CHAPTER 131 Anatomy and Physiology of the Eustachian Tube
Since Eustachius first described the anatomy of his eponymous tube in 1563, understanding of its function in healthy and diseased ears has continued to evolve.1 An anatomic connection between the middle ear space and the nasopharynx was recognized, but the role played by the eustachian tube was unclear. Although this connection was initially thought to be an organ of respiration, later observers realized that it was vital to the health of the tympanic membrane and middle ear as a whole. Pioneering otologists including Toynbee, Politzer, and Bezold developed a paradigm that held that the eustachian tube regulates and modulates the pneumatic status of the middle ear and mastoid to maintain the appropriate milieu for optimal sound transmission by the tympanic membrane and ossicular chain.
Initial concepts regarding the physiology of tubal function were found to be too simplistic. New information has led to a model of the eustachian tube as an “organ” because of its complex anatomy, function, and interdependent relationship with surrounding structures.2 A comparison of early otology texts with contemporary work reveals an evolution of the study of tubal function from limited therapeutics applied directly to the tube to an attempt to understand and modify intrinsic and extrinsic pathologic influences on its function.
Embryology and Postnatal Development
The eustachian tube is derived from the first pharyngeal pouch.3 The endoderm lining the tubotympanic sulcus invaginates between the first and second arch mesoderm to form the tubotympanic recess. The recess expands to form the tympanic cavity and the mastoid antrum. The osseous portion of the tube forms from the petrous and squamous parts of the temporal bone and the greater wing of the sphenoid bone. The cartilaginous tube has at least two discrete centers of chondrification.4 In patients with cleft palate, there is often a deficiency in the development of the lateral lamina.5
The muscles associated with the tube are the tensor veli palatini (TVP), dilator tubae (DT) (which is the medial bundle of TVP muscle),6 tensor tympani (TT), levator veli palatini (LVP), and salpingopharyngeus. These muscles appear early in development and form from the mesenchyme of the first (mandibular) arch together with the muscles of mastication.7 The TVP, DT, and TT are innervated by the mandibular branch of the trigeminal nerve, whereas the LVP is innervated by the vagus nerve.8 The TVP and DT change position during intrauterine development to form a more acute angle with the tube, particularly at the upper portion of the lateral lamina.7,9,10
The eustachian tube is patent during embryologic development, allowing for free flow of amniotic fluid into the middle ear space.11 Early patency explains the occasional finding of keratin and lanugo hairs in the middle ear cleft in infants, and may limit the ability to detect otoacoustic emissions during newborn hearing screening. It is conceivable that this route of entry of squamous epithelium may produce a congenital cholesteatoma, although the more likely mechanism seems to be epidermoid formation from the ectoderm of the first pharyngeal cleft.12
The most rapid development of the petrous and squamous portions of the temporal bone occurs in the first 2 years of life, and eustachian tubal development parallels this.13 Tubal length progresses from 17.5 mm in infants to reach an adult length of 37.5 mm. The length and area of the entire lumen increase more than twofold when comparing adults with young children, although the ratio of the cross-sectional diameter of the lumen to tubal length remains constant.7,14,15
The length of the osseous portion of the tube triples during development, whereas the cartilaginous tube increases 1.6-fold.16 The cartilaginous (nasopharyngeal) portion of the tube is three times as large in adults as in children, and the cross-sectional area, and presumably the efficiency of the dilatory muscles, increases with age.17,18
More significantly, with an increase in cartilage size, there are important changes in cellular composition and shape with aging that result in a less “floppy” tube in adults compared with children. The cartilage cell density decreases in the midcartilaginous portion, and intercellular elastin, present in the hinge region between the medial and lateral laminae, is far more abundant in adults than in children. The medial lamina develops more than the lateral lamina, and when viewed in cross section, the lateral lamina and lateral wall of the tube develop a greater “S” shape. These changes allow for more efficient tubal recoil.14,19–22
Other anatomic changes lead to an improvement in the efficiency of tubal function. During growth, there is a shift in the orientation of the cartilaginous portion to the osseous portion of the tube. When viewed from above, the long axis of the tube describes a greater curve with the increasing inferior and lateral movement of the cartilaginous tube. This augments middle ear protection.16 Additionally, the angle of insertion of the dilatory muscles (DT) becomes more perpendicular to the cartilaginous tube, and the tube becomes more dependent relative to the middle ear cleft.23 All these elements may play a part in the decreased incidence of otitis media with age.15
Anatomy
The function of the eustachian tube in pressure equalization, middle ear protection, and clearance can be understood only when its anatomic subtleties are appreciated. The tube is located in the skull base and connects the anterior portion of the middle ear cleft with the nasopharynx. Its anatomic course brings it close to many critical structures. The general shape of the eustachian tube can be described as two cones joined at their apices. It comprises an osseous, intratemporal portion and a cartilaginous, nasopharyngeal portion. These describe a gentle outward curve when viewed from above as it extends from the middle ear to the nasopharynx (Fig. 131-1).7
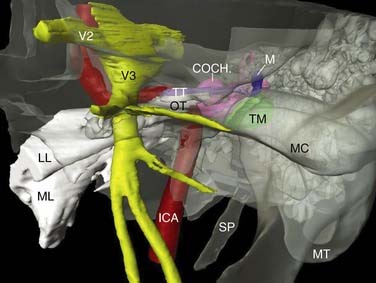
In adults, the osseous portion accounts for less than one third of the length of the tube, and the cartilaginous portion constitutes more than two thirds of the length, even if the central (junctional) region is considered part of the osseous tube.15,16 The orifice of the tube in the middle ear originates in the anterior mesotympanum (protympanum), with the mouth of the tube above the level of the floor of the middle ear. The orifice is not dependent, unless the head is tilted forward. It is triangular to oval in shape with a diameter of 5 mm × 3 mm and marks the entrance to the osseous tube.24 This portion of the tube progresses anteromedially to its isthmus portion along its longitudinal section of the petrous portion of the temporal bone.25 The petrous bone surrounds most of the osseous portion of the tube except for a part of the lateral wall that is surrounded by the sphenoid bone (Fig. 131-2).7 Because of the rigid walls in this anatomic segment, the lumen is always patent, unless obstructed by mucosal thickening or debris.

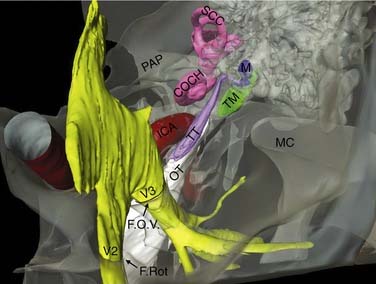
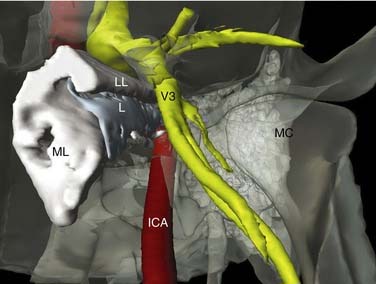
The osseous portion of the eustachian tube lies close to several structures (Fig. 131-3). The glenoid fossa of the temporomandibular joint is lateral and inferior to the osseous tube, the middle fossa dura lies superior, and the internal carotid lies medial. The medial wall of the tube is composed of two parts: a posterior labyrinthine portion and an anterior carotid portion.26 The horizontal segment of the petrous carotid artery is capped by thin bone (see Fig. 131-2). This bone has been found to be dehiscent in 2% of normal adult specimens and exceptionally thin in 22.2%.27,28 Distance between the bony wall and anterior tympanic anulus was found to be an average 4.9 mm. The TT runs just lateral to the midthird of the cochlea. Its semicanal can be found above the osseous tube on the nasopharyngeal side, but runs more medially as it approaches the middle ear. The average distance from the lumen of the tube to the dura of the middle fossa is 3.6 mm.24 All these structures are in jeopardy when the tube is surgically manipulated, and caution must be exercised when removing disease from the lumen.
Approximately 33% of patients have pneumatization of the petrous apex, and the osseous tube can be variably surrounded by peritubal air cells. Computed tomography (CT) has revealed that in 92% of patients, these cells can open directly into the osseous tube anterior to its tympanic orifice. This opening may play a role in persistent cerebrospinal fluid rhinorrhea after cerebellopontine angle surgery despite packing of the tympanic orifice of the tube.29
The osseous portion of the tube progressively narrows as it approaches the cartilaginous portion. Small endoscopes 0.8 mm in diameter are able to pass through this region.30 At its most anterior tip, the fibrocartilage of the cartilaginous tube extends slightly into the lumen of the bony canal. This area has been called the isthmus; however, it is not the narrowest part of the tube. Histopathologic studies measuring the circumference of the internal lining and the cross-sectional area of the tube have revealed that the narrowest portion of the tube in the closed and in the fully open positions lies in the proximal cartilaginous tube. Sando and coworkers15 proposed that the divisions of the eustachian tube be reclassified as osseous (lumen surrounded by bone), cartilaginous (lumen surrounded by cartilage), and “junctional” (lumen surrounded by bone and cartilage) (Fig. 131-4).
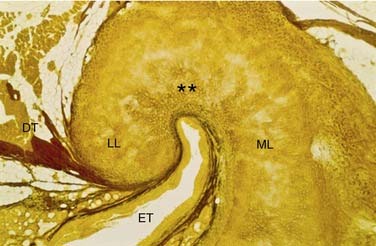
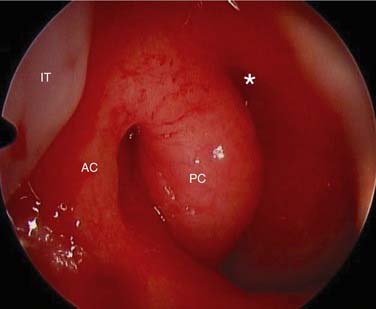
The cartilaginous portion of the tube has a complex shape reflecting the nuances of its function (Fig. 131-5). It is composed of two distinct rhomboidal plates when viewed from the side, with a large medial lamina and a much smaller lateral lamina. These are joined at the apical hinge region. In three dimensions, the cartilage is bell-shaped with a largest transverse diameter of 9 mm. When viewed from the nasopharynx, the fibrocartilage is in a distinct “crook” shape with the longer arm located medially. Its projection into the nasopharynx is covered by a layer of respiratory mucosa and is distinctly seen on nasopharyngoscopy as the torus tubarius. Although the laminae are principally composed of fibrocartilage, the hinge region contains an abundance of elastic cartilage allowing for efficient tubal opening (Fig. 131-6). The nasopharyngeal opening of the eustachian tube lies opposite the lateral aspect of the choana behind the posterior end of the inferior turbinate. It is partially protected from nasal airflow. This location makes blind cannulation of the tube challenging.
At the skull base, the cartilaginous tube is fixed superiorly to a shallow depression in the bone of the greater wing of the sphenoid (sulcus tubarius). Laterally, it is held in place by the medial pterygoid plate. This base of support prevents vertical and rotational movement of the pliable cartilage during opening. The angle the tube forms with the Frankfort horizontal plane has previously been estimated in infants and children, using gross anatomic measurements, to be approximately 10 degrees. As the skull and midface expand vertically, and the hard and soft palates descend, this angle increases to 45 degrees in adults.3 Imaging studies have revealed these angles in a Japanese population to be approximately 20 degrees in infants and children and 27 degrees in adults, with adult angles reached at approximately 7 years of age.31
The adenoid pad occupies the area between the nasopharyngeal openings of the tubes. A depressed space medial to each torus forms the fossa of Rosenmüller, an area of particular interest in the diagnosis of nasopharyngeal carcinoma (Fig. 131-7). This fossa extends posterolaterally and superiorly to the area behind the midportion of the tube. The distance between the deepest part of the fossa and petrous apex was found to be only 4 mm.32 Above this lies the foramen lacerum, a hiatus between the sphenoid and petrous bones, through which nasopharyngeal tumors may spread intracranially.
The muscles that allow for opening of the cartilaginous tube are arranged in a complex fashion. The principal and perhaps only dilator of the tube is the tensor TVP. It is composed predominantly of fast-twitch muscle fibers, but also contains slow-twitch fibers to maintain tone.18 This muscle has several distinct segments. The main body of the muscle originates in the base of the skull at the angular spine of the sphenoid and the scaphoid fossa at the root of the medial pterygoid plate. It progresses in a lateral and anteroinferior direction to curve around the hook of the hamulus.15 As it becomes tendinous, it fans out to insert into the aponeurosis of the soft palate and posterior edge of the hard palate. Secondary attachments in the maxillary tuber and the palatoglossal arch may be important in preserving muscle function after infraction of the hamulus during cleft palate repair surgery.33
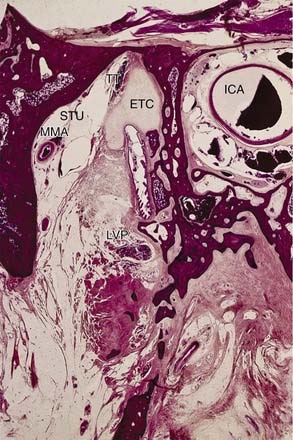
The TVP is said to have three anchoring points on which it isometrically contracts: the pterygoid hamulus, Ostmann’s fat pad, and the medial pterygoid muscle (Fig. 131-8).34 The fibers roughly parallel the plane of the lateral lamina of the cartilaginous tube. An additional segment of the TVP originates from the area of the hamulus and projects more perpendicularly to this plane. It attaches to the short lateral lamina of the cartilaginous tube and to a condensation of connective tissue lateral to the tubal wall and a portion of Ostmann’s fat pad.35,36 This segment has been termed the DT and may be a separate muscle.

Less important dilators of the cartilaginous tube include the levator veli palatini (LVP) and the salpingopharyngeus muscles. The LVP originates from the petrous apex. Here it lies medial to the tube, but its anterior segment is immediately inferior to the floor of the tube, separated by connective and fatty tissue.15,16 It inserts in a radiating fashion into the nasal surface of the soft palate. The LVP has been observed to facilitate tubal opening by elevating the floor of the tube and moving the medial lamina toward the midline during contraction. The salpingopharyngeus attaches to the edge of the cartilaginous tube medially and is directed inferolaterally. Its role in tubal function remains speculative. Swallowing, yawning, and clenching teeth may activate all these muscles.37
The histology of the tubal lumen is vital to its action. The bony canal is lined by a prolongation of the low cuboidal, ciliated mucosa of the middle ear. After the junctional region is passed, the mucosa transitions to pseudostratified, ciliated, columnar epithelium identical to the epithelium lining the upper respiratory tract.38 The density of ciliated and goblet cells gradually increases in a distal and inferior direction.39,40 Within the cartilaginous tube, the floor of the triangular-shaped lumen is different than the walls. The floor contains an abundance of mucus-producing goblet cells and is heavily rugated; in the upper half of the tube, the walls contain far fewer goblet cells and are generally smooth. It has been suggested that the lower half of the tube is principally involved with clearance of the mucociliary blanket, whereas the upper half is important to pressure equalization and gas exchange.15
Mucosa-associated lymphoid tissue is found submucosally throughout the eustachian tube and is particularly prominent around the inferior half of the cartilaginous tube.41 This tissue may be a factor in luminal obstruction when inflamed. The lateral mucosal wall is bounded laterally by a collection of adipose tissue termed Ostmann’s fat pad.42,43 This tissue represents one segment of a collection of adipose tissue around the tube and is in the shape of a cone with the base anterior. During conditions of metabolic stress, loss of this fat results in an abnormally patulous eustachian tube.
The arterial supply to the osseous tube consists of a branch of the accessory meningeal artery called the tubal artery and the caroticotympanic arteries arising from the internal carotid artery. The superior tympanic artery, which originates from the middle meningeal artery, supplies the TT. The deep auricular and pharyngeal arteries from the internal maxillary artery, the ascending palatine artery, and the ascending pharyngeal artery supply the cartilaginous tube. The venous drainage generally parallels the arterial supply with the pterygoid venous plexus of particular importance.44,45 Manipulation and air insufflations of the eustachian tube can result in intracranial complications owing to intracranial venous anastomoses, proximity of the internal carotid artery, and potential osseous dehiscence of the skull base.46–50
Physiology
Pressure Equalization
In its resting state, the cartilaginous tube is closed at its nasopharyngeal orifice. As pressure external to the middle ear cleft changes with fluctuations in atmospheric pressure and during nonphysiologic pressure alterations (e.g., airplane flight, diving in water), it must open to equalize middle ear pressure to ambient pressure. This opening allows for a state conducive to efficient sound conduction through the tympanic membrane and ossicular chain. This pressure equilibration is also accomplished by bidirectional gas exchange and transudation of fluid.51
During swallowing, the muscles that dilate the eustachian tube are activated; this occurs during a pause in respiration in the expiratory phase.51 As the soft palate is elevated and seals the nasopharynx, the TVP isometrically contracts providing a base of support for the DT. This muscle pulls on the lateral lamina and the connective tissue lateral to the tube. The superior half of the tube is typically C-shaped at rest. With lateral movement of the lateral lamina, owing to the hinge action between the laminae where the elastin fibers are in abundance, it becomes more circular in cross section.3,14,52 The medial lamella remains relatively rigid, and the sequence of muscular contraction allows for concerted tubal opening and flow of gas. Because the cartilaginous tube extends slightly into the osseous tube between the semicanal of the TT and the tubal lumen, there is no crimping of the tube during dilation. Other mechanisms that can initiate tubal opening include yawning, sneezing, and, in some patients, forced pressurization by swallowing with a closed glottis (Toynbee maneuver) or with insufflations of air (politzerization).
Slow-motion videoendoscopy has revealed four steps in tubal opening: (1) palatal elevation with medial movement of the lateral pharyngeal wall and medial rotation of the medial lamina (initiation of opening of the distal cartilaginous tube presumably by the LVP), (2) lateral movement of the lateral wall with dilation of the orifice laterally and vertically, (3) propagation of dilation of the tubal lumen from distal to proximal by the TVP/DT, and (4) opening of the proximal cartilaginous tube adjacent to the junctional region with formation of a round to crescent-shaped lumen.53 During this event, the tube remains open for 0.3 to 0.5 second, but is open much longer during yawning.51 In normal individuals, the eustachian tube fully opens once or twice hourly.54
To be fully opened, the dilatory muscles must overcome the intraluminal surface tension generated by the apposition of the mucosal surfaces. Surfactant protein B, similar to that obtained in bronchoalveolar lavage, has been identified in the secretory granules of surface cells lining the eustachian tube. The ability of surfactant to reduce the opening pressure in the eustachian tube has been shown experimentally.55–58 The surface tension in the normal eustachian tube is typically 58 mN/m, but is elevated in serous and mucoid otitis media.56,59 Tubal surface tension is also influenced by the amount and composition of tubal secretion. This is under control of the autonomic nervous system, and increased parasympathetic transmission has been shown to impair tubal opening.60
Tubal closure depends on adhesion of the intraluminal mucous blanket, elastic forces of the supporting tissues, and hydrostatic pressure of venous blood.51 The position of Ostmann’s fatty tissue in the posterolateral half of the tube enables it to assist in restoring the tube to its closed position.61
According to the classic theory of eustachian tube dysfunction suggested by Politzer in the 19th century, the gas contained in the middle ear/mastoid system tends to be absorbed into the bloodstream by the capillaries of the middle ear/mastoid mucosa when the tube is hermetically sealed.62 This was termed the “hydrops ex-vacuo” model. Although under normal conditions the middle ear maintains a very slight negative pressure a few millimeters of H2O lower than the nasopharynx, unless the tube periodically opens, the absorption of gas would result in a large negative pressure differential.63 Mechanical obstruction of the tube or impaired opening of the tube predisposes to middle ear pathology. In histologic specimens of patients with otitis media, the cross-sectional area of the tubal lumen tends to be smaller than in patients without otitis media, particularly in the osseous portion.64 This is due to a combination of submucosal inflammatory infiltrates and an increased density and hyperplasia of goblet cells.65
The continuity of the middle ear cleft to the volume of gas in the mastoid air cell system is likely to be important in pressure equalization. Bluestone and colleagues66
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


