Chapter 80 “A”, “V”, and other strabismus patterns
Overview and definitions
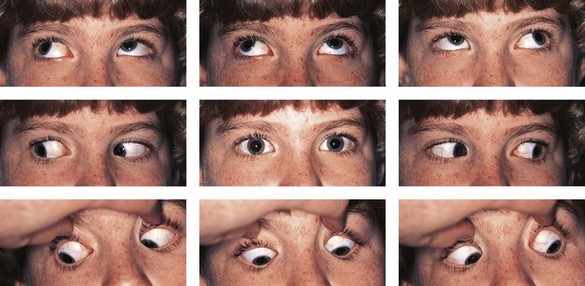
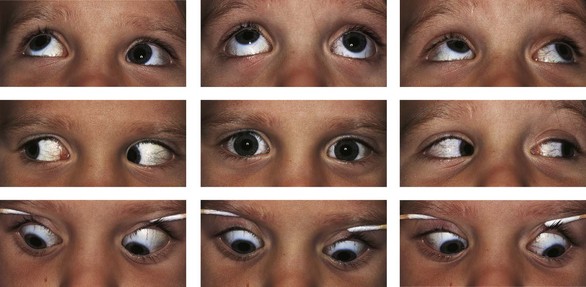
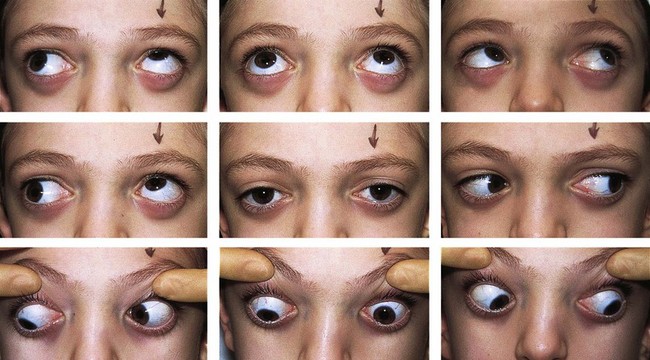
The terms “A” and “V” pattern describe horizontal strabismus that is vertically incomitant. It is characterized by a substantial difference in the horizontal deviation between the midline upgaze and downgaze positions. A patient with a “V” pattern is more esotropic or less exotropic in downgaze than upgaze (Fig. 80.1) and an “A” pattern is characterized by the converse (Fig. 80.2). By convention the difference between upgaze and downgaze must be 15 PD (prism diopters) or greater to diagnose a clinically significant “V” pattern and 10 PD to diagnose an “A” pattern. Less commonly, there are variations of pattern strabismus in which there is minimal change from downgaze to the primary position, but the eyes diverge in upgaze resulting in a “Y” pattern (Fig. 80.3 and  Video 80.1). The girl shown in Fig. 80.3 and
Video 80.1). The girl shown in Fig. 80.3 and  Video 80.1 was first diagnosed to have this motility pattern at 3 years of age. I have continued to care for her over the subsequent 33 years and her motility is unchanged. She is symptom free without treatment.
Video 80.1 was first diagnosed to have this motility pattern at 3 years of age. I have continued to care for her over the subsequent 33 years and her motility is unchanged. She is symptom free without treatment.


History
Duane first described a “V” pattern in 1897 in a patient with bilateral superior oblique palsy.1 Subsequently little attention was given to the importance of measuring the angle of strabismus in upgaze and downgaze until Urrets-Zavalia in 1948.2,3 Urist brought the “A” and “V” patterns into the English literature in 1951.4
Occurrence
Estimates of patients with strabismus having an “A” or “V” pattern range from 12 to 50%.5–8 This wide range is because ethnic and systemic factors influence the incidence of pattern strabismus and the make-up of each series. In one series of 421 patients with “A” or “V” patterns, 58% had an onset of strabismus prior to 12 months of age.6 “A” or “V” pattern strabismus occurs much more frequently in congenital or paralytic strabismus than in non-paralytic acquired strabismus. Brown’s syndrome (See Chapter 78) characteristically has a “V” pattern, differentiating it from inferior oblique palsy, in which an “A” pattern is found (Fig. 80.4). Duane’s syndrome (See Chapter 81) often presents with a “V” or “Y” pattern, and less commonly an “A” or “λ” pattern. (See Chapter 78, Fig. 78.7) “A” patterns with overdepression in adduction are frequently seen in patients with spina bifida and/or hydrocephalus with a 31% incidence having been reported.9,10 Although frontal bossing in children with hydrocephalus (See Chapter 55) may result in anterior displacement of the trochlea, mechanically enhancing the vertical vector of the superior oblique tendon with strengthening of the depressing action of the superior oblique. However, the exact mechanism is unclear.
Etiology
Oblique muscle dysfunction
The most popular theory, suggested by Knapp in 1959,11 attributes most cases of “A” and “V” pattern to oblique muscle dysfunction. Abduction is a tertiary action of the oblique muscles. Thus, if the inferior obliques are overacting and the antagonist superior obliques are underacting, one would expect a relative convergence in downgaze and divergence in upgaze, resulting in a “V” pattern. The converse occurs if the superior obliques are overacting and the inferior obliques are underacting, resulting in an “A” pattern. One typically finds the oblique muscles to be dysfunctional in this manner in most patients with pattern strabismus. This clinical observation, combined with the theoretical construct, has led to the justified implication of oblique muscle dysfunction as a cause of “A” and “V” patterns.
Torsion as a cause of “A” and “V” patterns
The torsion that accompanies oblique muscle dysfunction should theoretically cause or contribute to “A” and “V” patterns.12 Patients with a “V” pattern typically have an excyclotropia, which is most likely secondary to the accompanying inferior oblique overaction. This excyclotropia results in rotation of the rectus muscles (Fig. 80.5). The superior rectus muscles would become partial abductors and the inferior rectus muscles partial adductors, which will contribute to a “V” pattern. The medial rectus muscles will also have elevating force vectors and the lateral rectus muscles depressing force vectors, contributing to the elevation seen in adduction with overacting inferior obliques. I believe, however, that torsion is only a minor contributing cause of pattern strabismus not the main cause. Several observations support this belief.13 First, the rise or fall of an eye with oblique muscle overaction, as it moves into adduction is curvilinear. If the rise or fall were primarily caused by the change in force vectors of the rectus muscles as seen in Fig. 80.5, one would expect a linear trajectory. Secondly, surgery like the Harada-Ito procedure that mainly corrects torsion has a negligible effect on the overelevation in adduction in patients with fourth cranial nerve palsy, even when it eliminates the excyclotropia. In addition, it has been shown that objective extorsion may precede the development of overelevation in adduction and a “V” pattern in patients with infantile esotropia (See Chapter 73), by as much as several years. If the torsion caused the overelevation in adduction and the pattern, they should occur concurrently. Finally, surgery in the form of vertical transposition of the horizontal rectus muscles that successfully eliminates an “A” or “V” pattern will predictably worsen the underlying torsion (see section Horizontal transposition of vertical rectus muscles below).
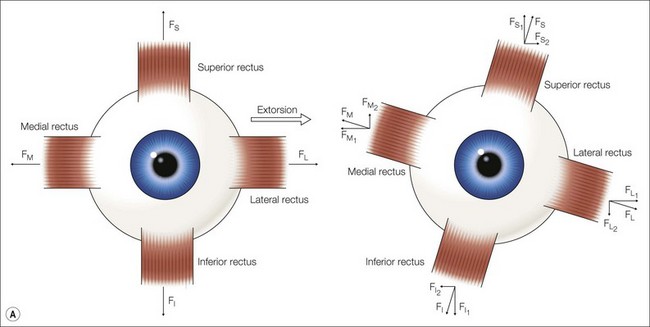
Fig. 80.5 (a) Effect of torsion on individual muscle function. An excyclorotation of the left eye will result in a clockwise rotation of the insertion of the muscles. This will create a vector for elevation of the medial rectus muscle, abduction for the superior rectus, depression for the lateral rectus, and adduction for the inferior rectus. (b) Effect of torsion on motility pattern. If the torsional changes that are depicted in Fig. 80.5A occurred in both eyes, the new force vectors would cause divergence in upgaze and convergence in downgaze. In addition there would be an elevation of the adducting eye and depression of the abducting eye. Thus, these torsional changes that occurred as a result of extorsion contribute to both the V-pattern and the elevation seen in adduction.
Orbital structural anomalies
Orbital anomalies are often associated with “A” and “V” patterns. There is a frequent occurrence of “A” pattern esotropia accompanied by inferior oblique underaction in patients with upslanting palpebral fissures and an association of “V” pattern exotropia with inferior oblique muscle overaction.14 In patients with downslanting palpebral fissures the opposite occurs. There is also a very high incidence of “A” and “V” patterns in patients with craniofacial syndromes15,16 (Fig. 80.6). Recently Clark and co-workers and Demer have attributed some cases of “A” and “V” patterns to orbital pulley heterotopia or laxity.17,18 This is an evolving concept with no good data as to the frequency that pulley issues are at fault.
Iatrogenic
An “A” or “V” pattern may develop as a result of prior strabismus surgery. This can result from an overcorrection from prior treatment of “A” or “V pattern strabismus. On occasion, a marked “Y” pattern can occur in the form of the anti-elevation syndrome after anterior transposition of the inferior oblique muscles19 (Fig. 80.7). Also, an “A” pattern frequently occurs following large bilateral recessions of the inferior oblique muscles, commonly in thyroid eye disease. This occurs from a loss of the adducting effect of the inferior rectus muscles in downgaze secondary to surgical weakening, and by an increase in innervation to the yoke superior oblique muscles.20

Horizontal rectus muscles
Urist felt overaction or underaction of the horizontal rectus muscles were responsible for “A” and “V” patterns4,5 and that the medial rectus muscles were more active in downgaze and the lateral rectus muscles were more active in upgaze. His surgical recommendations involved weakening the offending muscles. Although this theory is less compelling than others, it may explain the occurrence of some cases of “A” or “V” pattern where there is no other apparent cause. It can also explain the small decrease in “V” pattern observed after bilateral medial rectus recessions.
Other less popular theories
Brown felt that “A” and “V” patterns were caused by a weakness of the superior and inferior muscles respectively, resulting in apparent overaction of the yoke oblique muscles due to fixation “duress.”21 This theory is not widely accepted.
Gobin suggested that the primary event that causes a “V” pattern is an abnormal sagittalization of the inferior oblique muscles which decreases its vector for torsion resulting in an incyclotropia. Subsequently, to correct this abnormal incyclotropia, there is increased innervation to the excyclorotary muscles, resulting in inferior oblique overaction.22 In my opinion, this theory is inconsistent with the clinical findings of torsion in patients with pattern strabismus. According to the sagittalization theory, a patient with a “V” pattern should have no fundus torsion as the inferior oblique overaction served the purpose of eliminating an abnormal intorsion. In fact, these patients typically have objective extorsion.



