CHAPTER 19 Aesthetic Facial Analysis
These ideas were later revisited by the Renaissance artists, who began to define ideal proportions for the human form. This example is nowhere more evident than in the drawings of Leonardo da Vinci and his Vitruvian man (Fig. 19-1). It was da Vinci, who, through the study of anatomy, formulated ideal facial proportions and divided the profile into equal thirds (Fig. 19-2). Leonardo’s scientific accuracy rivaled that of Vesalius, whereas his artistic beauty remains unchallenged. Another Renaissance artist inspired by the Vitruvian notion of perfect proportions was the German printmaker Albrecht Durer. Durer used his own finger as a unit of measurement to construct a proportional system for the entire body, and in 1528 he published a four-book treatise on human proportions. Durer divided the facial profile into four equal parts and recognized that the length of the nose equals that of the ear.
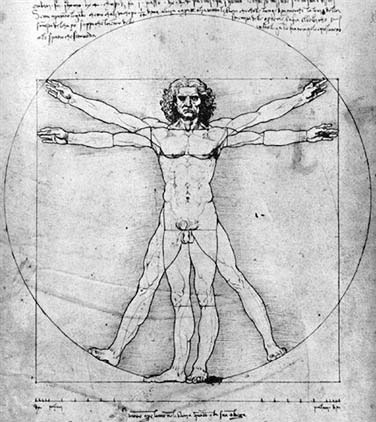
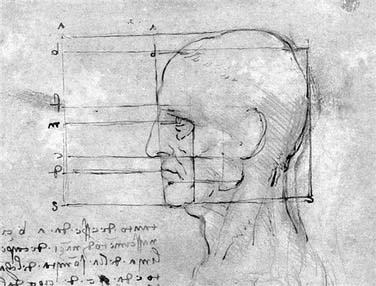
Figure 19-2. Leonardo da Vinci. The proportions of the head, ca.1490. Pen and ink over black chalk, 28.0 × 22.2 cm.
(Courtesy of the Galleria dell’ Academia, inv.236v, Venice.)
The artistic canons set forth in antiquity and during the Renaissance dominated Western art for centuries. In the twentieth century, anthropometrist Leslie Farkas and colleagues1 challenged the classic canons by measuring the facial proportions of 200 women, including 50 models. His results concluded that some of the canons are nothing more than artistic idealizations. Nevertheless, although social and cultural factors influence every generation’s concept of beauty, the aesthetic canons have withstood the test of time. Currently, the parameters established in the facial plastic surgery literature are based predominately on the works of Powell and Humphreys, who in 1984 crystallized this topic into a single text, Proportions of the Aesthetic Face.2
Anatomic Landmarks and Reference Points
Facial analysis is dependent on both soft tissue and skeletal anatomic landmarks. Soft tissue reference points are shown in Figure 19-3 and listed in Box 19-1. Skeletal reference points are defined by cephalometric analysis and are shown in Figure 19-4 and listed in Box 19-2.
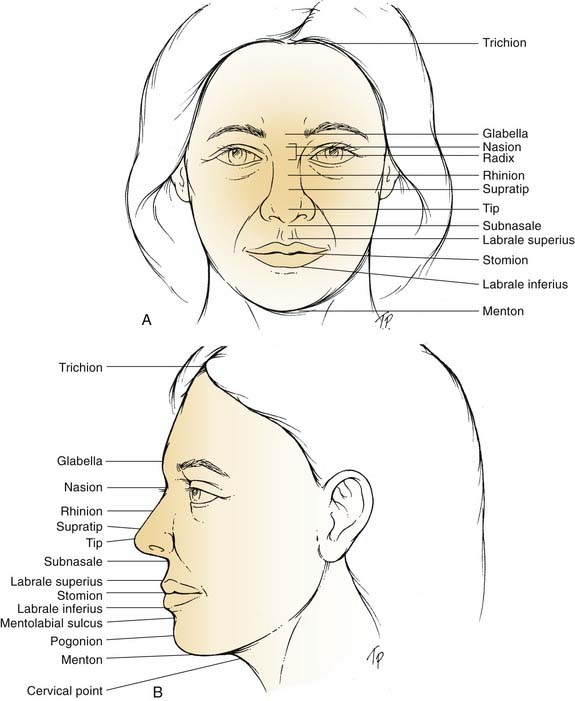
Box 19-1 Soft Tissue Anatomic Landmarks
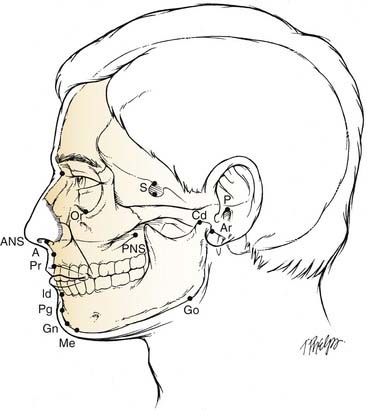
Box 19-2 Cephalometric Reference Points
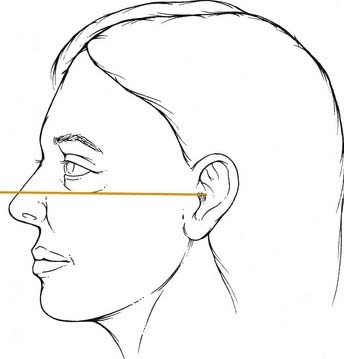
The Frankfort horizontal plane (Fig. 19-5) is the standard reference point for patient positioning in photographs and cephalometric radiographs. The Frankfort plane is defined as a line drawn from the superior aspect of the external auditory canal to the inferior border of the infraorbital rim while the patient’s gaze is parallel to the floor. A soft tissue definition for the inferior aspect of the infraorbital rim is the point of transition between lower eyelid and cheek skin.
Facial Proportions
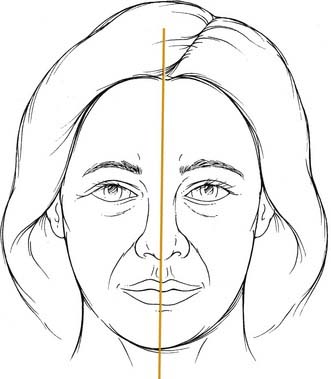
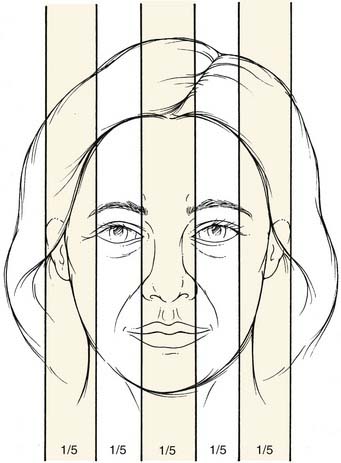
The initial assessment of the face evaluates symmetry. Symmetry is rarely perfect when comparing halves through a midsagittal plane (Fig. 19-6); nevertheless, midline points should lie on the axis line. Facial width is evaluated by dividing the face into equal fifths (Fig. 19-7). The width of one eye should equal one fifth of the total facial width, as well as the intercanthal distance or nasal base width.
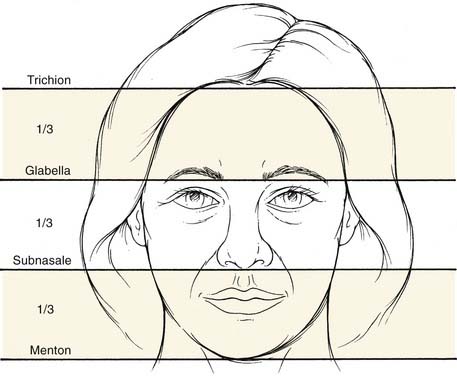
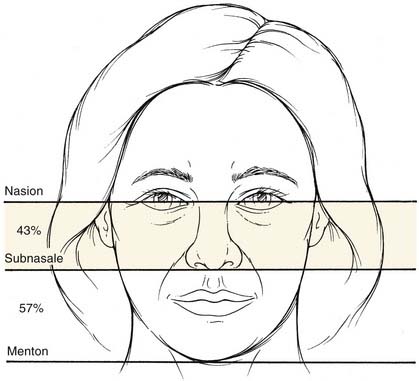
Facial height is commonly assessed by one of two methods. The first method divides the face into equal thirds (Fig. 19-8) as described by da Vinci. Measurements are made in the midline from the trichion to the glabella, from the glabella to the subnasale, and from the subnasale to the menton. The second method excludes the upper third of the face because of common variability regarding hairline position. Measurements are made from the nasion (as opposed to the glabella) to the subnasale and from the subnasale to the menton (Fig. 19-9). With this method the midface represents 43% of the height, with the lower face representing 57%.