(62.1)
where k d, k i, and k a are the wave vectors of the diffracted light beam, incident light beam, and acoustic wave, respectively. The frequency of the diffracted light beam νd is shifted from the frequency of the incident beam νi by an amount equal to the frequency of the acoustic wave νa. Depending on the relative orientation of incident light beam and acoustic wave, this frequency shift is upward or downward:

(62.2)
To enable heterodyne detection in an OCT instrument, the frequencies of reference and sample beams have to differ. The amount of this frequency difference is the carrier frequency. This is the frequency that is detected by a photodetector in the detection arm of the low-coherence interferometer in case of path length matching of the two arms.
In the original time domain A-scan-based systems, the frequency of the reference beam is automatically shifted as a result of the Doppler shift caused by the moving reference mirror. In our TS-OCT system, the frequency shift is generated by one or two AOMs placed in the reference arm (placement of the AOMs in the sample arm would also work in principle). If only one AOM is used, the carrier frequency is equal to the acoustic frequency νa (or 2νa if the AOM is passed twice). Since νa is usually several tens of MHz, the carrier frequency is rather high in this case. On the one hand, this enables very high scanning speeds; however, it requires high-speed detectors and amplifiers which usually have a poorer signal-to-noise ratio (SNR) than slower detectors/amplifiers. For this reason, frequently two AOMs are used. They are operated at slightly different frequencies ν1a and νa2. One AOM is oriented to upshift the light frequency and the other to downshift the frequency, so that the net frequency shift (and the net carrier frequency) is much lower, on the order of a few 100 kHz to a few MHz, thus enabling the use of slower low-noise detectors/amplifiers.
62.3 Interferometer Setups of SLO/OCT and Dynamic Focusing
In principle different interferometer configurations can be used for AOM-based en face OCT: Michelson and Mach–Zehnder interferometers. However, we discuss the operating principle of such an instrument with reference to a Mach–Zehnder interferometer scheme. This design [13] (c.f. Fig. 62.1) enables balanced detection and incorporates the simultaneous recording of a scanning laser ophthalmoscope (SLO) channel.
Fig. 62.1
Sketch of AOM-based Mach–Zehnder interferometer for retinal imaging. AMP amplifier, AOM acousto-optic modulator, BS beam splitter, Det single-mode fiber pigtailed detector, L1 and L2 lenses, SLD superluminescent diode, SLO-Det scanning laser ophthalmoscope detector (single-mode fiber pigtailed) (Reproduced from Pircher et al. [13] by permission of the Optical Society of America)
A low coherent light source emits a beam of short coherence length, centered at optical frequency ν0. This beam illuminates the interferometer where it is split by BS1 into two components: a reference beam and a sample beam. The reference beam traverses two AOMs with different frequency shifts (ν1 and ν2, resulting in a net light frequency shift of Δν). The angular spreads of the frequency-shifted beams caused by the two oppositely oriented AOMs cancel each other largely. This allows the use of very broadband light sources, thus enabling ultrahigh-resolution TS-OCT [9, 14]. After traversing the AOMs, the beam is reflected at two reference mirrors that are mounted on a translation stage. These act as a variable path delay unit (PDU) that is used to vary the length of the reference path between successive en face scans, thus changing the position of the coherence gate within the sample (in this case the retina). The beam is recombined with the sample beam at the beam splitter that is located at the interferometer exit (BS3). The sample beam traverses another beam splitter (BS2) and is directed to an x–y scanning unit. The telescope located after the scanning unit images the pivot point of the scanners onto the pupil plane of the eye. The last lens of the telescope is mounted on a translation stage that can be simultaneously moved with the change of the coherence gate, thus enabling a simultaneous shift of the focal position with the coherence gate [11]. The light is backscattered from the retina and split into two parts at the beam splitter BS2. One part is directed to the interferometer entrance where it is partly reflected by BS1 and is coupled into a single-mode fiber. This light is detected by an avalanche photodiode. Although it records part of the light backscattered from the sample, this light is not brought to interference with the reference beam. Therefore, this detector records a simple intensity image from the retina without coherence gating similar to a commonly used SLO [15, 16] detector. As will be discussed later on, this additional signal is essential for alignment, focusing, and post-processing purposes.
The other light part exiting BS2 is directed to the beam splitter at the interferometer exit (BS3) where it is recombined with the reference arm. Light from both exits is coupled into single-mode fibers and is detected by a dual balanced detector. The light-induced electrical signals from both interferometer exits are phase shifted by 180° between each other which enable the dual balanced detection by simply subtracting the two recorded signals before amplification. This procedure reduces source noise and excess noise [17]. In order to allow a pixel to pixel correspondence between SLO and OCT channels, the two OCT detectors have to be confocal to the SLO detector, and the signals are recorded simultaneously using the same data acquisition board.
Subject aligning and data recording are done in the following way. First, the focus is adjusted by moving the last lens and using the information of the SLO channel. Then the PDU is set to place the coherence gate to the location of the cone photoreceptors (junction between inner and outer segments of cones), a location that provides high backscattering signal. Shortly before starting the 3D data recording, the coherence gate and the focus are set deeper into the tissue (within the choroid). The x–y scanner scans the complete x–y plane corresponding to the depth position of the coherence gate (the layer thus scanned is the so-called coherence layer; its thickness is equal to the coherence length). If the sample beam hits a backreflecting or backscattering site within the coherence layer, the backscattered light will interfere with the reference beam. Since sample and reference beams differ in frequency by an amount Δν, the resulting interference signal will oscillate at Δν (the beat frequency). Δν constitutes a very stable carrier frequency that can easily be extracted by filtering with a band pass filter centered at Δν. The magnitude of the signal thus extracted is a measure of reflectivity of the sample as a function of the transversal position at the depth defined by the PDU. The signal magnitude is encoded on a grayscale. The signal from the SLO channel is recorded in parallel. However, the depth resolution of this channel is determined by the numerical aperture and the resulting depth of focus. After one en face scan, the PDU and focus settings are changed to move the coherence layer closer to the surface of the sample, and another en face scan is recorded. Step by step, the coherence layer is shifted through the sample. In this way, a 3D data set of a selected region of the sample is recorded. Figure 62.2 illustrates the transversal scanning scheme, as compared to the conventional, A-scan-based scheme, for the case of retinal imaging.
Fig. 62.2
Comparison of conventional longitudinal scan pattern (left) and transversal scan pattern (right)
62.4 Axial Eye Tracking and Transverse Motion Correction
Imaging the retina in vivo at high magnifications is challenging because of permanent eye motion. This motion will be present in all three dimensions. In FD-OCT axial eye motion is regarded as a minor problem because of the high axial imaging speed. Although axial motion is present in B-scans and in 3D volumes, these artifacts can largely be corrected in post-processing by, e.g., using correlation techniques between different B-scans. On the other hand, transverse motion artifacts can be a limiting factor. To overcome this, either hardware-based transverse eye tracking (2D) [18] has to be implemented or the transverse extension of the imaged volume has to be significantly reduced [19]. The scanning priority in TS-OCT is different; therefore, transverse eye motion can be corrected similar to high-resolution SLO systems in post-processing [20]. Axial eye motion, however, is a limiting factor for 3D measurements and has therefore to be corrected.
Our group introduced a concept for axial eye tracking that is based on an accurate measurement of the corneal apex position. The depth position of the cornea is then used to adapt accordingly the length of the reference arm of the TS-OCT instrument [21]. A sketch of an improved instrument is shown in Fig. 62.3 [22]. The system consists of several parts: the TS-OCT part, a separate FD low-coherence interferometer (LCI) for measuring the corneal apex position, and a part for changing very rapidly the length of the reference arm. The TS-OCT setup is similar to the scheme presented in Fig. 62.1. However, in order to improve the light efficiency within the instrument, additional polarization-sensitive components have been implemented. For details, refer to reference [22]. The LCI is based on a 90:10 fiber splitter and is operated at 1,300 nm with a bandwidth of 55 nm resulting in a depth resolution of ∼14 μm. Only 10 % of the light is directed to the sample arm. Via a dichroic mirror, the sample beam is coupled into the sample beam of the TS instrument and is directed to the eye. A collimated beam incident on the cornea is used which is essential in order to minimize influences of transverse motion on the measured apex position [23]. Moreover, only the corneal reflex is detected (no internal structure), resulting in a single OCT signal. Even though the depth resolution of the LCI is moderate, the peak position of the OCT signal can be determined very accurately. Light that is backscattered from the cornea is brought to interference with the light from the reference arm and is detected with a spectrometer. The spectrometer consists of a reflective diffraction grating and an InGaAs line scan camera that can be operated with up to 7 kHz.
Fig. 62.3
Scheme of a TS-OCT instrument with implemented high-speed axial eye motion correction. RSOD rapid scanning optical delay line, SD-LCI spectral domain low coherence interferometer, LS light source, P polarizer, DC dispersion compensation glass rods, BS beam splitter, L1–L4 lenses (L1 f = 50 mm, L2 f = 20 mm, L3 f = 40 mm, L4 f = 80 mm), AOM acousto-optic modulator, TS translation stage, PBS polarizing beam splitter, DM dichroic mirror, RM reference mirror, DG diffraction grating, Pe Pellicle, GS galvo scanner, x–y scanning unit consists of a resonant scanner and a galvo scanner (Imaging optics between the two scanning mirrors are omitted for clarity) (Reproduced from Pircher et al. [22] by permission of the Optical Society of America)
While the measurement of the corneal position can be done very fast, the corresponding adaption of the reference arm length can be a limiting factor because of the inertia of the optical components. Even if a high-speed translation stage is used, residual axial eye motion remains [21]. In order to improve the adaption speed, we implemented a technology that is well known from the pre-FD-OCT area: the rapid scanning optical delay line (RSOD) [24]. The RSOD which is placed into the reference arm of the TS-OCT interferometer (c.f. Fig. 62.3) consists of a diffraction grating, a lens, and a galvanometer scanner. The pivot point of the scanner is adjusted in order to change the group delay only (no additional phase delay is introduced). The improved axial eye motion correction speed ensures that residual correction errors are well below the depth resolution of the system. The tracking system is based on measurement of the corneal position. Hence, it cannot distinguish between axial eye motion and axial eye length changes caused by, e.g., fundus pulsation. However, these length changes are in the order of a few microns [25] and can therefore be neglected.
Using the information from the SLO channel, transverse motion correction can be done in post-processing similar to SLO instruments. For this purpose the cross correlation between each recorded SLO frame with a reference frame (chosen by the user) is calculated, and the frame is shifted according to the displacement from the position of the reference frame. All frames are averaged to produce a new reference frame that should be free of in-frame distortions (provided that the number of averaged frames is sufficiently large). The previous step is repeated using this new reference frame and applying the transformation matrix to the OCT images. Together with axial eye tracking, this procedure allows the recording of 3D volumes of the retina with negligible eye motion artifacts [22]. While the abovementioned procedure is sufficient for imaging without AO assistance, the implementation of AO requires an additional step. In a final step, each frame is divided into several subframes consisting of a certain number of transverse lines. The cross correlation is then performed between each subframe and a reference frame resulting in an improved transverse motion correction, because this procedure partly compensates for in-frame distortions [20].
62.5 High-Resolution Imaging of the Human Retina
It is known from histology that the photoreceptors in the human eye (rods and cones) are arranged in a very regular way resulting in a mosaic pattern [26]. In the fovea, the spot of best vision (in the healthy eye), the cone density and the regularity are highest. The density decreases exponentially with increasing eccentricity from the fovea. While there are no rods present in the fovea, the rod density reaches a maximum at around 12–20° eccentricity from the fovea.
One of the major challenges in retinal imaging using OCT in the past decade was the visualization of the cone mosaic. Using other imaging technologies, it was demonstrated quite early that in healthy eyes with good optics, the correction of low-order aberrations (e.g., defocus and astigmatism) can be sufficient in order to resolve cones in the periphery of the fovea [27]. Unfortunately, the field of view of these initial instruments was limited to a very small patch on the retina. An augmentation of cone visualization capabilities and extending the field of view were achieved with the introduction of adaptive optics (AO) [28–35]. AO corrects a variety of aberrations even of higher orders. Hence, the cone mosaic could be successfully imaged using AO-equipped imaging technologies as flood illumination fundus cameras [36] and SLO [37]. However, the depth resolution of these imaging techniques is rather limited and prevents the visualization of different interfaces of cone photoreceptors. OCT provides the necessary depth resolution, but its transversal resolution in the retina is commonly restricted by low NA to ∼20 μm which is not sufficient to resolve individual cones. The low NA is a compromise between transverse resolution and depth of focus, thus maintaining the transverse resolution over the entire imaging depth (i.e., the retinal thickness).
The first attempt to improve the transverse resolution by combining adaptive optics with OCT has been made in 2003 by the group of D. T. Miller at Indiana University [38]. The approach used full field OCT but faced sensitivity issues when applied in vivo. Later work used AO in an A-scan-based OCT system; however, visualization of individual cones could not be demonstrated with these initial setups [39, 40]. It took another year until transversal structures of a spacing similar to that of photoreceptors could be shown in OCT B-scans using AO-OCT by two different groups [41, 42]. However, both instruments had rather slow 3D imaging capabilities, preventing motion artifact-free 2D imaging of the cone mosaic in the en face imaging plane.
Our group picked up the initial abovementioned idea of cone imaging without using AO assistance. Because TS-OCT has the same scanning protocol as SLO, this technique is ideally suited for recording (nearly) motion artifact-free en face images of the retinal structure. We used the setup shown in Fig. 62.1 for this purpose and demonstrated cone mosaic imaging (in the en face plane) with OCT for the first time [13].
The system employed a moderately wide sampling beam of ∼4 mm diameter, enabling transverse resolutions sufficient to resolve the somewhat wider cone spacing at the periphery of the fovea but small enough to avoid excessive ocular aberrations and therefore (in the healthy eye) the necessity of adaptive optics. In addition the standard detection configuration in OCT is already confocal because it is based on using single-mode fibers [43]. The additional confocal SLO detector (also single-mode fiber coupled) operates in parallel to the OCT channel and provides an essential tool for correct subject and focus alignment. After the implementation of faster camera technology or fast swept source OCT technology, the simple concept of moderate sample beam diameter (and confocal arrangement) for cone photoreceptor imaging has been successfully translated to FD-OCT instruments [44–46].
Axial motion artifacts, however, limited the performance of our initial instrument to 2-dimensional imaging (B-scans or C-scans). Full 3D imaging capability was achieved by the implementation of an axial eye tracker [21, 22]. Figure 62.4 shows example images recorded in a healthy subject with a TS-OCT instrument that is equipped with an axial tracker. Figure 62.4a shows a B-scan retrieved from 3D data which demonstrates the capabilities of the axial tracker and the dynamic focus. The images were recorded at ∼4° eccentricity from the fovea and cover a volume of 1° (x) × 1° (y) × 500 μm (z). Note that despite the high transverse resolution, the entire depth is imaged sharply which could up to now not be achieved in the retina using FD-OCT. Similar to standard OCT, four distinct posterior layers can be observed. However, there is still some controversy on the labeling of these layers. We strongly favor the following association and provide different evidences for this labeling later on: (1) external limiting membrane (ELM), (2) boundary between inner and outer segments of photoreceptors (IS/OS), (3) end tips of photoreceptors (ETPR), and (4) retinal pigment epithelium (RPE). As can be observed in Fig. 62.4b, d, two layers, the IS/OS and ETPR, show a similar cone mosaic pattern as is known from SLO imaging. The appearance in both layers can be explained by the wave guiding properties of the cones [47]. The outermost layer does not show the cone mosaic and appears in general more diffuse than the previous two layers. Using polarization-sensitive OCT, a polarization scrambling was observed from this layer [8, 48, 49]. Data from patients and in vitro measurements showed that melanin is one cause for the polarization scrambling and that the layer can hence be associated with the RPE [50–52].
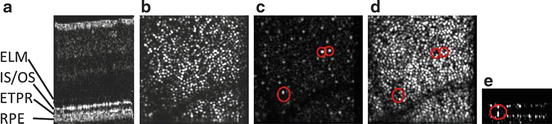
Fig. 62.4
TS-OCT images retrieved from a 3D volume. (a) Exemplary overview B-scan, (b) junction between inner and outer segments of photoreceptors, (c) within cone outer segments (locations of BRS that show no signal within the ETPR are marked with a red circle), (d) ETPR layer, (e) exemplary B-scan located at the position of the lower left red circle in (c) and (d) (Reproduced from Pircher et al. [22] by permission of the Optical Society of America)
Interestingly, as is shown in Fig. 62.4c, e, bright reflecting spots (BRSs) within the outer segments of the cones can be observed at some transverse locations. Defects within the cone outer segments could be one possible explanation for these signals. Using a Fourier analysis of the cone mosaic yields Yellott’s rings [53], and the radius of each ring is a direct measure of the row to row spacing of the cones. This spacing can be translated into cone density. Figure 62.5a shows the cone density measured at different eccentricities from the fovea for five subjects. The measured densities are in good agreement with values known from histology and show that for four out of five healthy subjects, the cone mosaic could be resolved down to ∼2° eccentricity from the fovea without the use of adaptive optics. In addition we measured the density of the BRS which shows some kind of maximum at 3–4° eccentricity from the fovea (c.f. Fig. 62.5b).
Fig. 62.5




(a) Measured cone density of five volunteers at different eccentricities from the fovea (black line: data from Ref [26]). (b) Measured bright reflections (BR) within the cone outer segments at different eccentricities (each color corresponds to a different subject) (Reproduced from Pircher et al. [22] by permission of the Optical Society of America)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
