CHAPTER 63 Acute and Chronic Laryngitis
Why Does Laryngitis Matter?
There are several broad reasons why laryngitis is significant. Functio laesa, the often overlooked “fifth sign” of inflammation (along with rubor, tumor, dolor, and calor), describes the loss of function in an inflamed organ, be it the liver in hepatitis or the hoarse voice of a patient with vocal fold edema related to viral laryngitis. The inflamed larynx does not phonate, swallow, or breathe well. In the extreme, this condition can lead to airway obstruction as seen in epiglottitis. Function may also be impaired after the resolution of the inflammatory process. In an important paper, Squire and associates1 demonstrated that the introduction of bacteria into an acquired airway injury in the rabbit model resulted in a higher rate of stenosis than seen in the controls; this effect was muted by the addition of antibiotics to the model. Fine degrees of dysfunction from bacterial infection have not been clearly described, however. In an innovative study, Reidy and colleagues2 exposed subjects to aerosolized antigens (to which they were known to have skin-test responsiveness). In this investigation, the subjects’ larynges did demonstrate greater mucus and other signs of irritation after exposure; their objective laryngeal parameters, such as acoustic voice parameters, did not change.
Finally, although it is not proven, many have suspected the relationship between laryngeal inflammation and malignant transformation. The most commonly considered mechanism is injury from refluxed materials. It was proposed many years ago by Ward and Hanson3 and has been further supported by the work of Koufman4 and Qadeer and associates.5–8
Acute Laryngitis
Phonotrauma
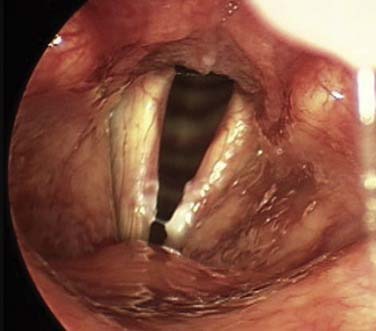
Vocal abuse, misuse, and overuse can contribute to phonotrauma. This may result in vocal fold hemorrhage and edema in addition to incurring changes at the molecular level.9,10 Although this process does not represent the usual concept of infectious or “exogenous” sources of inflammation, the tissue response to injury can be quite profound. The problem of vocal abuse and strain may be exacerbated by dehydration through its effect on phonation threshold pressure.11,12 On the basis of common clinical experience, many practitioners believe that vascular lesions of the vocal fold may begin or may be exacerbated by acute phonotrauma. In the case illustrated in Figure 63-1, a young singer noted the moment her voice changed during a performance. Examination of her vocal folds in the clinic revealed a left true vocal fold lesion with feeding vessels. Despite excellent hygiene, voice therapy, and conservative management, the lesion did not resolve, and she required phonosurgical intervention.

In the great majority of cases involving phonotrauma, medical attention is not sought. A patient who does seek care from an otolaryngologist is most likely to have recurrent or severe symptoms—or to be particularly sensitive to his or her vocal health. Clinical examination should include a detailed history and fiberoptic examination and stroboscopy, if available. There is little to no scientific basis for the usual treatments—voice rest, steroids, and other medications. Anecdotally, however, voice rest is quite useful to reduce further acute injury, particularly if there is a hemorrhagic component to the laryngeal injury. Paradoxically, some degree of mechanical strain (in the truest physics sense of the word) may be beneficial to appropriate vocal healing. Branski and colleagues13 have elegantly shown that low levels of mechanical activity may actually reduce inflammatory activity in vocal fold fibroblasts. This finding may be elucidated by further investigation as our understanding of the molecular basis of vocal fold injury improves.
Viral Laryngitis
The precise incidence of viral laryngitis is not known, reflecting its familiarity and its association with the ubiquitous viral “upper respiratory infection.” When it does occur, it may be due to typical “common cold” viruses, such as the rhinovirus. Many other viruses have been implicated in cases of acute viral laryngitis, including herpes zoster,14,15 coronavirus,16 as well as less familiar agents. There is no specific knowledge that antiviral treatments have any predictable impact on the clinical course of viral laryngitis. Supportive care, including rehydration and vocal rest, are commonly recommended. In one double-blind, placebo-controlled study, flurbiprofen, an anti-inflammatory medication, was shown to decrease discomfort in patients with viral laryngitis.17
In severe cases resulting in airway embarrassment, this aspect of clinical care naturally takes precedence. Medical management of the impaired and inflamed airway is familiar to readers from the airway chapters in this volume; it includes the use of steroids, antibiotics for secondary infections, proton pump inhibitors, and humidification. Although much of this approach has remained experiential and anecdotal, one prospective, double-blind, randomized study in children demonstrated better outcomes when dexamethasone was used in acute laryngotracheitis (croup) if given in the first 24 hours of treatment.18
Acute Bacterial Laryngitis
Much of this discussion, historically as well as in this edition, deservedly rests in the pediatric section. Epiglottitis—or, more properly, supraglottitis—continues to be a life-threatening infection of the upper airway in adults as well. Despite the great success of the Haemophilus influenzae B vaccine in limiting the frequency of this disorder,19 the clinical entity acute upper airway obstruction from bacterial infection of the larynx continues to occur. The presentation is often quite dramatic, with an urgent call to the emergency department for a drooling, febrile patient in respiratory distress. Depending on the acuity of the airway embarrassment, the adult patient may be examined fiberoptically to characterize the nature of the obstruction; determination of the severity of the obstruction and the clinical decision-making, however, are based on a generalized assessment of the patient’s overall appearance in addition to nonlaryngeal airway considerations, such as body habitus, jaw and mouth opening, and neck extension. If the patient requires airway intervention, intubation in a controlled setting (such as the operating room) or awake tracheotomy may be appropriate. This having been said, a review of 23 adult supraglottitis cases revealed that the minority (3/23) of cases required airway intervention.20 The remainder may be managed supportively, with humidification, intravenous antibiotics, close observation, and even with steroids.21
Laryngeal infection with Klebsiella rhinoscleromatis, part of the disorder known as rhinoscleroma, is another clinical entity that can affect the larynx. The disease may progress to airway obstruction with tracheal involvement but may be limited to rhinologic and vocal fold involvement. The disease is diagnosed from the identification of the causative organism, a gram-negative coccobacillus, within macrophages obtained from mucosal biopsy specimens. These are the characteristic Mikulicz cells of rhinoscleroma. The disease may be treated with fluoroquinolone antibiotics, tetracycline, and supportive airway management.22 Patients with this disease may also need acute as well as long-term surgical airway management; Amoils and Shindo23 reported on a series of 22 patients with rhinoscleroma, 13 of whom had laryngeal involvement.23 Of these 13, 3 had undergone tracheotomy at some point during the clinical course.
Acute Fungal Laryngitis
Candidal laryngitis is probably quite common, although its recognition as a clinical entity has increased. Sulica24 provided a succinct review of this disorder in 2005. Patients typically present with hoarseness with or without accompanying throat discomfort. The most characteristic finding is a diffuse, whitish speckling of the vocal folds or supraglottis (Fig. 63-2); this can be quite similar to that seen in thrush affecting the oral cavity and soft palate. Perhaps the most important lesson in the clinical recognition of laryngeal candidiasis is for the physician to suspect its presence in both immunocompromised and immunocompetent individuals. There are very few causes of white lesions on the surface of the vocal fold epithelium; the differential diagnosis includes hyperkeratosis/leukoplakia, malignancy, thick mucus, and candidal infection. Although formal culture is required to confirm the diagnosis, it is neither practical nor common. It has been theorized that patients with local risk factors, such as the recent use of broad-spectrum antibiotics or topical (inhaled) corticosteroids, are more prone to development of this problem. This theory is clinically reasonable but such an association is not exclusively the case; Candida should be included in the differential diagnosis of a great range of patients with epithelial abnormalities of the larynx.25
Candida may also become invasive with fulminant inflammation and erosion. This development requires aggressive medical treatment, including consideration for parenteral antifungal medication and airway support.22
Chronic Laryngitis
Bacterial Laryngitis
Although most otolaryngologists associate bacterial infection of the larynx with an acute process, chronic, even life-threatening disease may arise in this situation. Superinfection of the larynx may complicate intubation injuries or larynges already damaged from relapsing polychondritis, for example. Eliashar and colleagues presented several case examples of this occurrence.26 In each of the three cases outlined, purulent chondritis was noted in patients with prolonged (longer than 1 month) of hoarseness and stridor. These patients required surgical drainage and ongoing medical treatment. In two of the three cases, the pathogen was Staphylococcus aureus. Clinicians should suspect bacterial infection, regardless of its relative rarity, in patients who have persistent chronic inflammation of the larynx. Culture and drainage of abscess spaces may be required. The role of hyperbaric oxygen is not widely agreed upon for this disorder or even for chondroradionecrosis of the larynx, which is discussed elsewhere in this volume.
Fungal Laryngitis
The larynx may also become infected with pathogenic fungal species. The organisms include Blastomyces, Histoplasma, Coccidioides, Paracoccidioides, and Cryptococcus spp. In general, the clinical presentation of laryngeal fungal infection is not specific to the pathogen, but reflects general disturbance of laryngeal function—that is, consists of hoarseness and throat discomfort. Tissue biopsy and fungal stains are needed to confirm the diagnosis. The less common pathogens are not discussed in detail, although laryngeal infection with Sporothrix,27 Aspergillus,26,28 and Cryptococcus spp.29,
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


