 tenon capsule is like a hornets’ nest: disturb it and it strikes back. Most postsurgical complications after filtration procedures arise from the tenon capsule. The Fugo blade makes it possible to bypass the reactive tenon capsule (or at least to disturb it only minimally) while creating a basic minimum filtering track. The external pretenon approach may be transconjunctival, open, or subconjunctival.
tenon capsule is like a hornets’ nest: disturb it and it strikes back. Most postsurgical complications after filtration procedures arise from the tenon capsule. The Fugo blade makes it possible to bypass the reactive tenon capsule (or at least to disturb it only minimally) while creating a basic minimum filtering track. The external pretenon approach may be transconjunctival, open, or subconjunctival.
Under a slit-lamp microscope, the normal conjunctiva close to the upper limbus looks like a delicate transparent curtain. The membrane can be moved side to side over the underlying tenon capsule with simple thumb pressure over the lid. In fact, the conjunctiva is loosely tied to the tenon capsule and is not an entirely independent layer. Free movement of the conjunctiva is facilitated by looseness of the subconjunctival tissue and especially by virtue of a small quantity of interstitial fluid. This interstitial fluid can be tremendously increased in angioneurotic edema (chemosis) or after a filtration surgery (bleb). Angioneurotic edema is diffuse; when the edema subsides, the conjunctiva completely returns to normal. A surgical bleb is a blister; it is characterized by the presence of scarlike tissue in and around it. A bleb is also subject to temporal changes such as scarring, tenon cyst formation, or ballooning and thinning. Some of these changes are a prelude to leakage, inflammation, and infection. These very changes can cause surgery failure in two ways: a rise of intra-ocular pressure or, at the other extreme, hypotony.
On the basis of our research, we believe that regulation of fluid movement beneath the conjunctiva is largely controlled by conjunctival lymphatics. They facilitate removal of excess fluid and in the process also offer some resistance.
The concept and reality of lymphatics under the conjunctiva are important for glaucoma surgery. A reliable connection between the conjunctival lymphatics and the anterior chamber without involving other tissues would solve nearly all the problems inherent in glaucoma surgery. Surgery to control glaucoma simply means the continued transfer of fluid from the anterior chamber to under the conjunctiva.
If we could pull the conjunctiva down over the limbus and create a transconjunctival filtering track through the limbus into the anterior chamber, and if that could ensure a continued track that would withstand the repairing forces of related tissues, we would need to look no further for a surgical technique for filtration. But multiple factors come into play the moment a track is made, some of which may lead to undesired results or complete failure.
Microtrack Filtration or Transconjunctival Anterior Chamber Filtration
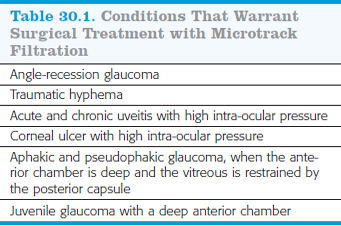
This procedure was first performed by Daljit Singh in 2004. Conditions that warrant microtrack filtration are shown in Table 30.1. Microtrack filtration can be used in other glaucoma cases if the anterior chamber is deep. The presence of a peripheral iridectomy in the region of filtration is helpful.
TECHNIQUE
Anesthesia
Surface anesthesia may be sufficient. To ensure that the patient feels no pain and will not move the eyeball at a critical moment during the procedure, balloon the conjunctiva with lignocaine 2% followed by 5 minutes of pressure under a pad.
Surgical Technique
- Hold the conjunctiva lightly with a plain forceps about 3 mm from the limbus. Pull it down over the cornea to determine the amount of resistance (Fig. 30.1–30.5). When the subconjunctival connective tissue/tenon capsule is caught by the forceps, it will resist being pulled down. The less the resistance the better, because that indicates that the tenon capsule is not being dragged down.
- Observe the limbus beneath the pulled-down conjunctiva, which should be nearly transparent. The track has to be made through the conjunctiva and the limbus without a counterpuncture. Therefore, the limbus should either be visible at all times or else physically protected from accidental touch by the Fugo blade. For better observation, stain the limbal conjunctiva with gentian violet. When the conjunctiva is pulled down, the limbus appears as a straight dark line. To avoid creating a buttonhole, do not cross this line.
- Use a 100-µm Fugo blade tip. The tip is bent in such a way that it moves smoothly in the right direction when the track is being made. Make a dry run to ensure a smooth, practiced movement during the actual procedure.
- The limbal area is visible through the transparent conjunctiva. It is up to the surgeon to decide at which point of the limbus to make the filtration track. Vertical entry at the posterior edge of the limbus will take the track to the anterior corneoscleral trabeculae. A track made close to the conjunctival attachment will open inside the anterior chamber far away from the corneoscleral trabeculae.
- Either pull down the conjunctiva with a metallic forceps or slide it toward the cornea and hold it down with a noncutting nonmetallic blade (Fig. 30.1).
- It takes only a tiny fraction of a second to make the filtration track. Keep the filament steady with very light pressure on the target tissue; it is best to hold your breath. The moment the Fugo blade is activated from the foot switch, it passes through the conjunctiva and the limbus into the anterior chamber. Fine bubbles appear in the anterior chamber from the tip. Release foot switch immediately to deactivate the Fugo blade.
- As the ablation tip is withdrawn, aqueous ooze follows and begins to lift the conjunctiva over the external opening. You can inject air, miotics, or sodium hyaluronate (Healon) into the anterior chamber through a fine cannula. Then allow the conjunctiva to retract to its normal position. Insert a bandage contact lens to support the external opening of the track and prevent overfiltration.
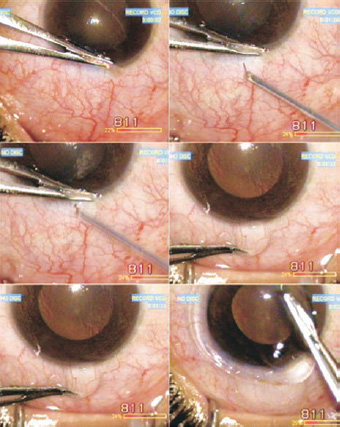
Figure 30.1. The conjunctiva is pulled over the cornea and a 100-µm Fugo blade tip is used to create a transconjunctival filtering track. A bandage lens is applied at the end of surgery.
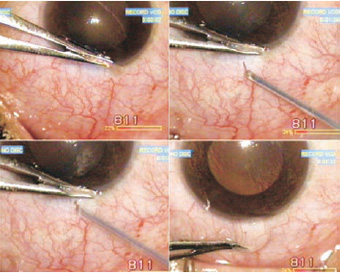
Figure 30.2. The conjunctiva is slid toward the cornea and held down at the limbus with a nonconductive crystal blund knife. A pointed 300mm Fugo blade repeatly pushes against the sclera to enter the anterior chamber. Air is injected into the anterior chamber.
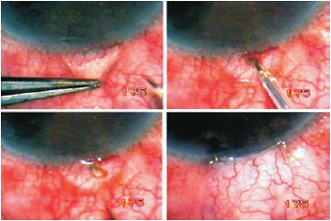
Figure 30.3. Open pretenon filtration. The detached and pulled conjunctiva reveals the insertion of tenon capsule. The filtration track is made anterior to the tenon insertion. As fluid starts draining, the conjunctiva is sutured back.
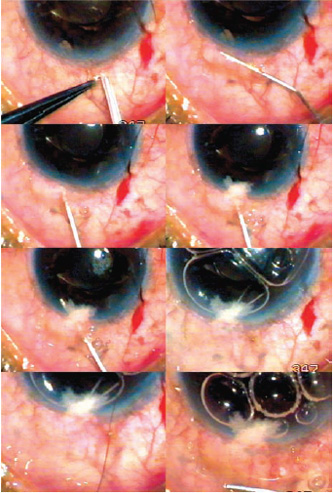
Figure 30.4. After making a hole in the conjunctiva close to the limbus, the pretenon space is opened first with saline and then ballooned with sodium hyaluronate. A 300-µm Fugo blade tip is introduced in the just-created space, turned at 45-degree angle, placed under the con- junctival insertion, activated, and pushed into the anterior chamber. Air is injected into the anterior chamber, and the initial conjunctival hole is closed with a suture.
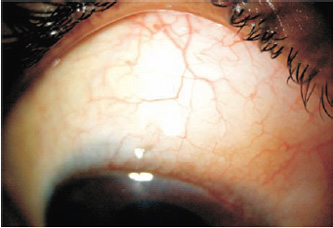
Figure 30.5. Extensive borderless bleb in a microtrack filtration that was carried out in the pretenon potential subconjunctival space.
In 2007, Kiranjit Singh began using the clear cornea filtration track, in which the ablating tip travels in the clear cornea before opening in the anterior chamber. The internal opening in these cases is directly visible under a slit lamp, without need of a goniolens. If internal closure of the track occurs because of an iris touch, the iris can be released by moving the iris with either a miotic or a mydriatic agent or else with a single shot of a neodymium:yttrium–aluminum–garnet (Nd:Yag) laser. In case of an iris block, my approach is to leave it alone for a couple of days while some resistance develops in the subconjunctival tissues, allowing for better control of anterior chamber depth when the iris is released. An internally blocked track can also be opened by injecting air or sodium hyaluronate through a small corneal incision.
Because of the uncertainty regarding anterior chamber depth and internal blockage with the iris after surgery, close monitoring is needed for 2 to 3 weeks, with additional minor interventions, if needed.
Surgical treatment of patients with juvenile glaucoma is particularly troublesome because of grave uncertainties connected with all surgical techniques. The conjunctiva in pediatric patients is transparent and very mobile. It is easy to make a transconjunctival track. Use a sharp, pointed Fugo blade tip to create the smallest possible internal opening right under the root of the conjunctiva. A very small internal opening and slow leakage reduces the risk of anterior chamber collapse and iris block. Place a bandage lens. Some astounding results have been obtained in young patients. The bleb formation is peculiar, in that no bleb at all appears; the conjunctiva is lifted diffusely and appears smooth and white.
Anterior chamber microfiltration cases require careful follow-up and management. The pupil needs to be contracted to keep the iris away from the internal opening of the filtration track. Cases with deep anterior chamber do better. A prefiltration laser peripheral iridotomy (PI) helps to some extent but a larger manual PI is better.
Postoperative Management
Patch the eye for 2 hours to allow the effect of the local anesthetic to wear off. Prescribe pilocarpine to be used three times a day to keep the pupil contracted, plus the usual antibiotic–steroids. Monitor the depth of the anterior chamber and the shape of the pupil. An oval pupil means iris attachment to the internal opening, which will result in deepening of the anterior chamber, followed by a rise in intra-ocular pressure.
Open Pretenon Filtration
The open technique for microtrack filtration was first performed by Dr. Hampton Roy in 2004.
Surgical Technique
- Detach about 3 mm of the conjunctiva from the limbus.
- Allow any bleeding point to close by itself. Do not cauterize.
- Lift the conjunctiva to see the tenon capsule veil. The anterior limit of tenon capsule is visible. The open space anterior to it is the pretenon potential space that has been surgically opened.
- Use a sharp, pointed 300-µm Fugo blade tip at medium power and energy to make a filtration track anterior to the visible end of the tenon capsule (Fig. 30.3). A small pointed tip produces a track that is widest (about 400µm) outside and narrowest (about 200µm) inside. The tip may be directed at a 45-degree angle.
- Switch off the energy the moment cavitation bubbles appear in the anterior chamber and withdraw the tip. The fluid starts moving through the newly made track.
- Inject intracameral carbachol to contract the pupil.
- Inject air to deepen the anterior chamber. You may inject sodium hyaluronate in the anterior chamber to support it for a couple of hours.
- Replace the detached conjunctiva with one or two sutures.
Closed/Subconjunctival Pretenon Filtration
It is possible to create a filtration track from the pretenon subconjunctival space to the anterior chamber using the technique described below.
Surgical Technique
- Use a 100-µm Fugo blade tip to make a hole in the conjunctiva close to the limbus at approximately the 11 o’clock position (Fig. 30.4).
- Balloon the conjunctive by injecting saline. Insert a 30-gauge cannula along the limbus while the saline is injected. Some fluid force plus manual force of the cannula is required to open up pretenon potential subconjunctival space.
- Inject sodium hyaluronate through a 30-gauge cannula, starting at the distalmost part of the opened subconjunctival space. This firmly raises the conjunctiva like a long blister. The blister will help protect the conjunctiva from injury during the next step.
- Introduce a 300µm Fugo blade tip, fully shielded right close to the tip, through the conjunctival hole and work it in for about 2 mm. Turn it toward the anterior chamber at an angle of 45 to 60 degrees. Keep the tip close to the insertion of the conjunctiva to the cornea. At this moment the sodium hyaluronate blister surrounds the tip, so the conjunctiva is not touched. Press the tip in the desired direction of movement while holding your breath, and activate the tip. In an instant, the tip crosses the cornea to enter the anterior chamber; inactivate the tip immediately. Confirm successful entry in the anterior chamber by noting the appearance of air bubbles forming inside and by visualizing the tip. Occasionally at the moment of entry, cavitation bubbles may form inside the cornea, rendering it temporarily opaque and thereby reducing visibility of the penetrating ablative tip.
- Use a 30-gauge cannula to inject air and/or sodium hyaluronate into the anterior chamber through the newly created track.
- Close the hole in the conjunctiva with a single suture.
- Introduce a 300µm Fugo blade tip, fully shielded right close to the tip, through the conjunctival hole and work it in for about 2 mm. Turn it toward the anterior chamber at an angle of 45 to 60 degrees. Keep the tip close to the insertion of the conjunctiva to the cornea. At this moment the sodium hyaluronate blister surrounds the tip, so the conjunctiva is not touched. Press the tip in the desired direction of movement while holding your breath, and activate the tip. In an instant, the tip crosses the cornea to enter the anterior chamber; inactivate the tip immediately. Confirm successful entry in the anterior chamber by noting the appearance of air bubbles forming inside and by visualizing the tip. Occasionally at the moment of entry, cavitation bubbles may form inside the cornea, rendering it temporarily opaque and thereby reducing visibility of the penetrating ablative tip.
Bleb formation after drainage through the pretenon potential subconjunctival space is very interesting. The fluid spreads freely under the conjunctiva and a diffuse edema is produced (Fig. 30.5).
Summary
The ab externo pretenon filtration technique can be combined with Fugo blade iridotomy or laser peripheral iridotomy. One day we may have extremely fine and stiff Fugo blade tips with electronic echo facility for interface recognition. It may then be possible to use the transconjunctival approach to selectively drain the Schlemm canal or to make minimally required anterior chamber openings that will drain aqueous fluid but do not disturb anterior chamber depth.
Suggested Readings
Sugar HS. Surgical anatomy of glaucoma. Surv Ophthalmol. 1968;13:143.
Ozle SA, Hill RA, Andrew JJ, et al. Infrared laser sclerostomies. Invest Ophthalmol Vis Sci. 1991;32:2498.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


