 he phrase “8-mm capsulotomy” is only a general description. The description means that we create a capsulotomy much larger than a standard 5.5-mm capsulotomy (Fig. 20.1). The precise size of the large capsulotomy varies according to the size of the eye. In sum, I make a capsulotomy 2 mm from the limbus. Many would say that this will damage zonules, but close analysis shows that this is not the case.1
he phrase “8-mm capsulotomy” is only a general description. The description means that we create a capsulotomy much larger than a standard 5.5-mm capsulotomy (Fig. 20.1). The precise size of the large capsulotomy varies according to the size of the eye. In sum, I make a capsulotomy 2 mm from the limbus. Many would say that this will damage zonules, but close analysis shows that this is not the case.1

Figure 20.1. A standard 5.5-mm Fugo blade capsulotomy is created in about 6 seconds.
Over the course of 10 years, I have performed several thousand of these large capsulotomies and yet have not had a single subluxation of an intraocular lens. From a pathophysiologic point of view, we should study patients with aniridia. In these patients, the tips of the ciliary processes extend inward toward the center of the eye such that the innermost tip of the ciliary processes reach the limbus, except on the temporal aspect of the eye, where they extend about 0.75 to 1 mm past the limbus. Because I am surgeon who performs temporal incision cataract surgery, I can easily achieve a capsulotomy 2 mm from the limbus everywhere except at the temporal aspect of the eye, where I can achieve a capsulotomy about 3 mm in from the limbus (Fig. 20.2). This procedure works out perfectly because the ciliary processes extend further inward at the temporal aspect of the eye.

Figure 20.2. It is simple to enlarge a capsulotomy with the Fugo blade. An 8-mm capsulotomy is being created around the 5.5-mm capsulotomy shown in Figure 20.1 with the Fugo blade tip under the iris out of view of the surgeon.
An 8-mm mechanical capsulorrhexis is very difficult to achieve without risk into the periphery. Yet, the 8-mm capsulotomy offers distinct advantages over the 5.5-mm capsulotomy.2 The large capsulotomy results in minimal force on the anterior capsule leaflet, thus reducing the risk of tearing the anterior capsule rim. A large capsulotomy all but eliminates anterior capsule contraction syndrome and capsule retention syndrome. I have observed that the small anterior capsule rim begins binding to the posterior capsule in 4 to 8 weeks postoperatively, thereby locking the haptics in place and preventing anterior capsule phimosis.
Because the lens is a convex structure, ablating the capsulotomy 2 mm from the limbus based on the surgeon’s view through the operating microscope actually produces a much wider rim than is seen from the surgeon’s view. This is because the surgeon is seeing a flat view of a structure that actually exists on an angle.
TECHNIQUE
The 8-mm capsulotomy allows a surgeon to quickly remove the lens nucleus from the lens bag.3 An 8-mm capsulotomy can easily be performed under the iris out of view of the surgeon as well as with a cloudy cornea (see Chapter 21: Small Pupil Cataract Surgery).
Surgical Technique
- Once you have completed an 8-mm capsulotomy, perform hydrodissection.
- Then use the phaco tip to impale the nucleus, rock it gently, and pluck it out of the lens bag.
- At this point, inject visco-elastic material behind the nucleus to push the posterior capsule back and to hold the nucleus in the pupil, where it can be mechanically cracked and phaco-emulsification performed (Fig. 20.3).

Figure 20.3. With the nucleus impaled with the phaco tip, it is lifted out of the lens bag while a viscoelastic cannula on the left places a cushion of viscoelastic material behind the nucleus.
By removing the nucleus from the lens bag, the surgeon proceeds with surgery while eliminating stress on lens zonules and minimizing risk to the posterior capsule. This technique is extremely important in cases with weak zonules such as pseudo-exfoliation.4
It should be emphasized that a Fugo blade capsulotomy can be performed in one continuous movement or can be created by joining multiple arcuate capsulotomy maneuvers (Fig. 20.4). This allows the surgeon to impale the nucleus with the phaco tip and pluck the nucleus out of the lens bag, then mechanically crack the nucleus in the iris plane (Figs. 20.5 and 20.6).

Figure 20.4. Multiple accurate capsulotomies are utilized to create an 8-mm capsulotomy in a different patient. Here the Fugo blade is under the iris in the process of creating accurate capsulotomies that are joined to create a final 8-mm capsulotomy.
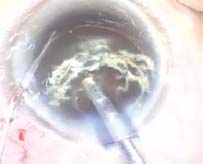
Figure 20.5. The phaco tip is used to pluck the nucleus out of the lens bag of the patient seen in Figure 20.4 while viscoelastic material is being injected behind the nucleus with the side-port cannula to push the posterior capsule back and hold the nucleus in the iris plane.

Figure 20.6. A nucleus probe is seen on the left being pushed through the body of the nucleus until it hits the phaco tip, thereby mechanically cracking the nucleus in the iris plane.
Summary
The 8-mm capsulotomy has realistic advantages for the surgeon. However, achieving a repeatable, safe 8-mm capsulorrhexis is difficult because a capsule tear that approaches the equator of the lens carries a high risk of escaping outward to the equator based on force vectors that aim the capsule tear toward the lens equator. On the other hand, plasma ablation of the anterior capsule with the Fugo blade allows a safe, repeatable 8-mm capsulotomy that may be created in one pass or in multiple passes.5 A microscopic view of a Fugo blade ablation path shows “rounded” ends that lack an acute nidus, and are therefore not prone to spontaneous tearing. Capsulorrhexis, on the other hand, has acute angles at the end of each tear in the capsule, which provides the perfect nidus for continued spontaneous tearing.6
Fugo blade plasma ablation is a paradigm shift in cataract surgery. Powered by C-cell rechargeable batteries, its low energy output is the foundation for its unparalleled safety profile even with weakened corneas or weakened zonules. Most importantly, the Fugo plasma blade allows the surgeon to perform surgeries that were previously almost impossible to perform without this novel technology.7
References
1. Kent C. Minimizing zonular stress with the plasma blade. Ophthalmol Manage. 2004;8:157.
2. Fugo RJ. Mature cataracts: how to breeze through them. Ocular Surg News. 2006;24:8–9.
3. Fugo R. Cushioned PhacoXcap technique addresses difficulties with small pupils, hard cataracts. Ocular Surg News. 2005;23:16–17.
4. Kent C. PhacoXcap: a new procedure makes it possible to phaco both nucleus & cortex outside the capsular bag. Ophthalmol Manage. 2002;6:80.
5. Charters L. Cataract surgeons gain better control with capsulotomy blade. Ophthalmol Times. 2003;28:16.
6. Fugo RJ, DelCampo DM. The Fugo blade™: the next step after capsulorrhexis. Ann Ophthalmol. 2001;33:12–20.
7. Video journal of cataract & refractive surgery. New Dev New Devices Fugo Blade. 2002;18(1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


