Fig. 75.1
Current long-range OCT system
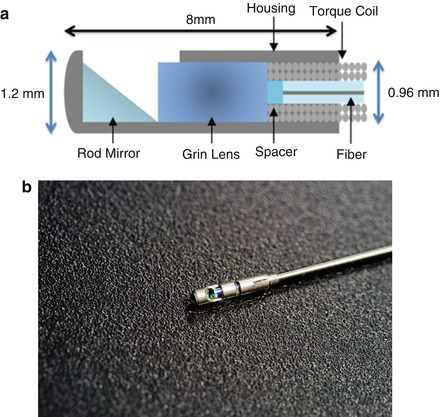
Fig. 75.2
Schematic (a) and picture (b) of LR-OCT probe
Fig. 75.3
Schematic of external rotational motor and probe
Acquired OCT data is processed using a modified algorithm [21]. An FFT is first performed to convert the signal into the frequency domain. Multiplication by the Heaviside function isolates the positive frequencies, and an inverse FFT is performed to obtain a complex time-domain signal. A demodulation step removes the carrier frequency from this term and compensates the dispersion cause by the acousto-optic modulator (AOM) by multiplying the negative phase values of a single A-scan obtained when the optical path length difference (OPD) of the reference arm with the AOM and sample arm is zero. The resulting remapped data is linearized in the K-domain via a recalibration step followed by a final FFT to recover the spatial information. Our OCT software package is written entirely in C++ and features a multithreaded design for data acquisition, image processing, and display that allows for maximizing computational throughput. The entire OCT algorithm is processed on a commercial graphical processing unit (GPU) using Nvidia’s CUDA package. This allows for frame-by-frame processing with a maximal frame rate of 25 frames per second for a given frame size of 2,000 A-lines.
75.3 Validation
The point spread function (PSF) versus imaging range graph (Fig. 75.4) was acquired by using a partial reflector at various distances and normalizing by the measured power. The system features a 6 dB sensitivity roll off at 12 mm total offset, which is in line with the expected imaging range give the removal of the mirror image.
Fig. 75.4
Sensitivity of the current LR-OCT system as a function of depth
In order to test the imaging capabilities of our system, a silicone airway was constructed. The airway was selected from a collection of adult CT scans devoid of pathology in the upper airway. The CT scan was loaded into commercial 3D rendering software, Amira, and a Standard Tessellation Language (stl) file was created for use as a model. Using rapid prototyping hardware, a phantom airway was molded in a green silicone matrix to ensure reflective properties compatible with the anatomical optical coherence tomography (aOCT) hardware (Fig. 75.4). The endoscopic LR-OCT probe and FEP sheath was introduced into the model airway in similar fashion to that of an actual research subject. A translucent model airway (Fig. 75.5), an exact copy of the green silicone phantom, was constructed to observe the pathway of probe and FEP sheath in the upper airway. A pullback scan of the phantom airway was performed. The resulting OCT data was compared against the original CT scan. As expected, the acquired OCT images are highly correlated with the original CT scan slices (Fig. 75.6).
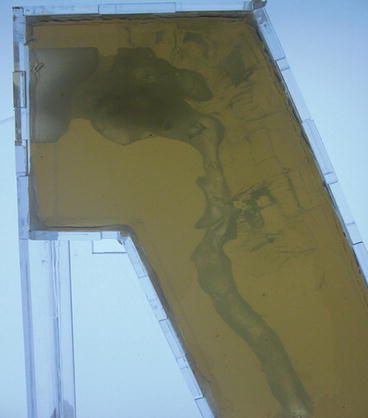
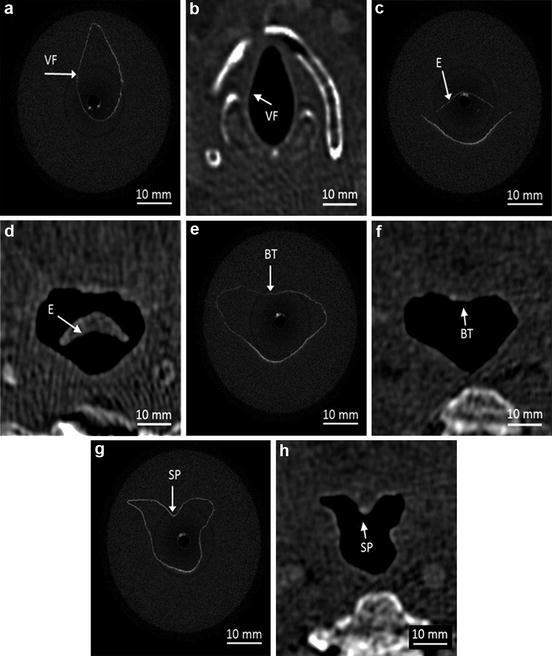
Fig. 75.5
Translucent model of normal phantom airway
Fig. 75.6
Comparison of OCT images (a, c, e, g) in model with normal CT scan (b, d, f, h). Vocal folds (VF), epiglottis (E), base of tongue (BT), and soft palate (SP)
75.4 In Vivo Human Studies
In vivo human adult imaging has been performed on adult and pediatric subjects. Patients’ upper airway was anesthetized using 4 % topical lidocaine administered bilaterally through the nostril; likewise the pharynx was anesthetized with an aerosolized benzocaine. Ten minutes was allowed to elapse in order for the anesthesia to take full effect. The subject was placed into the classical position for in-office fiber-optic endoscopy exam. The FEP sheath was inserted into the anesthetized nostril along the length of the upper airway to the level of the esophagus. FEP tubing was marked as it exited the nostril for repositioning in case movement of the pharynx shifted the probe out of position. The tubing was secured using paper tape attached to the bridge of the nose. The LR-OCT probe was then advanced down the FEP tubing until resistance was appreciated (signifying the probe has reached the end of the FEP tubing). Placement of the FEP tubing and probe was confirmed using a flexible laryngoscope introduced through the second nostril, after which the laryngoscope was removed. The LR-OCT probe was retracted through the airway at a rate of 0.5 cm per second over a distance ranging from 18 to 23 cm. Multiple sets of images were taken from each subject.
Examples of acquired OCT data are shown in Fig. 75.7. Each cross-sectional image is 43 × 43 mm. Anatomical structures such as the epiglottis (Fig. 75.7a), base of tongue (Fig. 75.7b) with associated tonsillar tissue, the soft palate and uvula (Fig. 75.7c), and adenoidal tissue (Fig. 75.7d) can be identified by their distinct tissue characteristics. Unlike OCT data acquired in phantom testing, up to 1.5 mm of tissue penetration was achieved and tissue substructure such as the elastic cartilage in the epiglottis can be seen.
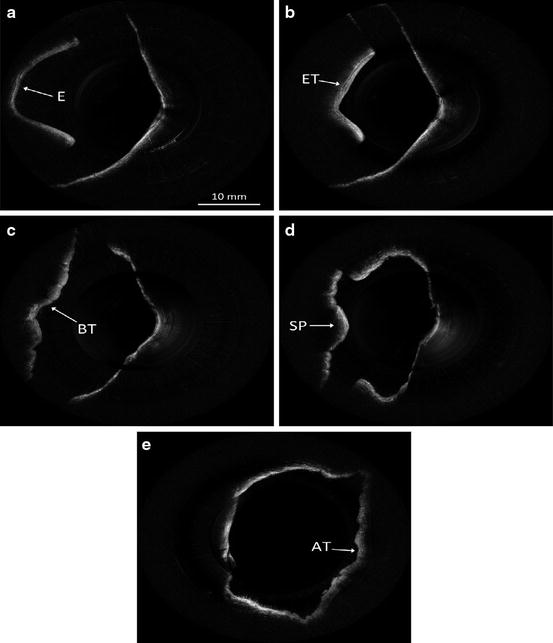
Fig. 75.7
Examples of in vivo LR-OCT images
75.5 Image Reconstruction/Rendering
OCT images are loaded into Mimics, a commercially available 3D rendering software. Anatomically, the airway contains many bends, the most exaggerated of which occurs around the area of the soft palate and continues onto the nasal passageways. However, OCT assumes the images are acquired in a linear fashion. Unlike CT or MRI, OCT axial slices deviate from one another in an absolute coordinate system in both X-Y-Z linear displacement and at least 1 angular degree of rotations freedom. Serial OCT images must be transformed to fit along a curved airway and aligned along the “common axis.” In order to fashion the linear LR-OCT data to represent the anatomical curve, a custom algorithm is used (Fig. 75.8). Using Cartesian coordinates from a series of CT scans acquired from normal patients. The database contains a variety of subjects, classified by age and sex. The acquired OCT data is matched to a CT scan that most closely correlates patient age and gender. The software creates a bend in sagittal slices of the OCT data creating an image that closely resembles the anatomic curvature. Figure 75.9 displays an example of data collection from a standard CT scan.
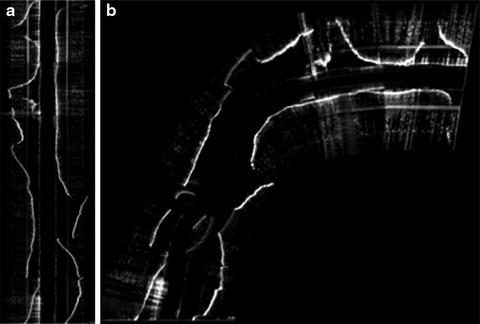
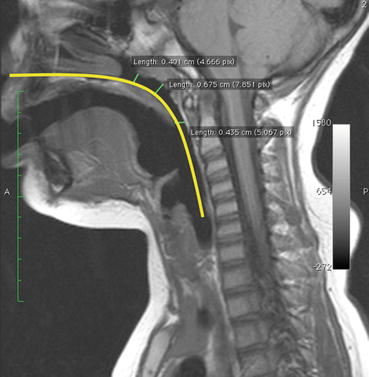
Fig 75.8
(a) Stacked LR-OCT data (sagittal view) as unprocessed linear data. (b) Stacked LR-OCT data (sagittal view) after applied bending algorithm
Fig. 75.9
Collection of Cartesian coordinates from normal CT scans for use in custom algorithm
The literature has described an OCT probe with integrated magnetic tracking which accurately locates the tip of the OCT probe within the lumen of the airway in 3D space (X, Y, Z coordinates). This configuration can provide patient-specific airway curvatures without the need for third-party software [22]. Commercial magnetic tracking systems are now available in a small form factor (0.56 mm). Integration with the existing LR-OCT probe has the limitation of increasing the OD of the probe, necessitating larger outer FEP sheaths, which may lead to increased patient discomfort. However, improvements in the technology may produce smaller tracking beacons that will add negligible bulk to the LR-OCT probe.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


