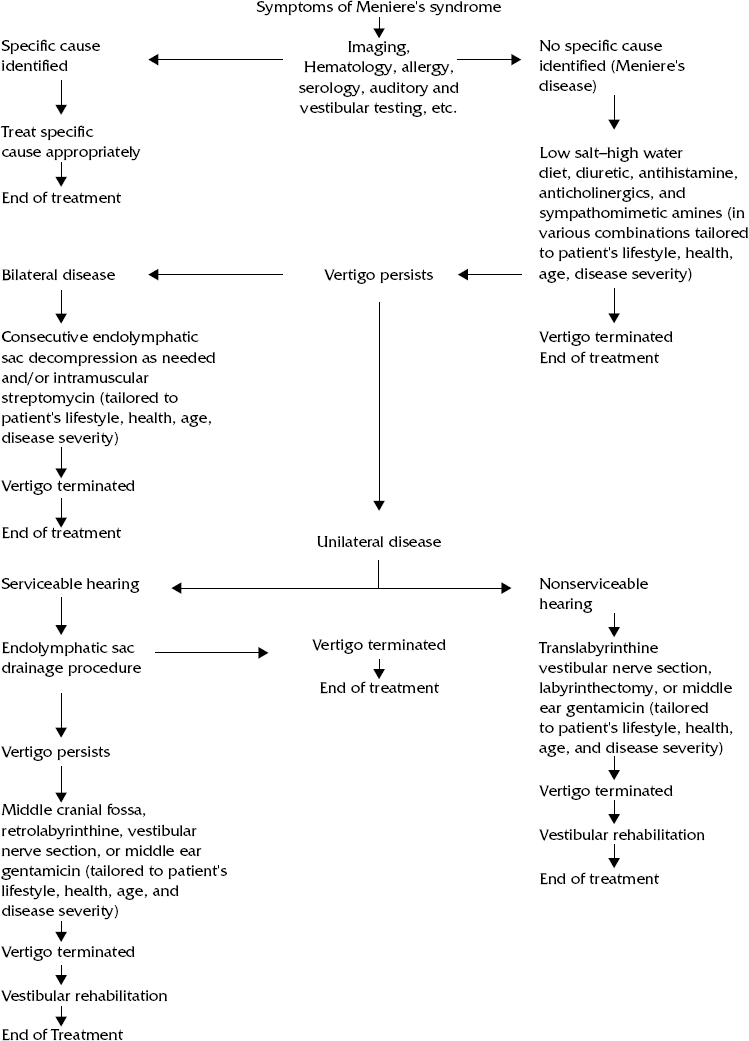
No treatment has proved effective in reversing the pathophysiologic process of Meniere’s disease. Further, no known treatment of Meniere’s disease will consistently reverse the hearing loss or eliminate the aural fullness and tinnitus that often accompany this disorder. Most treatments are directed toward eliminating the often incapacitating symptom of vertigo with its associated vegetative symptoms (Fig. 48–1). It is axiomatic that before treating the symptoms of Meniere’s disease, one must make the diagnosis. Most clinicians recognize the classic quadrad of fluctuating hearing, tinnitus, aural fullness, and incapacitating vertigo. The symptoms of Meniere’s disease, however, are frequently evolutionary, and any one of the four symptoms may precede the others by months to years.1 A high index of suspicion and the judicious use of diagnostic aids such as electrocochleography and, when hearing loss is present, dehydration audiometry can facilitate early diagnosis when doubt exists.2 Treatment may then be instituted avoiding unnecessary delay and morbidity. To complicate matters, some patients with the symptoms of Meniere’s disease (Meniere’s syndrome) will actually have a local, regional, or systemic cause for their symptoms.3 Failure to identify these causes may lead to inappropriate treatment and additional morbidity. Therefore, patients suffering the symptoms of Meniere’s syndrome should be evaluated for inhalant and food allergies, immune disease, syphilis, cerebellopontine angle lesions, and demyelinating disease. If any of these disorders are identified, their treatment takes priority. If no underlying cause can be identified, or if auditory and vestibular symptoms persist despite specific successful treatment of an identified abnormality, the cause of the patient’s symptoms is presumed to be idiopathic (Meniere’s disease). Histologic study of ears harvested from patients with Meniere’s disease has demonstrated distention of Reissner’s membrane into the vestibular scala, suggesting either overproduction of endolymph within the scala media of the cochlea or decreased absorption (endolymphatic hydrops).4 Most treatments have therefore been directed toward reducing endolymph volume pressure or bypassing the proposed pathophysiology of the disorder and directing treatment toward eliminating the symptoms of vertigo. Treatment for the vertigo that often accompanies acute spells of Meniere’s disease is designed to eliminate, or significantly reduce, this symptom and its associated nausea and vomiting. This objective is best accomplished using intravenous diazepam or droperidol if the patient can be carefully monitored. Promethazine hydrochloride (an antihistamine) in suppository form may be helpful in less controlled situations. Reassurance that the patient is not suffering a cerebrovascular accident or other life-threatening disease is essential if it is the initial attack and fluid repletion may be needed.5 Treatments used for the chronic condition of Meniere’s disease with recurrent incapacitating vertigo basically fall into the two categories of invasive and noninvasive therapy. Noninvasive treatments directed toward reversing the pathophysio-logic process include low-salt diet (< 2 g of sodium per day) and diuretics. Sodium causes fluid retention and has been implicated in the exacerbation of symptoms, presumably by increasing endolymphatic hydrops. It is hoped that low-salt diet and diuretics will have the opposite effect.6 It is proposed that some diuretics have a direct effect on ion transport in the stria vascularis and spiral ligament. Acetazolamide (a carbonic anhydrase inhibitor) and hydrochlorothiazide are commonly used. Acetazolamide appears somewhat more effective but also has a greater rebound effect when discontinued. Furosemide, a loop diuretic, may also be used but is more likely to require potassium supplementation. Vasoconstriction has never been convincingly shown to contribute to the pathophysiology of Meniere’s disease; therefore, vasodilators (e.g., niacin, histamine, papaverine hydrochlo-ride, histamine analogues) probably do not play a role in its treatment. Other noninvasive treatments used theoretically to reverse the pathologic process, such as lipoflavonoid (proposed to improve microvascular integrity of the stria vascularis), also appear to play little role in altering the pathophysiology of this disease.7, 8 Noninvasive treatments directed toward eliminating vertigo without addressing the inner ear disease process are legion. They include those treatments designed to produce temporary symptomatic relief and those designed to permanently ablate the vestibular neuroepithelium (e.g., streptomycin). Anticholinergic drugs are known to suppress activity within the vestibular system and, on occasion, reduce the vertigo associated with attacks of Meniere’s disease. They also reduce peristalsis and gastric secretion, which helps reduce nausea and vomiting, and they inhibit sweat gland activity or diaphoresis. Scopolamine and probanthine are the two most commonly used drugs in this class. Occasionally, however, the side effects of these drugs, especially scopolamine, are worse than the symptoms of Meniere’s disease, and the drugs may need to be discontinued. Antihistamines, especially those with strong anticholinergic effects, also seem to reduce the severity of the vertigo spells by suppressing the activity within the central nervous system. The precise mechanisms, however, are not totally clear. Meclizine, a piperazine derivative, is the most commonly employed antihistamine, and the side effect of drowsiness is uncommon. Amitriptyline, a dibenzazepine derivative, has not only been used to treat depression but may also reduce vertigo through its anticholinergic action. Figure 48-1 Treatment for the vertigo of Meniere’s disease. Sympathomimetic amines have long been used for suppression of vestibular symptoms. Amphetamines are notorious for substance abuse and are now under strict control by the Drug Enforcement Agency. The effects of ephedrine are similar to amphetamines but less pronounced. Ephedrine depolarizes and then blocks cells in the autonomic ganglia and appears to have the capacity of suppressing activity within the vestibular nuclei. It should be used judiciously in patients with hypertension. Psychotropic drugs, such as the benzodiazepines, have been used to treat the vertigo of Meniere’s disease. Benzodiazepines (diazepam, lorazepam, and clonazepam) either directly or indirectly enhance hyperpolarization and inhibition of neuronal firing. They are extremely effective in “crisis intervention” but their tendency to cause psychological and physical dependency argues against prolonged use.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


