Fig. 52 The extracranial surface of the right temporal bone with its sutures seen in the normal position. It is divided into: 1) The squamous part with the large temporal squama, the zygomatic process, and the mandibular fossa. 2) The mastoid part, with the mastoid process and the mastoid cortex situated within the petrosquamous parietomastoid and occipitomastoid sutures. 3) The tympanic part, consisting of the tympanic bone, forming the external acoustic meatus between the tympanomastoid suture (TM) and the tympanosquamous suture (TS), continuing into the petrotympanic suture (PT) within the mandibular fossa. The mastoid foramen (MF) is the opening for the emissarium occipitale. 4) The petrosal part, involving the medial structures of the temporal bone, is not visible in this figure, except for the middle ear.
The Extracranial Surface of the Temporal Bone
After exposure of the mastoid process using the retroauricular approach (Fig. 25) or the endaural approach (Fig. 24), the suprameatal spine (Henle’s spine), situated posterosuperiorly at the entrance of the ear canal, has to be located. The shape and position of the suprameatal spine varies. Anson and Donaldson (1992) describe four variants of the suprameatal spine, the styloid process and the tympanic bone:
Variant 1. The suprameatal spine is small and smoothly contoured. In these cases, the tympanic bone, forming the anterior wall of the external acoustic meatus, is a vertical plate, and the styloid process is very short (Fig. 53). A straight external acoustic meatus provides the best visualization of the drum and tympanic cavity, and is the most favorable shape for tympanoplasty.
Variant 2. The suprameatal spine is a sharp and elongated crest (Fig. 54). The deep tympanosquamous suture deludes a prominent anterior part of the tympanic bone, but the bone is a thin and straight plate that provides good access to the middle ear. The skin is difficult to elevate from the deep suture, and the bone itself is not prominent. The styloid process is short.
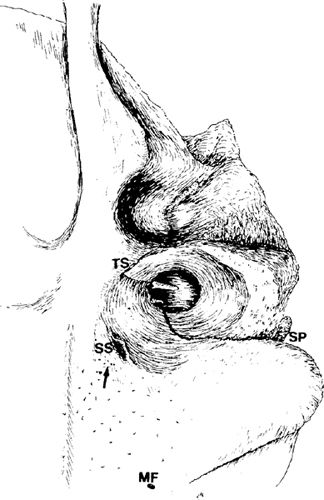
Fig. 53 The surface of the temporal bone, as seen by the surgeon sitting behind the patient. The suprameatal spine (SS) is small. The tympanic bone at the tympanosquamous suture (TS) is not prominent, and the anterior part of the tympanic bone is a vertical plate, allowing a relatively wide ear canal. The styloid process (SP) is very short. The course of the tympanomastoid suture posteriorly in the ear canal and the tympanosquamous suture superiorly (TS) is shown. MF: mastoid foramen, (MF), the cribriform area (arrow)

Fig. 54 The surface of the temporal bone. The suprameatal spine is a sharp and elongated crest (small arrows). The tympanosquamous suture is deep (large arrow), but the anterior part of the tympanic bone is a thin, straight plate, allowing good visualization of the tymponomeatal angle. The styloid process is short. The suprameatal spine is placed posterosuperiorly in the cortex of the mastoid process, and is in fact only a small groove for entrance of the vessels coming from the antrum. The styloid process is long. The anterior part of the tympanic bone is thick and prominent
Variant 3. The aperture for vessels lies somewhat superoposteriorly, close to the temporal line, and there is no true suprameatal crest, only a cone-shaped depression. The styloid process is relatively long (Fig. 55). The anterior part of the tympanic bone is thick and prominent.
Variant 4. The suprameatal area is smooth, and there is no suprameatal crest. The external auditory meatus is oval in outline, and the tympanic part of the temporal bone, forming the anterior wall of the ear canal, is prominent. The styloid process is very long (Fig. 56).
The temporal line is a horizontal ridge, continuing from the superior border of the zygomatic process posteriorly onto the mastoid cortex (Fig. 52). The temporal line is not always evident. Sometimes it is a prominent sharp ridge (Figs. 53, 57), sometimes a broad prominence (Fig. 55), and in some other cases it is hardly recognizable (Figs. 54, 56). It is safest to start drilling the mastoid cortex a few millimeters below the temporal line and gradually proceed towards it.

Fig. 55 The surface of the temporal bone. There is no true suprameatal crest, only a cone-shaped depression close to the temporal line (arrow). The styloid process is long, and the tympanic bone is thick and prominent

Fig. 56 The surface of the temporal bone. The suprameatal spine is not present. The anterior part of the tympanic bone is very prominent and thick (arrow). The ear canal is oval, the tympanosquamous suture is deep, and the styloid process is very long
Posterior to the suprameatal spine, a group of small holes in the mastoid cortex are occasionally seen, described as the cribriform area (Fig. 53). Small vessels pass through these foramina to the mucosa of the underlying antrum in infants, and it is here that a subperiosteal abscess forms in cases of acute coalescent mastoiditis. The cribriform area lies within Macewen’s triangle (Fig. 57), an imaginary triangle defined by three lines. The first line is the temporal line; the second is formed by the superior and posterior margins of the external bony meatus (this line goes through the suprameatal spine). The triangle is completed by a line drawn perpendicular to the first line and tangential to the second. Macewen’s triangle roughly defines the mastoid antrum deep to the cortex.
Posteriorly, alongside the occipitomastoid suture, the mastoid foramen is visible, and this is the opening of the emissarium occipitale (Santorini) (the occipital emissary vein) connecting the veins of the occipital region with the sigmoid sinus (Fig. 52).
The roof of the bony ear canal is an important landmark, and should be visualized in any type of mastoidectomy except simple mastoidectomy. The canal skin should be carefully elevated, and the tympanosquamous suture should be located at the 12-o’clock position and exposed. The skin is firmly attached at the suture by fibrous tissue, which should be cut with a sickle knife in order to expose the entire suture. The size of the tympanosquamous suture varies from a small, barely recognizable fissure (Fig. 57) to a deep notch, hampering the view of the Shrapnell’s membrane region (Fig. 58). Any irregular bone in the superior part of the ear canal should be drilled away in any type of mastoidectomy. A deep tympanosquamousal suture can also be described as a fissure.
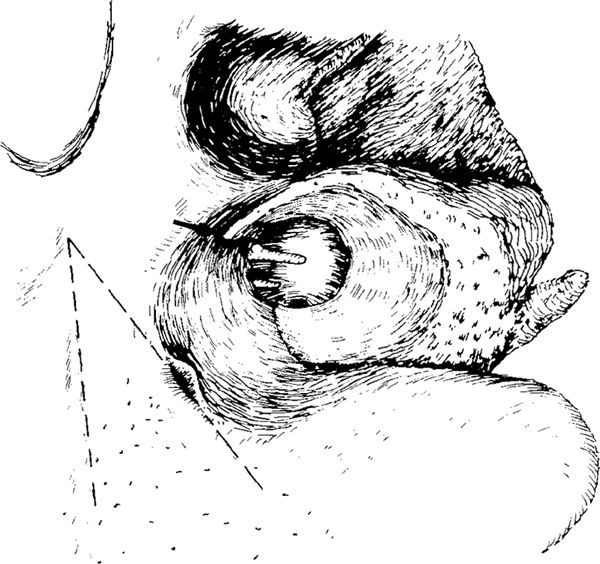
Fig. 57 The bony ear canal, with a barely recognizable tympanosquamous suture (arrow). The temporal line is a sharp ridge, and Macewen’s triangle is indicated (dashed line)

Fig. 58 The bony ear canal, with a deep tympanosquamous suture (arrow) and a prominent notch on the anterior part of the tympanic bone

Fig. 59 The hypotympanum. The tympanic bone has been removed to illustrate anatomic relationships in the hypotympanum. P: the promontory, with the oval window superiorly, the round window niche posteriorly, and the hypotympanic cells inferiorly. JB: the jugular bulb fossa; the entrance of the carotid artery (arrow) and its course through the temporal bone (dashed lines)
The floor of the ear canal is formed by the tympanic bone, and should also be visualized before the mastoidectomy, at least as far as the tympanomastoid suture, which starts medially at the bony annulus at the 9-o’clock position and continues inferolaterally towards the apex of the mastoid process (Figs. 53, 58). Sometimes extensive drilling of the tympanic bone needs to be performed in order to visualize the lower part of the posterior tympanum or the hypotympanum in cases of cholesteatoma or glomus tumor. Removal of the tympanic bone between the two fissures gives an excellent view of the entire hypotympanum and carotid canal (Fig. 59).
The Mastoid Process–The Mastoidectomy
After the temporal line, the suprameatal spine, Macewen’s triangle, the roof and floor of the ear canal, the tympanosquamous and the tympanomastoid sutures, and the tip of the mastoid process (Figs. 52, 53) have been identified, the cortical bone is removed from the surface using a large cuttting burr, starting behind the suprameatal spine within Macewen’s triangle. After wide cortical bone removal, exenteration of the lateral mastoid air cells is performed (Fig. 60). The anatomy of the lateral part of the mastoid process varies widely in relation to the degree of pneumatization, which can be almost nonexistent, with no cells at all, or extensive, with complete pneumatization of the mastoid process, thin cortical bone, and many large and small cells extending subcortically posterior to the sigmoid sinus. Toward the tip of the mastoid process, the cells are usually larger (Fig. 60).
Middle Cranial Fossa Dural Plate
Superiorly, the middle cranial fossa dura plate has to be located. This is achieved by drilling superiorly in the mastoid process, toward the temporal line (Fig. 60). The mastoid air cells superiorly lie just under the cortical bone, and end in a solid bony plate. This plate continues medially (Fig. 61). When the bone at the middle cranial fossa dura plate is thinned, the dura becomes visible, a pinkish color initially showing through the thin bony plate, followed by the whitish color of the dura itself or by bleeding from small dural vessels. The pinkish color is due to the vascularization of the dura.
Laterally, the middle fossa dura plate is large. It extends from the zygomatic region anteriorly to the sinodural angle and the superior petrosal sinus posteriorly (Fig. 61). Because the superior petrosal sinus runs in an anteromedial direction, the area of the middle fossa dura plate diminishes medially toward the labyrinth.
The middle fossa dura plate is the roof, or tegmen, of the pneumatized spaces of the temporal bone. The tegmen is divided into the tegmen mastoidei, the most lateral part; the tegmen antri at the level of the mastoid antrum; and the tegmen tympani at the level of the epitympanum, extending medially as far as the superior semicircular canal and the epitympanic recess anteriorly (Fig. 61).
There is some disagreement about the nomenclature for the tegmina. Anson and Donaldson (1992) use only the term tegmen tympani. Proctor (1989) uses both the terms tegmen tympani and tegmen antri, and as well as these Proctor uses the terms squamosal tegmen for the area lateral to the petrosquamous lamina (Körner’s septum), and petrosal tegmen for the area medial to it. Some surgeons use the term tegmen tympani for the entire middle fossa dural plate while others reserve the term for its medial part. The present author believes that this large and surgically important area of middle fossa dura plate should be topographically subdivided into three parts, allowing for more precise description of the pathology and surgical techniques associated with it, and therefore suggests the terms tegmen mastoidei for the most lateral part; tegmen antri for the middle part, forming the roof of the mastoid antrum; and tegmen tympani for the most medial part, forming the roof of the epitympanum and pretympanic recess (Fig. 63).
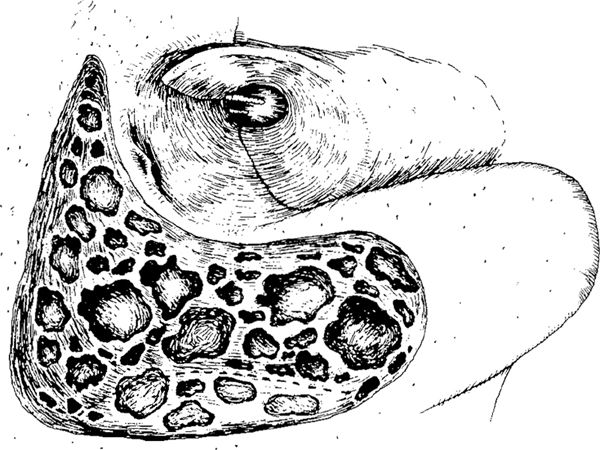
Fig. 60 The subcortical lateral region of the mastoid process in a case of extensive pneumatization, with large and small air cells occupying hte subcortical space of the entire mastoid process. The cortical bone is relatively thin. Superiorly, the middle fossa dura plate is indicated, and posteriorly, the approximate position of the lateral sinus is indicated by dashed line
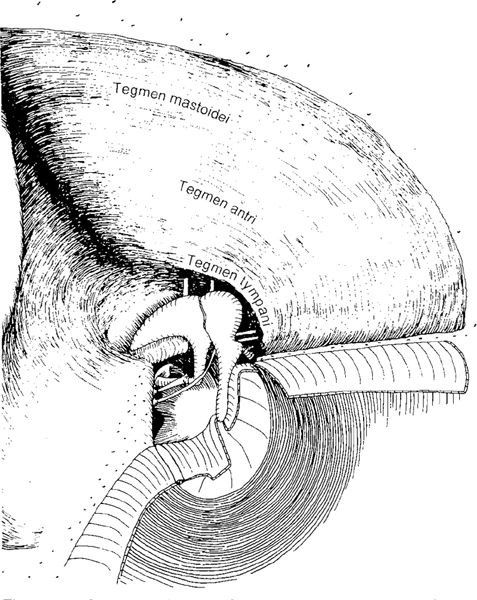
Fig. 61 Division of the middle fossa dura plate into the tegmen mastoidei, tegmen antri, and tegmen tympani in a large canal wall–down mastoidectomy. The sinodural angle and sigmoid sinus are shown (inferosuperior view seen in the normal position)
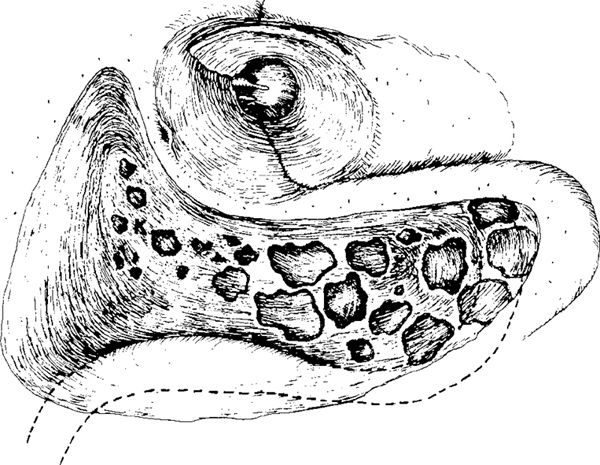
Fig. 62 Cortical mastoidectomy, with exenteration of the lateral mastoid air cells. There are large mastoid cells at the tip of the mastoid process, lateral to the sigmoid sinus. Superiorly, the mastoid cells are removed until Körner’s septum (K) is reached and the middle fossa dura plate is exposed. Posteriorly, the most lateral part of the sigmoid sinus is exposed, and its further course towards the mastoid tip under the facial nerve is indicated
The Sigmoid Sinus
The posterior limit of the standard mastoid cavity is the sigmoid sinus, or lateral sinus. It is a continuation of the transverse sinus, and passes through the deep part of the mastoid process, under the facial nerve, toward the jugular bulb. In a well-pneumatized mastoid process, the lateral aspect of the sigmoid sinus is covered by mastoid air cells (Fig. 60). After removal of these cells, a slightly bluish discoloration of a smooth bony plate can be seen (Fig. 62). With further thinning of the bone over the sinus, it becomes increasingly blue. The sigmoid sinus usually lies a few millimeters deep to the cortex of the mastoid process. The posterosuperior part of the sigmoid sinus is at the most superficial level (Fig. 63). Inferiorly, the sinus lies gradually deeper, making an anterior curve and crossing the tip of the mastoid process at a level deep to the digastric crest. Adjacent to the vertical portion of the facial nerve, before forming the jugular bulb, the sigmoid sinus lies deepest (Fig. 64).
The anatomy of the sigmoid sinus varies. In relation to the ear canal, it can be positioned either anteriorly or posteriorly. Some investigators have found that the anteriorly positioned sinus is more common in ears with poor pneumatization (Heermann and Riehm 1961). We suspected the same tendency, but after measuring temporal bones, there was no significant correlation between the distance from the sigmoid sinus to the ear canal and the degree of pneumatization (Turgut and Tos 1992a).
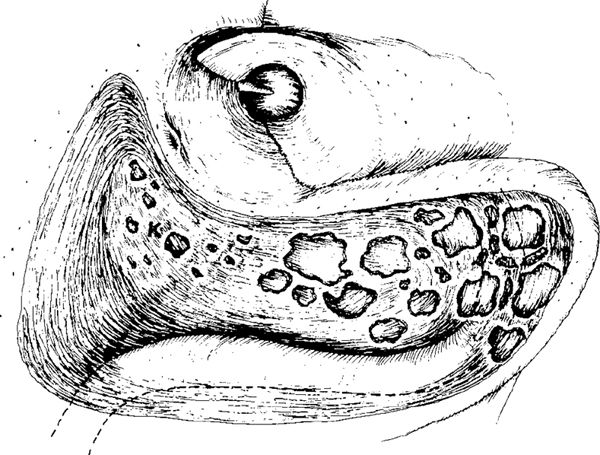
Fig. 63 Cortical mastoidectomy, with further exposure of the sigmoid sinus and the middle fossa dura plate and exenteration of the air cells as far as Körner’s septum (K). At the tip of the mastoid, there are large air cells lying lateral to the sigmoid sinus
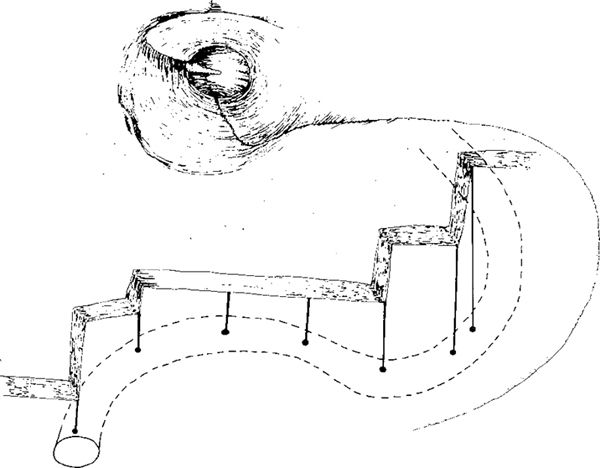
Fig. 64 The position of the sigmoid sinus in relation to the mastoid cortex (schematic). The most superficial position of the sinus is at its posterosuperior part. Toward the tip of the mastoid process, the sinus lies considerably deeper. Under the facial nerve and toward the jugular bulb, it is at its deepest
The Sinodural Angle
The sinodural angle is the angle between the middle fossa and posterior fossa dura plates and the superior part of the sigmoid sinus (Fig. 61). In a well-pneumatized ear, small air cells usually occupy the sinodural angle, and should be removed or opened in a mastoidectomy. Sometimes it is necessary to drill deep down into the angle, exposing the superior petrosal sinus (Figs. 65, 66). Laterally in this angle within the mastoid cortex, the emissarium mastoideum (Citelli) is located. This emissary vein connects the sigmoid sinus with the veins draining the middle fossa dura and the temporal squama. The veins may lead to troublesome venous bleeding during the drilling of the cortical bone in the most lateral part of the sinodural angle. The sinodural angle is usually deep. In the depths of the angle, the superior petrosal sinus is located (Fig. 66). The superior petrosal sinus enters the sigmoid sinus on its medial surface, and runs in a bony sulcus along the edge of pars petrosa, dividing the middle fossa dura plate from the posterior fossa dura plate (Fig. 67). It runs medially toward the petrous apex (Fig. 66).
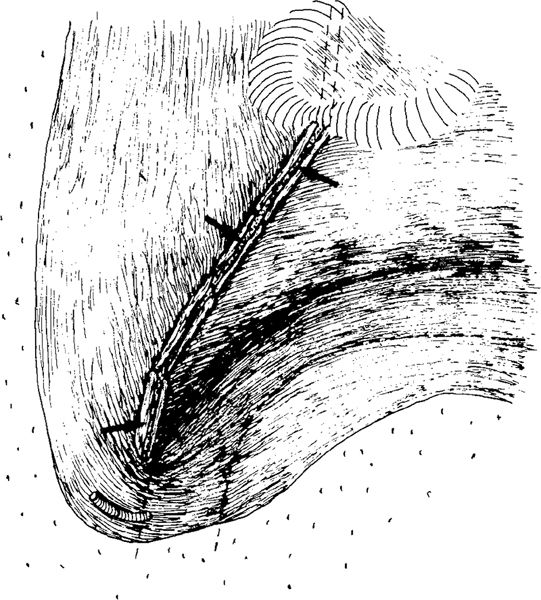
Fig. 65 The sinodural angle, with the superior petrosal sinus partly exposed (arrows)

Fig. 66 The superior petrosal sinus in the sinodural angle. The dura totally exposed. It runs from the medial (inner) aspect of the sigmoid sinus, deep in the sinodural angle within the duplicature of the dura, in a medial direction beweeen the superior and posterior semicircular canals. Arrow: emissarium mastoideum (Citelli)
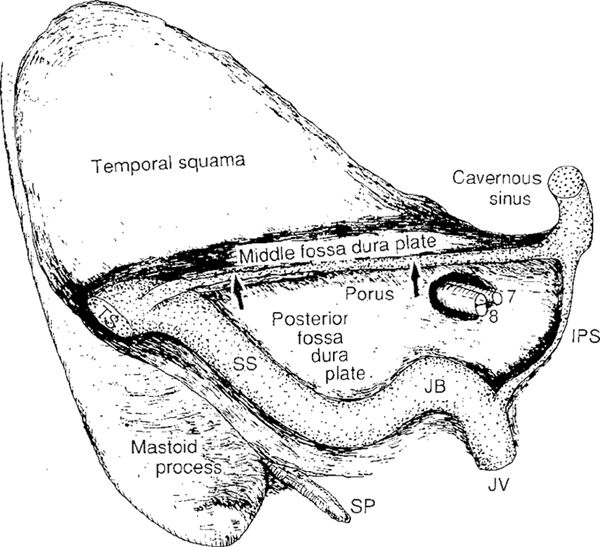
Fig. 67 The inner surface of the temporal bone. The superior petrosal sinus lies in its sulcus (arrows) between the middle and the posterior fossa dura plates, connecting the sigmoid sinus (SS) and the cavernous sinus. The inferior petrosal sinus (IPS) connects the cavernous sinus and the jugular bulb (JB). JV: jugular vein, TV: transverse sinus, SP: styloid process
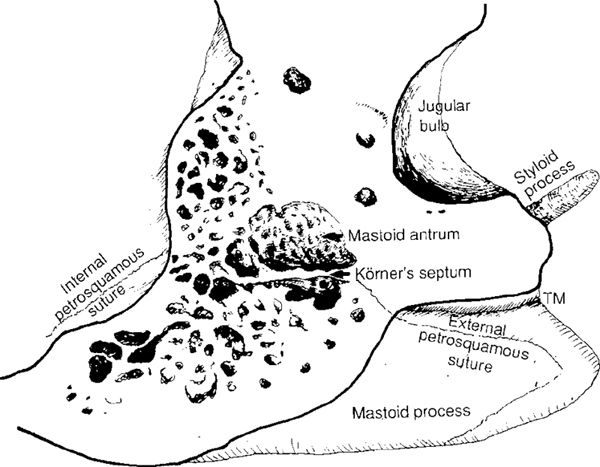
Fig. 68 Vertical section through the right temporal bone, partly redrawn after Proctor (1989), showing a well-preserved petrosquamousal lamina (Körner’s septum, arrow) continuing superiorly into the internal petrosquamous suture and inferiorly into the external petrosquamous suture, dividing the superficial lateral mastoid cells for these structures into squamomastoid cells and petromastoid cells lying medially to the sutures
Körner’s Septum
After exenteration of the superficial mastoid air cells (Fig. 62), a bony plate can be seen at the bottom of the kidney-shaped cavity. This plate is Körner’s septum, or the petrosquamous lamina. In a well-pneumatized mastoid process, the plate of Körner’s septum is hardly recognizable (Körner 1899). It is indicated by somewhat smaller cells in the upper part of the cavity (Fig. 63), but in the lower part, large cells can be present at the level of Körner’s septum. Körner’s septum represents the site of embryological fusion of the squamous and petrous portions of the temporal bone. Between the two components there is a sutural line that is normally obliterated. Occasionally, however, a plate of bone persists between the two parts, called Körner’s septum (Figs. 68, 69). Körner’s septum may give a false impression of having reached the antrum (Ballance 1919, Caparosa 1972, Goycoolea et al. 1989). When this bony septum is present it divides the mastoid process into a superficial-(squamous)-portion and a deep-(petrosal)-portion, both portions open separately into the antrum (Fig. 69) (Proctor et al. 1981, Proctor 1989). If the squamous portion is poorly pneumatized (Fig. 70) or sclerotic, there may be great difficulty finding the mastoid antrum, unless the surgeon is aware that Körner’s septum—the petrosquamous lamina—is present and must be penetrated to reach the air cells in the deep portion of the temporal bone. Schullmann and Rock (1972) pointed out that Körner’s septum should be considered: 1) if there is difficulty in approaching the antrum; 2) if the antrum is small and constricted; and 3) if it is felt that the antrum has an anomalous position.

Fig. 69 A similar vertical section through the entire temporal bone, including the petrosal apex, at the level of the vertical portion of the facial nerve, illustrating Körner’s septum (arrows), with the mastoid antrum and petromastoid cells medial to it and the squamomastoid cells lateral to it (partly redrawn after Proctor 1989)
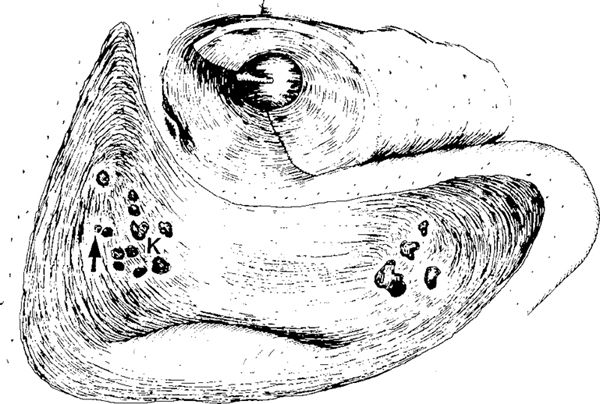
Fig. 70 Thick Körner’s septum (K) in a poorly pneumatized mastoid process and only few small cells, which should be followed along the middle fossa dura plate toward the antrum (arrow)
Whenever a persistent and dense Körner’s septum is found, it should be removed to eliminate a dual pneumatic system (Goodhill 1978). Failure to recognize the presence of Körner’s septum may lead the surgeon to seek the antrum at a more superficial level. During this procedure, the surgeon may wrongly search for the antrum anteroinferiorly, and may expose and damage the facial nerve. In such cases, drilling along the middle fossa dura plate is therefore extremely important until the antrum and lateral semicircular canal are located.
Mastoid Antrum
Passing the petrosquamous lamina or Körner’s septum in an anterosuperior direction along the middle fossa dura plate, the antrum is reached (Figs. 68, 69). The antrum varies considerably in size; in a small, sclerotic mastoid with little or no pneumatization, the antrum is quite small. In ears with extensive peneumatization, it can be voluminous. In ears with no petrosquamous lamina, there is no border between the large mastoid cells and the antrum. In such cases, the antrum is huge. Anterosuperiorly, the antrum continues along the tegmen to a narrow passage, the aditus ad antrum to the epitympanum.
The superior wall of the antrum is the tegmen antri (Fig. 61). The medial wall of the antrum cavity is the labyrinth. Anteriorly, the lateral semicircular canal is immediately recognizable, and lateral to the canal, the incus body and short process of the incus are seen. The posterior and superior semicircular canals are not visualized; they are covered with small air cells or bony spicules (Fig. 71). The bone surrounding the antrum may be sclerotic, pneumatized with small air cells, or spongiotic in children.
The Labyrinth
When the antrum is entered, the prominence of the lateral semicircular canal should be visible, and this is the most important landmark in the antrum (Fig. 71). After further removal of the air cells around the superior and posterior semicircular canals, the canals are also visualized (Fig. 72). The superior semicircular canal runs perpendicularly to the lateral canal, but is about 2 mm deeper (Fig. 73). The anterior junction of the superior and lateral semicircular canals is at the anterior ampulla. The anterior crus then runs superiorly toward the tegmen tympani, and curves posteriorly to join with the posterior semicurcular canal at the common crus (Fig. 74). The posterior semicircular canal also runs perpendicularly to the lateral semicircular canal. The posterior half of the posterior canal is located posterior to a line bisecting the lateral semicircular canal (Fig. 75) (Donaldson’s line; Anson and Donaldson 1992). The anterior half of the posterior canal runs anteriorly to the Donaldson’s line and emerge deep to the facial nerve, to enter the vestibule.
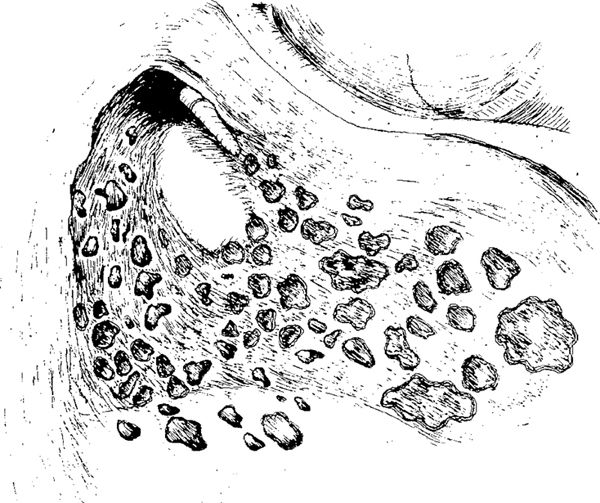
Fig. 71 Exposure of the mastoid antrum in mastoidectomy of a well-pneumatized ear. Anteriorly, one can see the incus, malleus, and intact ear canal wall, medially the lateral semicircular canal, and superiorly the tegmen antri. The antrum is surrounded by numerous small periantral air cells, and it communicates anteriorly with the epitympanum through the aditus ad antrum, which is a narrow space between the lateral semicircular canal and the middle fossa dura plate
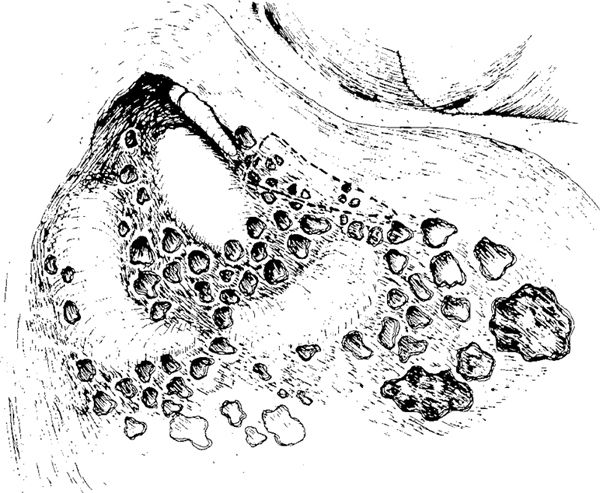
Fig. 72 The semicircular canals. The periantral and some of the perilabyrinthine air cells are removed, exposing the most prominent parts of the three semicircular canals: lateral, superior, and posterior. In well-pneumatized ears, these are surrounded by numerous small air cells. The facial recess is indicated by the dashed lines forming a triangle inferior to the incus
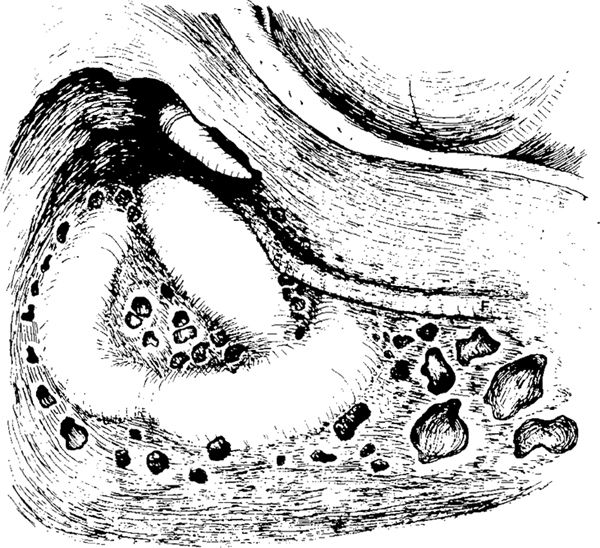
Fig. 73 The supralabyrinthine, infralabyrinthine, and retrolabyrinthine air cells are opened, and the contours of the three semicircular canals are clearly visualized. Anteriorly, the facial nerve (F) is skeletonized
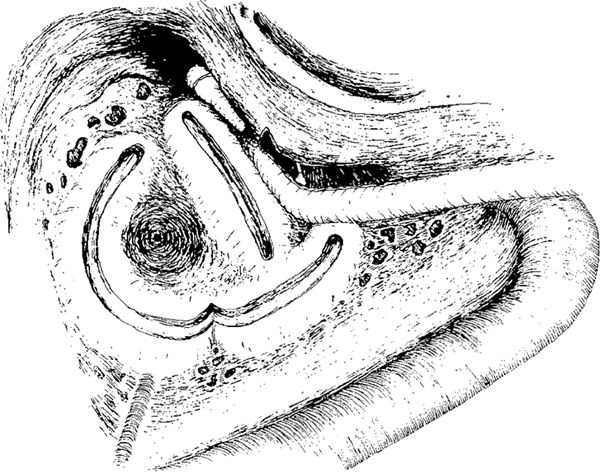
Fig. 74 The anatomy of the open semicircular canals and their relation to the facial nerve. The inter-labyrinthine air cells have been removed, and the opening for the labyrinthine arteria in the middle of the inter-labyrinthine region is visible. Some supralabyrinthine and retrolabyrinthine cells are opened. Infralabyrinthine cells lying inferior to the posterior semicircular canal are visible. Anteriorly, the vertical portion of the facial nerve with its genu is seen. It continues to the horizontal part of the facial nerve situated anteriorly to the lateral semicircular canal. Between the bony ear canal and the vertical portion of the facial nerve, the facial recess is opened. Through the recess, the pyramidal process and the tendon of the stapedial muscle are visible. Posterior to the labyrinth, the posterior fossa dura plate with the skeletonized sigmoid sinus is seen; it runs in an anterior direction under the facial nerve
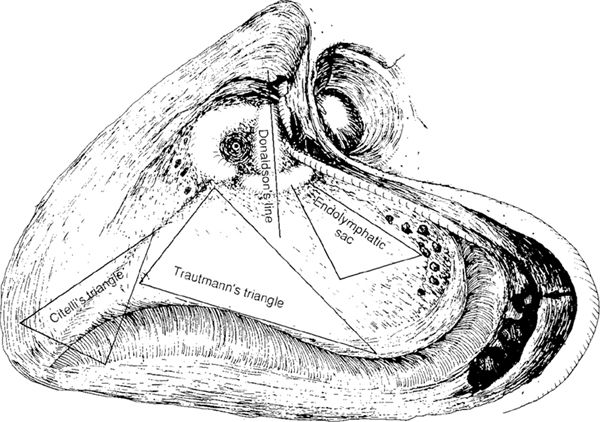
Fig. 75 Completed extended mastoidectomy with intact canal wall and posterior atticotympanotomy: superiorly, the entire middle dura fossa plate; posteriorly, the skeletonized sigmoid sinus and the entire posterior fossa dura plate; inferiorly, the sigmoid sinus, the deep mastoid cells, and the digastric crest (arrow). Anteriorly, the skeletonized facial nerve, incus, malleus, and intact ear canal are visible. Medially, the three semicircular canals are seen. Citelli’s triangle, the sinodural angle, Trautmann’s triangle, the position of the endolymphatic sac, and Donaldson’s line, are indicated
The Posterior Fossa Dural Plate
The posterior fossa dura plate is a large bony plate demarcated superiorly by the superior petrosal sinus, laterally and inferiorly by the sigmoid sinus, and medially by the posterior semicircular canal (Fig. 75). The posterior fossa dura plate forms the posterior wall of the antrum and the posterior wall of the petrosal part of the mastoid process. After locating and skeletonizing the sigmoid sinus, the posterior bony plate is the next structure encountered when drilling medially. It already appears before penetration of Körner’s septum and entry to the antrum (Figs. 62, 63, 70). It is recognized as a solid plate continuing towards the posterior semicircular canal. Most of the posterior fossa dura is included in Trautmann’s triangle, an imaginary triangle bounded by the tegmen mastoidei, superior petrosal sinus, sigmoid sinus, and the bony labyrinth. Inferior to Trautmann’s triangle and Donaldson’s line, the endolymphatic sac is seen, resembling a reflection of the posterior fossa dura (Fig. 75). The endolymphatic sac continues medially, ending in the endolymphatic duct, which lies within the vestibular aqueduct, a bony canal running posteromedial to the posterior semicircular canal and ending in the vestibule (Fig. 76).
The tip of the mastoid process in well-pneumatized ears usually contains large air cells. At the same depth as the facial nerve, there is the digastric crest (Fig. 75). On the external surface of the mastoid process, a corresponding depression occurs. This is the digastric fossa or mastoid incisura, relating to the attachment of the digastric muscle. Inferolateral to the sigmoid sinus and medial to the digastric ridge and the facial nerve, large air cells can be found (Fig. 75).
Facial Recess
The facial recess lies immediately lateral to the facial nerve at the external genu of the nerve (Fig. 75). It is usually a collection of small air cells (Fig. 72), continuing from the antrum towards the facial sinus, but there is no communication between these cells and the tympanic cavity. The facial recess is a surgical term. It is a triangle formed by the facial nerve medially, the chorda tympani laterally, and a bony buttress at the incudal fossa superiorly (Figs. 77, 78). Access to the tympanic cavity through the facial recess was used by Wullstein (1952, 1968) as “the middle ear inspection hole,” and was thoroughly elaborated later by Jansen (1962) in connection with the intact canal wall tympanoplasty technique (Jansen 1972). Jansen called this procedure posterior tympanotomy, and the name became very popular. The present author prefers to call Jansen’s posterior tympanotomy the posterior atticotympanotomy, partly because the procedure consists of drilling and opening via the facial recess from the posterior attic to the tympanic cavity, and partly because the term posterior tympanotomy— like the inferior, anterior, and superior tympanotomies—describes opening of the tympanic cavity from the ear canal by elevation of a tympanomeatal skin flap including the posterior fibrous annulus (Volume 1, pp. 79–86).
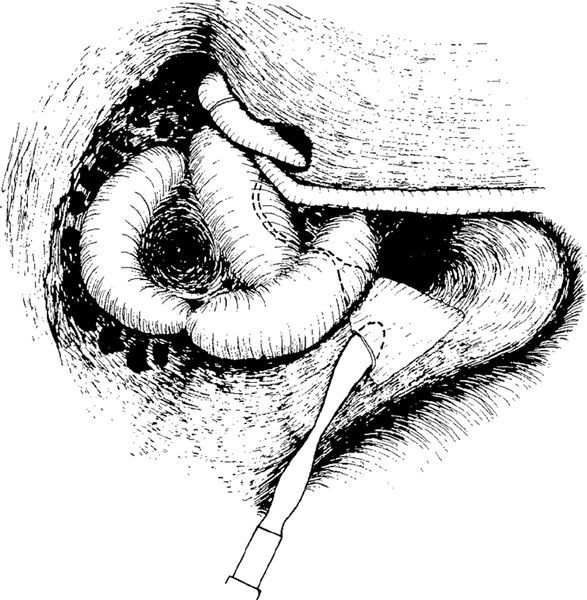
Fig. 76 Exposure of the endolymphatic sac, with decompression and opening. The course of the endolymphatic duct, posterior to the posterior semicircular canal toward the vestibule, is indicated by dashed lines
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


