Most otologic surgeons, even experienced ones, would agree that surgery for congenital aural atresia is challenging. Some submit that this procedure is inappropriate for unilateral cases, whereas others express no hesitation in recommending intervention to selected patients. The basis for this controversy has not been clearly articulated in the literature. In many cases, the bias has simply been inherited as part of the philosophy of one’s training program. In order to provide more objectivity to this issue, several possible areas of concern need to be explored: (1) impact of unilateral hearing loss, (2) probability of achieving binaural hearing with surgery and stability of hearing results over time, and (3) surgical risks, especially to the facial nerve. The purpose of this chapter is to analyze these issues and draw conclusions regarding surgery for the unilateral atretic ear.
Issue 1: Impact of Unilateral Hearing Loss
In the past, clinicians expressed little concern about unilateral loss of hearing. Recently, research has shown that children with a significant unilateral sensorineural hearing loss—and presumably a significant unilateral conductive hearing loss—do experience a variety of auditory, linguistic, and cognitive difficulties that may impact educational progress.1 Impaired sound localization1–3 and speech recognition in background noise do occur with unilateral hearing loss and may underlie these difficulties. Interestingly, the speech recognition problem occurs regardless of whether the speech stimuli are directed toward the normal or hearing-impaired ear.4, 5 These findings have obvious implications for the student in the typical classroom environment.
Both clinical and animal research have shown evidence of auditory brainstem abnormalities in the setting of unilateral conductive hearing loss. For example, Moore et al.6 have experimentally induced unilateral conductive hearing losses in ferrets during critical periods. Various abnormalities in the development of binaural neural elements in the auditory brainstem pathways were noted. Clinical studies of adults with unilateral conductive hearing loss using auditory brain stem responses (ABR) and the masking-level difference (MLD) have also documented abnormalities in brain stem auditory processing.7 Specifically, delays in wave V and in I to V and III to V interwave intervals were noted. The MLD, a behavioral test that measures the sensitivity of the auditory system to interaural differences of time and amplitude, was reduced, and they correlated significantly with the ABR abnormalities. These changes were similar to those observed in children with chronic otitis media with effusion.
Issue 2: Probability of Achieving Binaural Hearing and the Stability of Hearing over Time
No one would argue that surgery for congenital aural atresia has the same potential for hearing restoration as does stapedectomy; few middle ear procedures involving the middle ear ossicles do. But is the success rate so modest that unilateral cases are best observed, at least until the individual is an adult and can make his or her own decision?
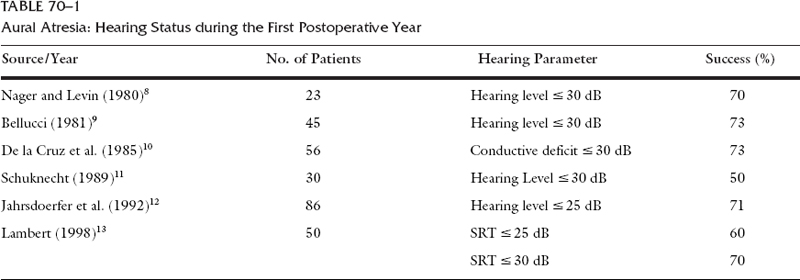
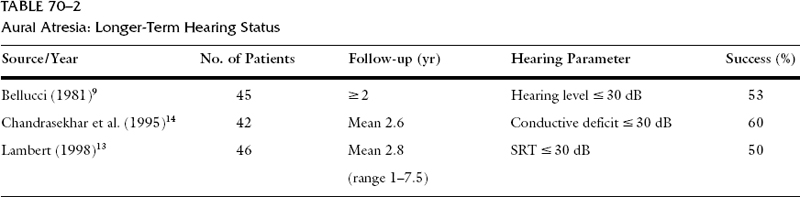
Within the first postoperative year, a hearing level of 30 dB has been achievable in approximately 70% of patients8–13 (Table 70-1). This degree of success compares favorably with many tympanoplasty procedures involving reconstruction of the ossicular chain. Like chronic ear surgery, some decrement in hearing is to be expected over time9, 13, 14 (Table 70-2) and revision surgery may be necessary. In my experience, approximately 60% of patients will achieve an excellent initial hearing result of 10 to 25 dB SRT. Approximately 75% of these individuals will maintain this level of hearing longer term (follow-up: mean 2.8 years, range 1 to 7.5 years). Considering all patients, revision surgery will be necessary in approximately one-third of cases. The most frequent complication requiring secondary surgery is stenosis of the external ear canal. Even for the highly successful stapedectomy, approximately 20% of patients will experience a significant recurrent conductive hearing loss after successful air–bone gap closure if follow up extends beyond 5 years.15
Issue 3: Surgical Risks
Injury to the facial nerve is, perhaps, the most feared complication in otologic surgery. In chronic ear disease the facial nerve may be partially obscured by granulation tissue and the infectious process may have eroded areas of the fallopian canal. The facial nerve is placed at jeopardy in cases of aural atresia because of the abnormal development of the temporal bone. This vulnerability can be minimized, however, by recognizing the anomalies likely to be encountered. Anterior and lateral displacement of the mastoid segment and dehiscence of the tympanic segment should be anticipated. The former anomaly is of particular concern when enlarging the new canal posteroinferiorly.16
Appropriate patient selection, surgical technique predicated on a thorough understanding of abnormal facial nerve development, and judicious use of facial nerve monitoring will permit aural atresia surgery with minimal morbidity. In my personal experience of 50 primary and 17 revision surgeries, one patient developed a temporary facial paresis. A series of 1000 patients was recently reported by Jahrsdoerfer and Lambert17 and an approximate 1% incidence of facial paresis or paralysis was reported. Postoperative facial nerve dysfunction can therefore, be expected in 1.0 to 1.5% of patients, an incidence which approximates that encountered during mastoid and middle ear surgery for cholesteatoma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


