20
Abnormalities of the Mucosal Wave
No characteristic of laryngeal imaging is more dependent on the unique capacity of videostroboscopy than the mucosal wave evaluation. Still images, or even recorded normal light fiberoptic examinations, cannot provide the data necessary to evaluate the mucosal wave. The use of stroboscopic light or high-speed image capture (such as high-speed video or videokymography) is needed to evaluate this parameter.
One important limitation of videostroboscopic examinations should be mentioned here. Because videostroboscopy requires a periodic voice to trigger a stroboscopic light source, videostroboscopy is not always capable of recording the mucosal wave information in all patients. Furthermore, severely dysphonic voices, significant pitch breaks, glottal insufficiencies, and large mass effects can make visualization of a mucosal wave with videostroboscopy difficult or even impossible.
High-speed imaging systems eliminate the need for a periodic voice by capturing real-time images but come with their own constraints (Fig. 20.1).1 The high cost of videostroboscopic systems often limits their availability, but the even higher cost of high-speed imaging systems makes their availability more rare. In addition, the large quantity of data that highspeed systems record, for which discrete clinical protocols do not exist, makes the routine use of these imaging systems uncommon.
Videokymography is another alternative for imaging vocal fold vibration in patients with nonperiodic voicing. Widely viewed as a more economical way to achieve real-time images, it can record, in real time, a single selected line across the vocal folds, providing an opportunity to look at the mucosal wave form produced at that point of the vocal fold margin (Fig. 20.2). Looking at several points on the vocal fold edge or at the site of a lesion requires several evaluation passes. Videokymography is considered to be more capable of identifying subtle differences in the mucosal waveform from side to side, and its use should be considered in complicated diagnostic situations.2
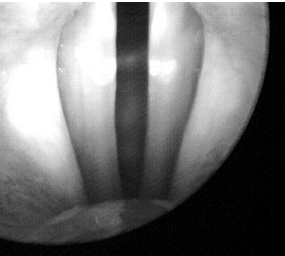
Fig. 20.1 A high-speed video image.
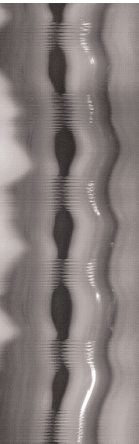
Fig. 20.2 A videokymography image.
It is important to remember that the image of a mucosal wave on the screen is a two-dimensional representation of the three-dimensional movement of the vocal fold mucosa and the superficial lamina propria over the deeper vocal fold structures. As such, the mucosal wave is the best vocal fold vibratory parameter for providing information about the state of the histologic layers of the vocal fold and the disorders affecting them. It can be impacted, however, by other components of the vibratory system, in addition to the state of the superficial vocal fold tissue. The degree of tension present in the entire laryngeal system affects the mucosal wave, with increasing tension often, but not always, decreasing vibration. In addition, because vocal fold vibration and mucosal wave are the result of pulmonary pressure and airflow rates, abnormalities in these parameters can affect the wave as well. The overall glottal configuration also plays a role in the vibratory pattern. We will discuss each of these components individually.
 Respiratory Effects on Mucosal Wave
Respiratory Effects on Mucosal Wave
The inability to generate adequate respiratory support, intentionally or unintentionally, causes the vibratory component of vocal fold movement during phonation to decrease and results in a decrease of the mucosal wave. For example, in a patient with a tracheotomy and no vented airflow to the larynx, no vocalization is present due to lack of a power source, so no mucosal wave is present. Pathologic etiologies such as asthma, emphysema, and other pulmonary disorders that decrease glottal airflow can decrease the mucosal wave by the same mechanism.
Neurologic disorders affecting respiratory strength, such as post-polio syndrome and other central neurologic pathologies, can also decrease pulmonary function and subsequent vibration. Furthermore, abnormalities of glottal function linked to abnormal “respiratory” patterns can cause decreases in the mucosal wave, such as paradoxical vocal fold motion, spasmodic dysphonia, and other dystonias or neurologic disorders. In addition, hypofunctional and aphonic vocalization created by poor functional respiratory effort will produce a lack of airflow and, therefore, cause a decrease or absence of the mucosal wave.
 Glottal Configuration Effects on Mucosal Waves
Glottal Configuration Effects on Mucosal Waves
Glottal configuration patterns also play a role in mucosal wave development. Hypofunctional or hyperfunctional patterns of closure will affect the vibratory edge and can be shown to change the mucosal wave. In situations where a lack of contact between the vocal folds takes place, such as presbyphonia (Fig. 20.3; Video Clips 16, 17, and 24), vocal fold paralysis (Fig. 20.4; Video Clips 25, 27, and 28), and hypofunctional muscle tension dysphonia (Fig. 20.5; Video Clip 20), the mucosal wave can be decreased or absent. In these situations, inadequate forces opposing the vocal folds alter the vibratory pattern by decreasing the build-up of subglottal pressure.
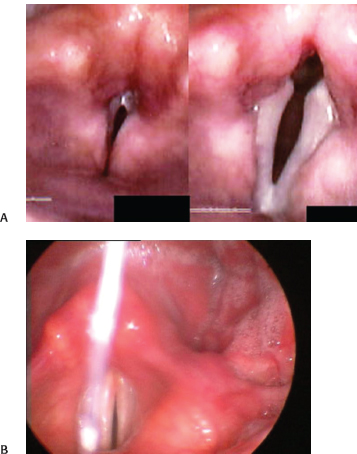
Fig. 20.3 (A) Presbyphonia. On the left, supraglottic tension obscures view of the vocal folds. On the right, the concave contour of the folds is better appreciated. (B) Presbyphonia with the vocal folds at maximum adduction. Note the persistent glottic opening.
 Medial Compressive Forces
Medial Compressive Forces
Decreases in the mucosal wave can be seen in situations of hyperfunction when the muscular tension on the vibratory edges of the vocal folds becomes too great for the subglottal air pressure to overcome. This phenomenon is most typically seen in hyperfunctional muscle tension dysphonia (Fig. 20.6) but is also seen in disorders such as spasmodic dysphonia (Fig. 20.7) and central neurologic disorders. It is important to remember that normal vibratory structures likely exist in these patients and that it is the forces at the glottal level that limit airflow and vibratory function. Additionally, extreme hyperfunction can prevent the visualization of the vocal folds, making evaluation of vocal fold vibration impossible (Fig. 20.8).
Studies have shown that specific muscle activation and firing patterns alter the vocal fold vibratory pattern and that certain sequences increase the stresses on the vibratory margin.3 However, quantifying or distinguishing the forces causing the decrease of the mucosal wave in various muscular patterns seen clinically is not currently readily achievable. As most models now being used to quantitatively describe the impact of changes in the various components of the laryngeal vibratory system are theoretical models, their use in the clinical setting is problematic.
 Superficial Lamina Propria and Mucosal Effects on Mucosal Wave
Superficial Lamina Propria and Mucosal Effects on Mucosal Wave
The limitation of many theories about vocal fold injury and healing is the fact that they are based on studies using animal and in vitro models, so direct data on human disease processes is not available. What we do know is that the role of the superficial lamina propria in the development and resolution of glottal edema is likely related to its role in the development of vocal fold fibrosis, both in short-term and long-term outcomes. Increased intravas-cular pressure at the vocal fold edge has been shown to affect vocal vibration and is theorized to be a component of the response to injury of vocal folds.4 In addition, the vibration of vocal fold fibroblasts increases the production of matrix proteins in the lamina propria, such as fibronectin and collagen type 1.5 Changes in collagen types and quantity are an important factor in scarring in any tissue and are critical at the vocal fold vibratory margin. This type of alteration of the balance of the lamina propria components can result in changes to mucosal wave patterns. One of the more important inferences that can be made from the evaluation of the mucosal wave during a diagnostic videostroboscopy concerns the health of the superficial lamina propria and overlying mucosa.
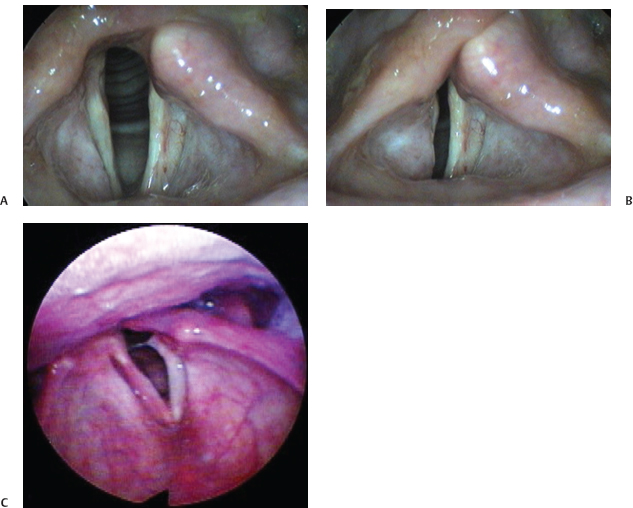
Fig. 20.4 (A) Left vocal fold paralysis with the vocal folds in an abducted position. (B) Left vocal fold paralysis with the vocal folds adducted. A persistent glottic opening is apparent even at maximal adduction. (C) Vocal fold paralysis and contralateral hemorrhage. The lateralized position of the left vocal fold prevents closure despite medial movement of the right vocal fold.

Fig. 20.5 Hypofunctional dysphonia with a persistent glottic opening.
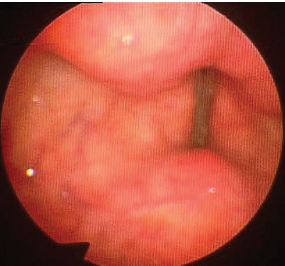
Fig. 20.6 Hyperfunctional dysphonia. Notice medialization of ventricular folds secondary to squeezing.
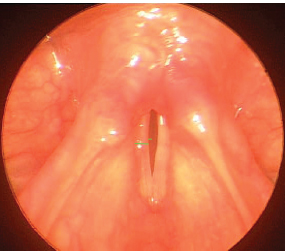
Fig. 20.7 Adductor spasmodic dysphonia. The vocal folds appear normal but the mucosal wave is less than one half of the width of the vocal fold. The short green line depicts the width of the right mucosal wave, and the longer green line depicts the width of the right vocal fold. Normally, the short green line should be about half the length of the long green line.

Fig. 20.8 Severe hyperfunctional dysphonia. The ventricular folds obscure the true vocal folds, preventing evaluation of their vibratory characteristics.
It is important to remember that the progression of a patient along the spectrum of edema, stiffness, and frank scarring is not absolute or irreversible. The acute mass effects caused by fluid or blood due to edema and hemorrhage can cause a decease in the mucosal wave patterns by themselves (Fig. 20.9). Following the mucosal wave recovery through repeated videostroboscopic examinations can be an effective way to monitor the recovery of the vocal fold in these processes. Persistent decrease of a mucosal wave can indicate a fibrotic reaction and cause concern about potential scarring (Fig. 20.10).
Scarring and the associated loss of the normal superficial lamina propria structure represents one of the most common diagnoses indicated by a decreased mucosal wave. The complete absence of a mucosal wave implies that the superficial lamina propria has been completely eradicated (Video Clips 32 and 33). The results of vocal fold stripping procedures are an extreme example of this problem (Fig. 20.11). Affected patients demonstrate no mucosal wave throughout the vibratory edge, indicating that the superficial lamina propria was likely removed with the surgical procedure and has now been replaced with more fibrotic tissue.

Fig. 20.9 Vocal fold edema. The swelling of the superficial lamina propria secondary to fluid in the interstitial space results in a decreased mucosal wave.
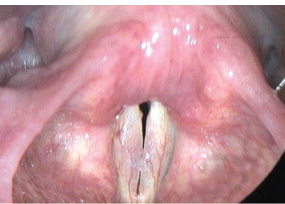
Fig. 20.10 Fibrotic reaction resulting in scarring and a decrease in the mucosal wave.
A decreased mucosal wave can also provide information about the state of mass lesions on the vocal fold vibratory edge, such as the degree of associated fibrosis (Video Clip 40). Changes in the mucosal wave can indicate the depth of the lesion, as in premalignant lesions, as well as provide information about how amenable a benign lesion is to nonsurgical and surgical intervention. Leukoplakia, a white keratotic patch, is a lesion in which the decrease of mucosal wave can be concerning, as a cancer diagnosis can be more likely when a decreased mucosal wave indicates involvement of the superficial lamina propria (Fig. 20.12; Video Clip 35). The status of vocal nodules can be aided by the evaluation of the mucosal wave over them. The presence of a continuous, normal mucosal wave over the nodules indicates they are probably not fibrotic and, therefore, more likely to resolve with voice therapy (Fig. 20.13; Video Clip 18).
 Limitations and Concerns about Mucosal Wave Interpretation
Limitations and Concerns about Mucosal Wave Interpretation
There is sometimes difficulty in interpreting the implications of differences in the mucosal wave between the vocal folds. Whereas this type of difference may represent unilateral pathology, such as paralysis or a mass lesion, left-right differences in the mucosal wave are also seen in normal individuals. The relationship of these differences to fatigue and other components are not known.6 Changes found in a normal population with the more detailed videokymographic techniques indicate that some of these changes may not be clinically significant and may not represent a cause of dysphonia.7
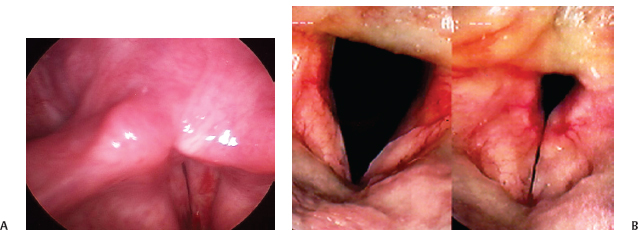
Fig. 20.11 (A) Scarring after vocal fold stripping of the left vocal fold. (B) Severe bilateral vocal fold scarring.
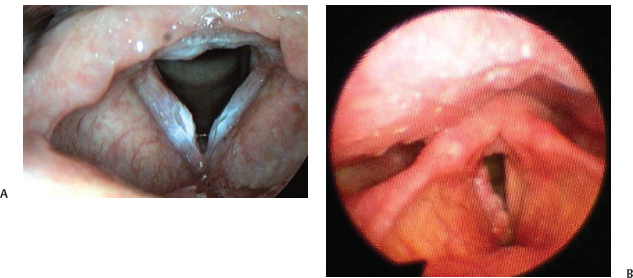
Fig. 20.12 (A) Leukoplakia of both vocal folds that may result in a decrease of the mucosal wave depending on the involvement of the superficial lamina propria. (B) Extensive leukoplakia of the right vocal fold with complete loss of the mucosal wave.
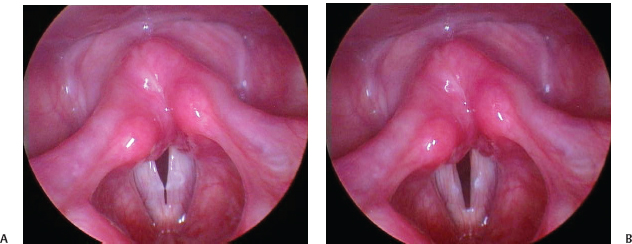
Fig. 20.13 (A) Nodule: View with superior surface of vocal folds approximated before the onset of the mucosal wave. (B) Nodule from A with mucosal wave flowing over the nodules indicating that they are soft and likely to respond to speech therapy.
Although the mucosal wave provides significant information about the state of the multilayer vocal fold structure, it is only one element of the overall evaluation of a videostroboscopic examination and must be taken in context of the entire clinical picture. Several different components of the vocal tract can cause the decrease of the mucosal wave, so it is important to look at all components and their role. Disorders affecting the respiratory power source of vibration, glottal configuration changes both organic and functional, and vibratory edge lesions can all play a role in decreasing the vibratory effect.
References
1. Patel R, Dailey S, Bless D. Comparison of high-speed digital imaging with stroboscopy for laryngeal imaging of glottal disorders. Ann Otol Rhinol Laryngol 2008;117:413–424
2. Svec JG, Sram F, Schutte HK. Videokymography in voice disorders: what to look for? Ann Otol Rhinol Laryngol 2007;116:172–180
3. Lowell SY, Story BH. Simulated effects of cricothyroid and thyroarytenoid muscle activation on adult-male vocal fold vibration. J Acoust Soc Am 2006;120:386–397
4. Czerwonka L, Jiang JJ, Tao C. Vocal nodules and edema may be due to vibration-induced rises in capillary pressure. Laryngoscope 2008;118:748–752
5. Wolchok JC, Brokopp C, Underwood CJ, Tresco PA. The effect of bioreactor induced vibrational stimulation on extracellular matrix production from human derived fibroblasts. Biomaterials 2009;30:327–335
6. Lohscheller J, Eysholdt U, Toy H, Dollinger M. Phonovibrography: mapping high-speed movies of vocal fold vibrations into 2-D diagrams for visualizing and analyzing the underlying laryngeal dynamics. IEEE Trans Med Imaging 2008;27:300–309
7. Shaw HS, Deliyski DD. Mucosal wave: a normophonic study across visualization techniques. J Voice 2008; 22:23–33
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


