Facelifting dates back to the early 1900s. A few surgeons in Europe and in the United States were experimenting with the removal of small skin strips from in front of and behind the ears.1 Dr. Jacques Joseph,2 in 1921, and Dr. Bettman,3 in 1920, were the first surgeons to publish before-and-after photographs of their facelift results. During the first 60 years of facelift surgery, dissection was limited to the subcutaneous plane. It was not until the 1950s in the United States that the “classic”; wide skin undermining facelift became the norm. This technique was not significantly challenged until Skoog4 in 1974.
Facelift surgery in the first half of the twentieth century was considered to be an act of extreme vanity. Surgeons who performed such “risky and unnecessary”; operations were looked down upon by society and the medical community. Increased public demand and affluence have led to a dramatic rise in facelifting. Consequently, the number of facelift techniques has also markedly increased.
Successful manipulation of facial tissues other than skin for facelifting began during the early 1970s due to a better understanding of facial anatomy as well as surgical anesthesia improvements. In 1974 Skoog first described his “deep-plane”; facelift, which emphasized the presence of an interconnected “skin-fat-musculofacial unit”; that, if elevated together, improved facelift results. Owsley5 further described use of the platysmal muscle for lifting in 1977. Other surgeons quickly began reporting additional techniques involving the platysma.6, 7
Innovations over the past 20 years have led to the development of the “composite,8,9 deep-plane,10 subperiosteal,11–13 laser, and endoscopic14 facelifts. Skoog’s elevation of the platysma muscle in his advancement flap sparked the interest in the musculofascial plane or superficial musculoaponeurotic system (SMAS), initially described in 1976 by Mitz and Peyronie.15 The SMAS was more accurately detailed in 1984, when Jost and Levet’s publication challenged the previous SMAS concept.16 There continues to be a great deal of disagreement, as well as confusion, regarding the best plane of dissection, not to mention the definition of surgery. The manipulation of a musculofascial plane to achieve improved and longer-lasting results has become common practice for many cosmetic surgeons. Elevation of this musculofascial plane is a key component of the biplane facelift described in this chapter.
General Approach to Facelift Surgery
In the senior author’s practice, which spans a career in facelifting of 25 years, the biplane facelift has become the workhorse operation and is used for most patients. Newer innovations, including the use of laser dissection and the skin-sparing technique described later in this chapter, basically have not altered the approach that has been in use for more than 15 years. In patients who are seeking additional upper facial rejuvenation, the biplane facelift can easily be combined with either a direct or endoscopic coronal lift. However, for patients who are concerned primarily about upper facial rejuvenation, the extended subperiosteal coronal lift is still the operation of choice.
In the senior author’s opinion, no other operation provides the elegant upper facial rejuvenation that is characteristic of this operation. This is especially true when there is an indication to correct a downward slope of the lateral canthal region. Although the technique of the extended subperiosteal coronal lift is beyond the scope of this chapter, it is important to understand that, when this operation is selected, lower facelifting must be sharply modified.
The plane of dissection for the subperiosteal lift extends down to the mandible, making it essential to avoid additional mid-face dissection when carrying out lower lifting. For this reason, when lower facelifting is combined with a subperiosteal lift, a biplane neck dissection is performed, but very little sub-cutaneous undermining is carried out in the face. A subperiosteal lift effectively lifts not only the upper face but also the midface; subcutaneous dissection in the cheek area is only necessary to remove redundant skin.
Regardless of the facelift technique used, there will always be some secondary relaxation. We suggest to all our lower facelift patients that they consider a secondary tuck (a mini-facelift) 12 to 24 months after the original surgery. When this secondary procedure is carried out, it is done under local anesthesia and involves reopening the incision around the ear, both anteriorly and posteriorly. Very limited undermining is carried out, and the skin is slightly advanced and excised.
The wound is subsequently closed in two layers, using 4–0 Monocryl and a running 6–0 plain gut. No dressings are applied, and patients are able to return to essentially normal activity the day after surgery. In spite of the limited undermining and advancement, it is remarkable how this procedure enhances the effect of the original operation.
Over the course of many years, we have had a considerable number of patients who have returned every few years for a secondary tuck, effectively eliminating the need for a second facelift. Because of the limited morbidity and risk associated with the procedure, we believe this technique deserves more widespread emphasis. Because of the network of subcutaneous scar tissue that has developed through the subcutaneous dissection of the facelift, this secondary tuck seems to provide a very strong and lasting lift that far exceeds what one would anticipate from so minor a procedure.
Since its introduction by Hamra,17 the term deep-plane facelift has been widely used. The term can be confusing because not every surgeon is following the technique as originally described by Hamra, but the term has generally come to be accepted as a type of facelift that is carried out in a plane deeper than the subcutaneous plane.
The term sub-SMAS is commonly used for this type of dissection, but we prefer to avoid use of the term SMAS , again because there is often confusion on the part of surgeons as to the precise meaning of this term. As one approaches the anterior border of the parotid, the SMAS becomes so thin as to become an almost microscopic layer. For that reason, we prefer to use the term musculofascial layer as described by Jost and Levet.16
When carrying out a deep-plane dissection, it is essentially the same as simply using the deeper plane of the biplane lift (see below). Although the deep-plane lift sacrifices some of the versatility of the biplane lift, it does offer an advantage of safety, as the subcutaneous flap is very limited and, in fact, after the excess skin is trimmed, it becomes nonexistent. For this reason, we tend to favor the deep-plane approach in patients who are smokers and diabetics, and increasingly for patients who are undergoing combined laser resurfacing with facelift. Because the biplane facelift is our workhorse operation, the technique is described in some detail.
Introduction to the Opportunistic Biplane Facelift
The biplane facelift described in this chapter is based on principles that increase aesthetics and longevity with limited morbidity. Facial aging is most pronounced from changes occurring in the deeper musculofascial plane that result in ptosis of the malar fat pad, jowl region, nasolabial folds, and neck. Precise elevation and rotation of this plane is accomplished using this biplane facelift technique. We call the operation “opportunistic,”; because there is no set anatomic limit to the deep-plane dissection. Rather, it is based on the concept of elevating tissue to the point where the flap can be easily advanced with the effect of providing adequate lift in the mid- and lower midface regions. Generally, this point is quite obvious. A rather sharp release is effected when sufficient elevation is accomplished, and the surgeon observes a marked lifting effect around the anterior cheek and the corner of the mouth.
Lifting the musculofascial flap anteriorly until adequate release is obtained allows the surgeon to obtain an improved lift with better control of the multivector pull necessary in this deeper plane of musculofascial tissue. We have not had any incidence of periauricular wound margin necrosis since adopting this technique. A natural appearance is achieved as a result of the deep multivector lift, with minimal skin tension after redraping.
The term opportunistic also applies to the concept of recognizing that, in some patients, the musculofascial layer becomes so attenuated as the dissection proceeds anteriorly that the resulting biplane flap would lack sufficient strength to provide adequate pull. In these cases, the surgeon wisely retreats and depends on plication for deeper support.
Tumescent anesthesia and fine cannula lipodissection, combined with electrocautery and laser dissection, all help minimize operative time (which averages hours) and postoperative morbidity. Because the primary lift is in the deeper plane, we have essentially eliminated skin excision in the temple and occipital regions. Skin bunching in the mastoid area subsides after a few weeks, resulting in a completely hidden scar within the hair and a decreased incidence of skin injury behind the ear. We depend entirely on the deeper pull for the effectiveness of the lift. Skin excision in front of the ear is very conservative. This has produced much better healing and finer scars because of the total absence of pull on the skin.
We have long abandoned postoperative drains or extensive head wraps and have seen no increase in postoperative hematomas. Our incidence of hematoma requiring surgical drainage was 2% (4 out of the past 200 cases) after biplanar facelifts without the use of drains or dressings, compared with a prior incidence of 4% when dressings had been routinely used. Part of the difference is attributable to the ability to recognize early small hematomas during recovery that can be treated conservatively by milking the flap, thus avoiding large hematomas when dressings are removed 24 hours after surgery. In addition, it appeared to us that hematomas would sometimes occur on removal of the drain and may have actually been caused by abrasion of the drain removal. Avoidance of dressings promotes patient comfort and may help avoid the swelling that can result from the tourniquet effect of compressive dressings.
Submusculofascial dissection has been reported to increase the risk of facial nerve injury; arguments have been made that plicating the SMAS is safer and as effective as the deeper plane techniques. In our experience, no permanent facial nerve injuries have occurred. There is no question that expert knowledge of the facial anatomic planes and neurovascular distribution is a requirement to avoid this complication with any facelifting techniques. Furthermore, our use of operating loops and laser dissection minimizes the risk of facial nerve injury. We expect to see the buccal nerve fibers during the course of dissection overlying the masseter muscle and, in fact, feel more comfortable when they are in view. Frequently, portions of the ramus mandibularis are seen as we begin dissection of the posterior platysma.
SMAS plication facelifts can improve facial aesthetics,18, 19but limited improvement is often seen in the malar and mandibular border due to the inability of this technique to free the restraining fibers (zygomatic and mandibular ligaments) in these regions. The biplane lift breaks these adhesions during the submusculofascial dissection. As mentioned, the “opportunistic”; description given to this lift is based on the concept of only dissecting far enough anteriorly to release the flap. Should poor flap quality (thickness or continuity) exist, the procedure can easily be converted to a simple SMAS plication procedure.
Biplane Facelift Technique
PREOPERATIVE MARKING
Initial marking is confined to outlining the incisions in the temple and in the mastoid region Figure 27-1). We begin by determining the proposed lift vector. A line is then drawn perpendicular to that vector, constituting the temporal and occipital ends of the facelift incision. These lines are marked with the patient sitting and before induction ofanesthesia. The remaining incisions can easily be marked in the operating room.
PREPARATION AND ANESTHESIA
Nearly all our surgery is carried out under endotracheal anesthesia, although it can be carried out using analeptic technique. The incisions in the scalp are prepared by shaving hair conservatively around the incision site.
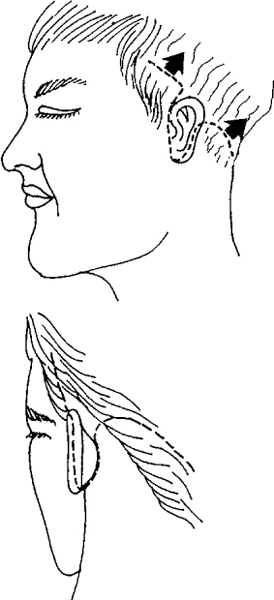
Figure 27—1 Location of incisions.
After the initial preparation, a modified tumescent infiltration is accomplished. We use a solution containing 250 ml of saline, 50 ml of 2% lidocaine, and 1 ml of 1:1000 epinephrine. The infiltration is facilitated by using a self-filling syringe in line with the tumescent solution. Infiltration is begun with the deep dermis of the temporal and occipital incision sites and then subcutaneously over the entire face and neck, with care taken to limit the injection to the subcutaneous plane in these areas. The layer between the temporoparietal and temporalis fascia is flooded to facilitate later blunt dissection in that area.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


