 ecause the tenon capsule is a reactive tissue and contributes to filtration failure as a result of the formation of scarring, tenon cysts, or both, it is logical to avoid this tissue in the course of glaucoma surgery. The tenon capsule is firmly attached to the limbal connective tissue about 0.5 to 1 mm behind the insertion of the conjunctiva. This creates a potential pretenon space between the anterior conjunctiva and the limbal connective tissue. The Fugo blade makes it possible to use this space to create a filtering track, with the aim of minimizing tenon capsule involvement.
ecause the tenon capsule is a reactive tissue and contributes to filtration failure as a result of the formation of scarring, tenon cysts, or both, it is logical to avoid this tissue in the course of glaucoma surgery. The tenon capsule is firmly attached to the limbal connective tissue about 0.5 to 1 mm behind the insertion of the conjunctiva. This creates a potential pretenon space between the anterior conjunctiva and the limbal connective tissue. The Fugo blade makes it possible to use this space to create a filtering track, with the aim of minimizing tenon capsule involvement.
A track is made from the pretrabecular cornea to the distal pretenon potential subconjunctival space. As a primary procedure, it can be applied in all cases of glaucoma with moderate or deep anterior chambers, or in which at least the anterior chamber can be deepened during surgery. Peripheral iridectomy is mandatory. It is useful for cases in which the perilimbal area has been extensively damaged or fibrosed and any attempt to make a conjunctival flap has little chance of success. The only thing required is a virgin area of limbal and perilimbal conjunctiva, so that the outflowing aqueous can drain into the conjunctival lymphatics. The greater the intact virgin conjunctiva, the more the draining lymphatics can absorb the fluid load. Ultimately, it is the volume of the draining aqueous fluid that determines the final intra-ocular pressure. If the flow from inside is unimpeded, then resistance from the subconjunctival tissues and the carrying capacity of the lymphatics determine the level of success.
A number of specific factors affect the successful outcome of ab interno pretenon filtration, as discussed below.
First, the inner openings must be patent. This means the presence of no iris tissue, no pigment, no blood, no lens matter, no vitreous, no scar formation, no regrowth of endothelium over the site of the opening, and no edema of the cornea around the hole. The size of the opening should be adequate, but what constitutes “adequate size” is difficult to measure. The opening should be large enough to create fluid pressure sufficient to overcome subconjunctival resistance and allow for proper drainage, yet does not result in hypotony.
Second, the track is not closed, minimized, or compromised by any of the factors listed above.
Third, the fluid should not be dammed by byproducts of tissue reaction. To some extent this is natural and perhaps unavoidable. In order to drain, the outflowing aqueous has to negotiate as interstitial fluid through the reactive connective tissue to get into the lymphatic network of the conjunctiva, which is surrounded by the same connective tissue.
Fourth, post operative reactivity of the tenon connective tissue may have an effect. No hard-and-fast division between the subconjunctival connective tissue and the tenon capsule exists. A closure of the external opening of the filtering track may be simple scarring, which may or may not also extend inside the track, or it may be in the form of a raised dome sitting over the external opening. The size of this dome, or the so-called tenon cyst, varies. The thickness of the tenon cyst wall also varies from an initial thin wall that canbe breached by pressing the eyeball to being so thick that you could call it “sclerification.” High-risk cases include young eyes with a thick tenon capsule, trachomatous conjunctiva with pannus formation and fornix shrinkage, prolonged treatment with local antiglaucoma medication, and previously failed surgery.
Fifth, if mitomycin must be used in ab interno filtration, it has to be delivered beneath the conjunctiva, either before making the filtration or afterward. No optimal regimen of mitomycin application has been determined. For pretrack application, it should be injected under the conjunctiva close to the limbus where the track will be made. The optimal concentration and time must be determined by the surgeon. Afterward, it is thoroughly diluted and washed with lactated Ringer solution, which has an acidic pH and is good for this purpose. For posttrack application, the anterior chamber should first be blocked with sodium hyaluronate, so that no mitomycin enters it. At the end of the application, mitomycin is flushed from beneath the conjunctiva by copious irrigation in the anterior chamber. The fluid should come out of the initial opening that was made close to the limbus. Although we do not have enough experience to recommend precisely how to use mitomycin, we do believe its use should be limited to high-risk cases.
Finally, too many variables exist in any kind of filtration surgery. Ab interno filtration reduces the number of variables, especially with regard to tissue dissection, cauterization, application of mitomycin, and suturing. Some factors remain unresolved: exact entry and exit points, dimension of the filtering track, and tissue response to the draining aqueous.
TECHNIQUE
Anesthesia
Administer a facial block. Balloon the conjunctiva with lignocaine with adrenaline and apply a pressure bandage for 5 minutes. To avoid subconjunctival bleeding, open the conjunctiva with a 100-µm Fugo blade tip and inject the anesthetic fluid with a cannula.
Surgical Technique
- Use a 100-µm Fugo blade to puncture the conjunctiva close to the limbus at the 11 o’clock position.
- Pass s curved 30-gauge cannula through this opening, and push it to negotiate the most distal, pretenon potential subconjunctival space up to the 1 o’clock position. Then balloon this track with sodium hyaluronate 1.4% or, preferably, 1.8% (Fig. 29.1).
- Make a 1.5-mm-wide, deep pocket incision in the clear cornea. Make the incision obliquely so as to allow any straight device to reach the periphery of the iris. The inner end of the incision should be about 1 mm away from the limbus.
- Inject intracameral carbachol to contract the pupil to the maximum.
- Perform peripheral iridotomy. Slightly deepen the anterior chamber with sodium hyaluronate. Introduce a 300-µm straight Fugo blade tip through the pocket incision to reach the iris periphery. Gently press the tip and maintain it still on the iris, then very briefly activate it at medium power and high intensity. A flash may be seen and an air bubble may form. An air bubble will also form under the iris, indicating that ablation does not extend beyond the iris. Withdraw the tip and irrigate the area to visualize the iris opening. If desired, you may perform an additional iridotomy close by (Fig. 29.2).
- Inject more sodium hyaluronate under the limbal conjunctiva. This is needed to prevent damage to subconjunctival tissues and buttonholing by the activated tip as it exits.
- Use a curved 300-µm Fugo blade tip to form an ab interno track. First, deepen the anterior chamber to the maximum with sodium hyaluronate. Set the Fugo blade to high power and high intensity. Carefully introduce the unactivated tip in the pocket incision and approximate it to the cornea and limbus. Keep gentle pressure on the tip in the direction of the distal subconjunctival space, then activate it momentarily. You will see a flash and feel the tip advance in the corneal tissue. A second momentary activation takes the tip into the shock-absorbing visco-elastic fluid–filled subconjunctival tissue. A sure sign of the tip emerging in the subconjunctival tissues is the appearance of cavitation bubbles beneath the conjunctiva and some sodium hyaluronate extruding through the initially made conjunctival hole at the limbus. The track is now complete. Withdraw the curved tip in a curvilinear motion.
- Any doubt about the formation of the track should be dispelled by introducing a curved 30-gauge cannula in the filtering track and making it appear under the conjunctiva. A 30-gauge cannula is 300 µm wide. The same cannula can be used to introduce mitomycin around the external opening.
- Place a large air bubble in the anterior chamber. The air bubble in the anterior chamber further seals the corneal pocket incision.
- Insert a bandage contact lens. Maintain gentle pressure on the external opening of the track to prevent shallowing of the anterior chamber.
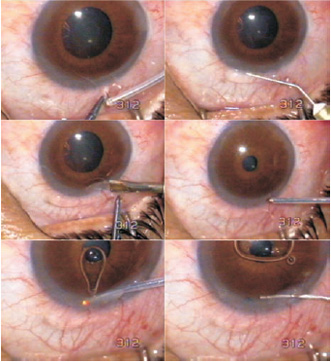
Figure 29.1. A 100-µm Fugo blade tip makes an opening in the conjunctiva close to the limbus. A 30-gauge cannula is routed beneath the distal pretenon conjunctiva and raises it by injecting sodium hyaluronate. A pocket incision is made in the cornea. A 300-µm tip is passed into the anterior chamber and is activated after touching the peripheral iris. An iridectomy is performed and becomes visible when the viscous agent is injected to deepen the anterior chamber.
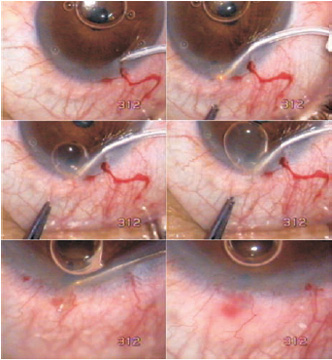
Figure 29.2. A curved 300-µm Fugo blade tip is introduced through the corneal pocket incision. It is activated and passed through the peripheral cornea into the distal subconjunctival space. The bleb made from viscous sodium hyaluronate prevents injury to the conjunctiva. The resulting track is confirmed by passing a 30-gauge (300-µm diameter) curved cannula through it.
Postoperative Management
Have the patient open the eye after 4 hours, when the effect of the facial block wears off. The bandage lens is usually in place and sits on the fluid-lifted conjunctiva. The anterior chamber is usually well formed, or it may be shallow.
Prescribe pilocarpine 2% twice a day. Even though an iridectomy is in place in line with the internal track opening, a contracted pupil ensures that the iris does not cause a block. To minimize subconjunctival fibrocytic reaction, prescribe steroid–antibiotic drops seven to eight times a day and steroid–antibiotic ointment at bedtime.
Remove the contact lens after two days. By this time, the conjunctival hole at the limbus is closed. At the end of 3 days, satisfactory anterior chamber depth and an extensive borderless bleb are usually achieved. The bleb edema reduces in a week to 10 days.
Taper steroid treatment in about 2 months.
Failure after Ab Interno Filtration
Track failure occurs for two reasons: closure of the internal opening or closure of the outer opening. Gonioscopy establishes the cause and guides the treatment.
If the internal opening is blocked with iris, pigment, or any nondescript debris, it is cleared with neodymium:yttrium–aluminum–garnet laser shots. The fluid will begin to drain and a bleb raises around the outer opening. If the inner opening is clear, the track or the outer opening needs attention.
Early raised intra-ocular pressure with nonformation of a bleb or a rapidly failing bleb may be managed by reopening the track, once again using the ab interno approach. Topical anesthesia is enough. Pressure with a curved cannula opens the original pocket incision, from where the cannula is guided into the filtration track. Fluid is injected through the cannula to clear the track and the outer opening. Depending on the situation, it may be desirable to inject antimitotic medication under the conjunctiva via the same route.
Summary
Ab interno filtration using the Fugo blade is an alternative technique for draining aqueous fluid. Further refinement of this technique is possible with improved blade tips and videovisibility through an ultrathin high-quality fiberoptic system.
Suggested Reading
Ozler SA, Hill RA, Andrew JJ, et al. Infrared laser sclerostomies. Invest Ophthalmol Vis Sci. 1991;32:2498.
Scimeca G. Phaco with transciliary filtration an alternative to triple procedure. Ocular Surg News. 2005;23:58.
Singh D, Bundela R, Agarwal A, et al. Goniotomy ab interno: “a glaucoma filtering surgery” using the Fugo plasma blade. Ann Ophthalmol. 2006;38:213–217.
Sugar HS. Surgical anatomy of glaucoma. Surv Ophthalmol. 1968;13:143.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


