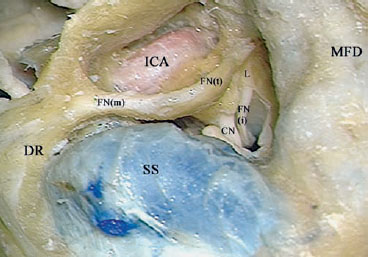
Fig. 2.70 The full length of the intratemporal facial nerve can be seen. CN Cochlear nerve, DR Digastric ridge, FN(i) Internal auditory canal segment of the facial nerve, FN(m) Mastoid segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, ICA Internal carotid artery, L Labyrinthine segment of the facial nerve, MFD Middle fossa dura, SS Sigmoid sinus
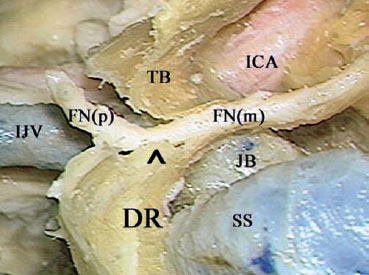
Fig. 2.71 This figure shows the exit of the facial nerve from the stylomastoid foramen (^) of a left temporal bone.DR Digastric ridge,FN(m) Mastoid segment of the facial nerve, FN(p) Intraparotid facial nerve, ICA Internal carotid artery, IJV Internal jugular vein, JB Jugular bulb, SS Sigmoid sinus, TB Tympanic bone
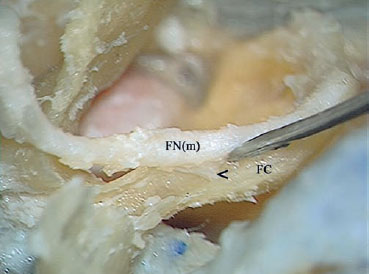
Fig. 2.72 The fibrovascular attachments (<) of the mastoid segment of the facial nerve (FNm) to the fallopian canal (FC) can be appreciated.
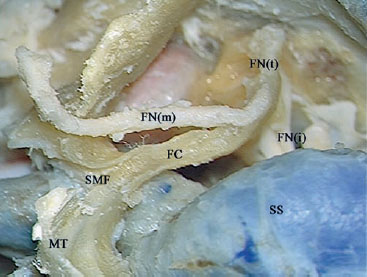
Fig. 2.73 The fibrovascular attachment has been sharply cut, and the mastoid segment of the facial nerve (FNm) has been freed from the fallopian canal (FC). FN(i) Internal auditory canal segment of the facial nerve, FN(t) Tympanic segment of the facial nerve, MT Mastoid tip, SMF Stylomastoid foramen, SS Sigmoid sinus
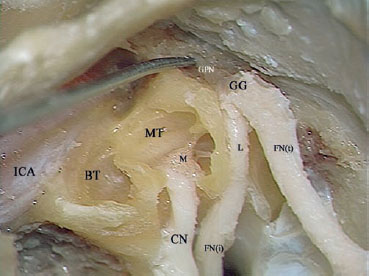
Fig. 2.74 The cochlear nerve (CN) can be seen here passing from the in ternal auditory canal to the modiolus (M), and the relationship between this part of the cochlear nerve and the internal auditory canal (FNi) and labyrinthine (L) segments of the facial nerve can be appreciated. BT Basal turn of the cochlea, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, GPN Greater petrosal nerve, ICA Internal carotid artery, MT Middle turn of the cochlea
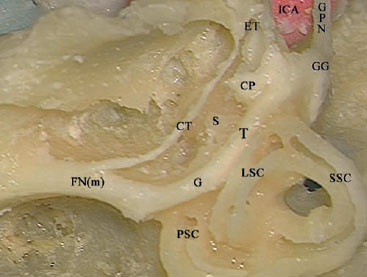
Fig. 2.75 The relationship of the facial nerve to the inner ear as seen from a lateral view of a left temporal bone. CP Cochleariform process, CT Chorda tympani, ET Eustachian tube, FN(m) Mastoid segment of the facial nerve, G Genu, GG Geniculate ganglion, GPN Greater petrosal nerve, ICA Internal carotid artery, LSC Lateral semicircular canal, PSC Posterior semicircular canal, S Stapes, SSC Superior semicircular canal, T Tympanic segment of the facial nerve
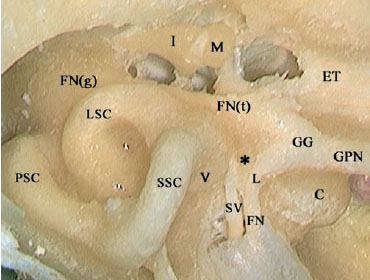
Fig. 2.76 The relationship of the facial nerve to the inner ear seen from a left middle cranial fossa. * Bill’s bar, C Cochlea, ET Eustachian tube, FN Tympanic segment of the facial nerve, FN(g) Facial nerve genu, FN(t) Tympanic segment of the facial nerve, GG Geniculate ganglion, GPN Greater petrosal nerve, I Incus, L Labyrinthine segment of the facial nerve, LSC Lateral semicircular canal, M Malleus, PSC Posterior semi circular canal, SSC Superior semicircular canal, SV Superior vestibular nerve, V Vestibule
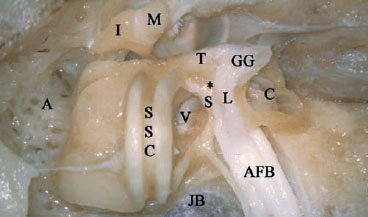
Fig. 2.77 The relationship of the facial nerve to the inner ear, seen from a left middle cranial fossa. In this case, the labyrinth has been opened. * Bill’s bar, AFB Acoustic—facial bundle, A Antrum, C Cochlea, GG Genic ulate ganglion, I Incus, JB Jugular bulb, L Labyrinthine segment of the fa cial nerve, M Malleus, S Superior vestibular nerve, SSC Superior semi circular canal, T Tympanic segment of the facial nerve, V Vestibule
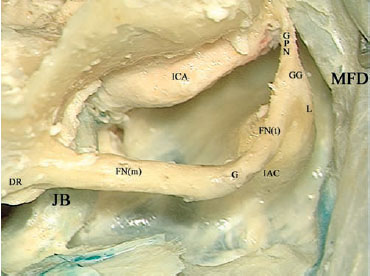
Fig. 2.78 A transotic approach has been used in a left temporal bone, and the whole course of the facial nerve has been skeletonized. Note the wide distance between the low jugular bulb (JB) and the internal auditory canal (IAC). Note also that the mastoid segment of the facial nerve (FNm) is centered on the lateral surface of the jugular bulb. DR Diastric ridge, FN(t) Tympanic segment of the facial nerve, G 2nd genu of the facial nerve, GG Geniculate ganglion, GPN Greater petrosal nerve, ICA Internal carotid artery, L Labyrinthine segment of the facial nerve, MFD Middle fossa dura
< div class='tao-gold-member'>



