Yttrium-Aluminum-Garnet Laser Use in Pseudophakia
Adam H. Rogers
Caroline R. Baumal
Posterior capsule opacification (PCO) is a significant cause of treatable visual loss occurring after cataract surgery. PCO is at present the most common complication of cataract surgery, occurring in up to 10% to 50% of patients at 3 years after cataract extraction.1 Although both pharmacologic andinvasive surgical methods have been used to treatPCO, the neodymium:yttrium-aluminum-garnet (Nd:YAG or YAG) laser remains the standard of care for the treatment of PCO after cataract surgery.2,3,4,5 In the United States alone, 573,000 YAG laser capsulotomies were performed on Medicare beneficiaries in 1998. Thus, this procedure is performed on a significant number of patients who have undergone cataract extraction each year with a tremendous economic impact.
HISTORICAL TREATMENT OF POSTERIOR CAPSULE OPACIFICATION
Before development and widespread availability of the Nd:YAG laser, surgical capsulotomy was the primary treatment of PCO. In the presence of an anterior chamber lens, one approach was to pass a small gauge needle or fine blade through a limbal incision under topical anesthesia (either at the slit lamp or operating microscope) to create an opening in the posterior capsule. The cutting instrument could be maneuvered behind an anterior chamber intraocular lens (ACIOL). The limbal technique offered the lowest risk of rupturing the anterior hyaloid face. Cystoid macular edema and vitreous to the incision were the main complications.6,7 However, the presence of a posterior chamber intraocular lens (PCIOL) made the limbal approach more difficult and led surgeons to advocate a pars plana approach to open the posterior capsule. In the operating room, a vitrectomy instrument was inserted at the pars plana and activated to create a central opening in the posterior capsule.
ND:YAG LASER
The Nd:YAG laser is a solid-state model that was developed in the early 1980s by Frankhauser and Aron-Rosa. It contains an artificially produced garnet crystal consisting of yttrium and aluminum oxides in which roughly 1% to 2% of the yttrium ions are replaced by the rare earth element neodymium (Nd). The electrons are activated to an excited state by an intense light source and the energized ions emit photons of light. Mirrors at each end of the laser cavity reflect the photons of light, and amplify the amount of photons produced. In this process, laser light is generated at a wavelength of 1064 nm in the near infrared spectrum.8,9
MECHANISM OF ND:YAG LASER PHOTOCOAGULATION
Q switching is a property of the Nd:YAG laser that allows the laser cavity to store energy. The Q switch acts as a type of optic shutter that blocks laser emission and promotes storage of large amounts of energy. When the shutter is open, accumulated energy can be instantaneously released as a short burstwith a duration of approximately 10 nanoseconds.The released energy is focused on a focal target me-dium and generates electrically conductive “optic plasma.” The electrons orbiting the medium become dissociated from their atoms and free electrons are generated. Nd:YAG laser disruption of the target medium results from the stripping of electrons and the production of elevated temperatures and shock waves. Thus, the Nd:YAG laser functions as a photodisruptive agent to break down target tissues. Increasing the energy of each pulse can also increase the amount of disruption. In contrast to photocoagulating lasers that rely on absorptiveproperties of the material, the Nd:YAG laser is independent of absorptive properties and can be applied even to transparent structures.8,9 This property of the Nd:YAG laser makes it useful in the treatment of PCO after cataract surgery.
ND:YAG POSTERIOR CAPSULOTOMY
INDICATIONS
Despite major advancements in cataract surgery, complete removal of all lens epithelial cells at the time of surgery is currently not possible. The posterior lens capsule and a portion of the anterior capsule remain in place to support a posterior chamber lens during modern extracapsular cataract extraction techniques. Posterior capsular opacification occurs when retained lens epithelial cells from the equator of the anterior capsule proliferate, undergo metaplasia, and then migrate across the posterior capsule. Posterior capsular opacification occurs in two forms: Elschnig’s pearls and fibrotic changes from residual cells that undergo metaplastic transformation into myofibroblasts.1,10 In the past, visually significant PCO requiring YAG capsulotomy occurred in 57% of eyes at 3 years after cataract surgery.5 However, with current techniques, this figure has been significantly reduced.
The visual symptoms produced by the PCO may mimic those of the primary cataract. Thus, PCO is often referred to as a “secondary cataract.” However, the visual impairment may be insignificant and thus require no intervention despite the clinical presence of PCO. A significant PCO requiring treatment may produce decreased visual acuity, glare, photophobia or impaired contrast, and color sensitivity. Patients generally notice a slow decline in visual quality after the initial visual improvement following cataract surgery.
On clinical examination, retinoscopy identifies a red reflex that may be normal or slightly dull and irregular. Despite the ability to perform retinoscopy, the manifest refraction typically does not improve visual acuity. Slit lamp examination with side illumination demonstrates a thickened, irregular posterior capsule that may be slightly opacified or translucent (Fig. 1). Multiple vesicles in the capsule represent flattened Elschnig’s pearls. Fluid in the vesicles is typically clear but may occasionally be turbid. Retroillumination may enhance the thickened, vesicular appearance of the posterior capsule. Examination of the retina is imperative to exclude other causes of decreased central vision that may occur after cataract surgery including cystoid macular edema, diabetic macular edema, or retinal detachment. Venous occlusive disease and age-related macular degeneration are additional causes of diminished visual acuity that commonly occur in this elderly population who undergo cataract surgery.
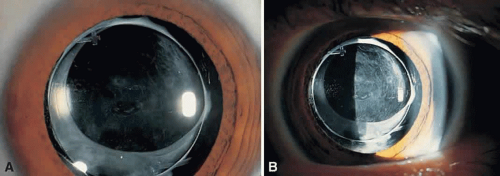 Fig. 1. Examination by diffuse (A) and side (B) illumination demonstrates a thickened, opacified posterior capsule. |
PROCEDURES
The Nd:YAG laser is a slit-lamp-mounted system with a double spot helium-neon aiming beam that merges to one beam with fine focusing. The eye is anesthetized topically and a contact lens maybe placed on the cornea if magnification of the posterior capsule is desired. The pupil may be pharmacologically dilated or remain undilated, depending on the preference of the treating ophthalmologist. Apraclonidine hydrochloride 1% is administered before laser treatment to prevent postoperative intraocular pressure (IOP) elevations. With the patient secured in the slit-lamp-mounted laser, the red helium-neon beam is focused on the posterior capsule so that energy is not transferred to the IOL or anterior hyaloid face. When properly focused, the two aiming beams merge into one. An initial laser power setting of 1.0 mJ or less is used to commence treatment. When Nd:YAG energy is successfully delivered to the posterior capsule, a break appears that enlarges along the lines of tension. Occasionally gas bubbles form on the capsule, which either clear spontaneously or can be dislodged by gently tapping on the contact lens. If the initial power setting fails to create an opening through the capsule, the energy level is gradually increased until laser disruption of the capsule occurs. Attempting to create a single opening in the capsule without increasing the energy level is ineffective and acts only to increase the total energy delivered to the eye. It is rarely necessary to increase the Nd:YAG laser power above 2.5 mJ.
Multiple techniques exist to create an opening in the posterior capsule. These include cruciate, circular, or inverted U-shaped patterns. With the pupil in an undilated state, single shots are placed in the visual axis. Regardless of the technique, the goal is to create an opening in the posterior capsule that is slightly larger than the resting pupil (Fig. 2). Typically, this will be 3 to 4 mm and require 30 to 40 spots of laser to the posterior capsule. An effective way to minimize the number of laser applications is to treat the areas of capsule under tension. The openings created expand from the tensile forces of the opacified capsular bag. In a thickened opacified capsule, pieces of the capsule may be released into the anterior vitreous. These pieces inferiorly migrate out of the visual axis within 1 week of treatment without inducing any visual disturbances.
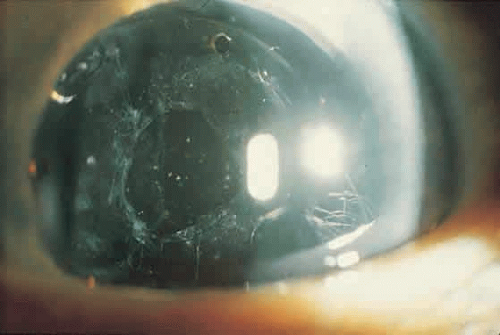 Fig. 2. Opening in the posterior capsule from a Nd:YAG laser following cataract surgery. |
Most YAG capsulotomies are uncomplicated; an opening in the capsule is successfully created in 98% of cases.11 Visual acuity improves almost immediately following treatment. The eye may be treated before or after the procedure with apraclonidine 1% to blunt a potential rise in IOP, which is measured 20 to 60 minutes later. Persistent elevation of IOP occurs infrequently and is typically treated with an ocular hypotensive agent and close observation. Corticosteroid eye drops three or four times daily (e.g., fluorometholone acetate or prednisolone acetate 1%) for 4 to 7 days is a management option used by some ophthalmologists. Generally, patients experience only minimal symptoms, if any, after this procedure. Follow-up typically occurs in 1 week, unless the IOP is significantly elevated on post-YAG testing. Long-term follow-up is required in eyes with persistently elevated IOP.12
COMPLICATIONS
Although Nd:YAG laser posterior capsulotomy is a relatively straightforward procedure, complications may be encountered. The most common intraoperative complication reported in a cohort of 2110 patients followed by the Food and Drug Administration (FDA) was damage to the IOL.11 Accurate focusing of the helium-neon beam on the posterior capsule prevents the occurrence of this event. However, postoperative contraction of the capsular bag can move it into very close proximity to the posterior surface of the IOL, leading to this complication. Other factors that increase the likelihood of IOL damage include increased thickness of the PCO membrane and the total laser power used. Despite the occasional creation of laser-induced pits in the IOL, these typically do not cause visual disturbances. Rupture of the anterior hyaloid face was the second most frequently reported complication occurring in 19% of the patients observed during the FDA study. Less frequently encountered intraoperative complications were bleeding in 1.0%, corneal edema in 0.3%, and iris damage in 0.4% of cases.11
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


