Acanthamoeba Keratitis
Richard L. Abbott
Colleen P. Halfpenny
Michael Zegans
Troy R. Elander
Acanthamoeba is a ubiquitous, free-living protozoon that causes a serious and troublesome keratitis. At greatest risk are contact lens wearers who use nonsterile solutions in their lens care regimen. Because useful vision can be lost as a result of this infection, an increased awareness of clinical and laboratory signs is essential. Earlier suspicion and diagnosis may improve the medical and surgical outcome of this potentially devastating disease.
Etiology
Acanthamoeba organisms are small and resilient, with a wide distribution in the environment.1,2 The protozoan’s life cycle is characterized by a transformation from active trophozoite to dormant cyst. The irregularly shaped trophozoite, which is 15 to 45 μm in diameter, is slowly motile (Fig. 18A.1). The cyst is 10 to 25 μm long and has a thick double-walled external structure consisting of an outer wrinkled ectocyst and inner polygonal endocyst (Fig. 18A.2).3,4 Transformation from the trophozoite to the cyst stage enhances survival in unfavorable circumstances, which include wide temperature ranges, desiccation, food depletion, pH changes, low oxygen concentration, and cell crowding.5
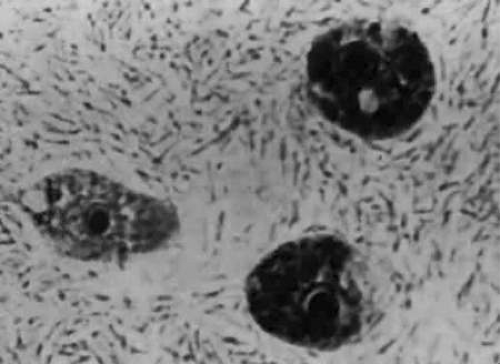 Figure 18A.1 Acanthamoeba trophozoite. |
 Figure 18A.2 Characteristic polygonal Acanthamoeba cyst. |
Of all free-living amebas, only two genera are pathogenic in humans: Acanthamoeba and Naegleria.1,6,7 Naegleria is rapidly fatal in young healthy adults, usually from granulomatous meningoencephalitis.8 Currently, no ocular disease from Naegleria has been reported. Acanthamoeba can cause both ocular and nonocular disease.9,10 In rare and experimental circumstances, Acanthamoeba has caused ocular disease other than keratitis, including uveitis, optic neuritis, and chorioretinitis.11,12,13
Incidence
Acanthamoeba keratitis was first described by Jones in 1973.14 Since then, the reported cases in the United States have steadily increased to more than 200, although the exact incidence is unknown. From 1973 to 1981, reported cases averaged 1 per year. From 1981 to 1984, cases gradually increased, with a dramatic rise occurring from 1985 to 1987.15 Possible factors responsible for this surge include heightened familiarity with the disease among ophthalmologists, the discovery of cases previously missed in keratoplasty specimens,16 and a truly increased incidence. This greater incidence may represent an increase in prevalence, virulent strains, or contact lens wear.4 Since the late 1980s, there have been conflicting reports regarding whether the incidence of Acanthamoeba keratitis is increasing or decreasing.17 However, the prognosis with medical treatment does seem to be improving.18,19
The Centers for Disease Control found no gender predilection for Acanthamoeba keratitis. The age range was from 13 to 82 years, with a medium of 29.15 Most cases of Acanthamoeba keratitis have occurred in warmer climates during the summer months.20 In addition to the United States, cases have been reported in Europe, Africa, Asia, and Australia.17 It is expected that there is approximately 1 case per 30,000 hydrogel contact lens wearers per year (0.33 per 10,000) in England, Europe, and Hong Kong. A higher reported rate in Scotland in 1996–1997 can be attributed to the use of lens disinfection with chlorine tablets dissolved in tap water.21
More than 22 species of Acanthamoeba have been isolated. Those causing keratitis, in decreasing frequency, are Acanthamoeba castellanii, Acanthamoeba polyphaga, Acanthamoeba rhysodes, Acanthamoeba culbertsoni, and Acanthamoeba hatchetti. In 20% of cases, multiple species are isolated.20 So far, only four genotypes have been associated with keratitis, of which the majority has been T4, but T3, T6, and T11 have each caused individual cases.22
There are three major risk factors for developing Acanthamoeba keratitis: contact lens wear, exposure to contaminated water, and corneal trauma. Among younger patients, contact lens wear is the major predisposing condition.15
Infection in Contact Lens Wearers
The first association between contact lenses and Acanthamoeba keratitis was made in 1984.23 Initially, the major recognized risk was from daily soft lens wear in contaminated water environments such as hot tubs, swimming pools, and lakes.2 Next, the important association with homemade saline became apparent. Subsequently, the list of involved lenses expanded to include extended-wear, polymethylmethacrylate, gas-permeable, combined hard/soft, and disposable lenses.24,25,26 There is in vitro evidence that trophozoites have a higher affinity for the first-generation extended-wear silicone-hydrogel lenses as compared with conventional hydrogel lenses, and therefore, these patients may be at the highest risk of infection.21,27 Conversely, it is estimated that the incidence in rigid contact lens wearers is 9.5 times lower than that in soft or hydrogel users.22 There have also been an increasing number of reports of Acanthamoeba infection in overnight orthokeratology.28
Contact lenses may predispose for infection because of epithelial breaks from lens deposits, prolonged wearing schedules, or improper lens handling. In addition, micro-organisms may adhere to the lenses or reside in the lens care system.4,23
One study showed an alarmingly high percentage of asymptomatic contact lens wearers with contaminated lens care systems.29 Because Acanthamoeba organisms use bacteria and fungi as food sources, this contamination would appear to predispose for Acanthamoeba keratitis. A related study examined the lens care systems of known patients infected with Acanthamoeba and clearly established an association with bacteria, fungi, homemade saline, and improperly used nonpreserved saline.30
Several investigators have examined the efficacy of contact lens disinfecting systems against Acanthamoeba.31,32,33,34 In general, heat disinfection is more effective than chemical disinfection in killing trophozoites and cysts.31,32 Cleaning solutions vary in effectiveness with respect to concentration, exposure time, and Acanthamoeba species.32,33,34 Recommended treatment for low-water-content contact lenses is thermal disinfection. For other lenses, chemical disinfection with either commercial preserved or nonpreserved solutions is encouraged. Nonpreserved saline should be discarded weekly, used in small quantities, and kept refrigerated.25 The use of homemade saline with distilled water and salt tablets should be discontinued. Infrequent lens disinfection, tap water rinses, and overuse of commercial solutions increase the risk of Acanthamoeba keratitis.29
Clinical Features
The clinical features of Acanthamoeba keratitis can be easily confused with those of other corneal infections. Numerous reports have detailed the vast array of signs and symptoms that occur with this entity, and attempts have been made to elucidate its most common presenting features.35,36,37,38,39 Through recognition of these findings, as well as understanding its chronic clinical course, improved diagnostic accuracy may be achieved by the clinician.
Symptoms
With the onset of the disease process, patients may complain of blurred vision, photophobia, tearing, blepharospasm, and foreign body sensation. Severe ocular pain is consistently reported by patients and often seems out of proportion to the keratitis and degree of inflammation present.36,37,39,40,41,42 Symptoms tend to wax and wane, depending on the rapidity of onset and severity of the chronic keratitis and the anterior chamber inflammatory reaction.
Signs
The corneal epithelium may show a variety of changes in early Acanthamoeba keratitis before stromal involvement.35 These findings, although nonspecific, must be recognized as part of the clinical picture. They may represent early epithelial infection prior to stromal invasion and are summarized in Table 18A.1.
TABLE 18A.1 Epithelial Changes in Acanthamoeba Keratitis | |
|---|---|
|
Persistent epithelial erosions occur in the vast majority of cases. Occasionally, these epithelial erosions begin as coarsely elevated, dendritiform lines that break down early, which may explain why a great majority of patients undergo treatment for herpes simplex.39 Histopathological examination and cultures taken from these lesions have been reported positive for Acanthamoeba.35
After some form of epithelial involvement, stromal infiltration develops, usually in the central or paracentral cornea. Initially, its appearance is not characteristic and involves the anterior stroma as a serpiginous, gray-white infiltrate with an overlying epithelial defect (Fig. 18A.3). Small satellite lesions and edema may develop around the main infiltrate. As the infection progresses, the infiltrate becomes most dense at its peripheral aspects, forming the characteristic annular infiltrate (Fig. 18A.4). This ring is considered the hallmark of Acanthamoeba keratitis; however, it usually occurs only in more advanced cases.3,16,35,39,42 It may be segmental or circumferential, with stromal thinning or furrowing and a variable overlying epithelial defect.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


