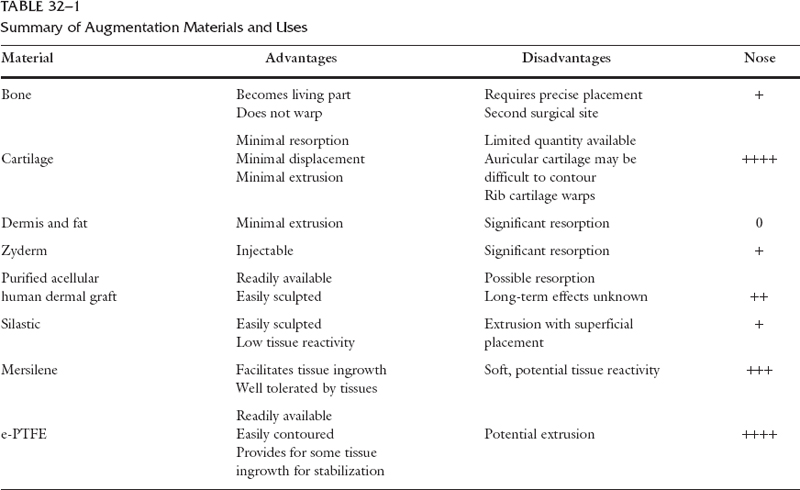
The use of implants in rhinoplasty is controversial. A variety of materials are commonly employed in nasal surgery for augmentation and for reconstruction. Autogenous tissue has long been advocated as the mainstay for nasal implants. Autogenous cartilage is most commonly employed for structural and augmentation grafting in the nasal tip, as well as for dorsal deformities. However, the limited availability and unpredictable resorption of both autologous and homologous implants have made newer alloplastic implants important considerations for dorsal augmentation. Selecting the most suitable graft or implant material for soft tissue augmentation is difficult. A wide variety of materials and techniques are employed by outstanding surgeons who have equally compelling arguments for the materials they use. No single material is suitable for all augmentation and nasal reconstruction situations. Each has its advantages and disadvantages (Table 32-1). The surgeon’s own experience and personal preference play a large role in the success of the material used. The indications for soft tissue augmentation in the nose are most commonly associated with depression over the cartilaginous or bony dorsum pyramid—the so-called saddle-nose deformity. This can occur to a variety of degrees and as the result of a variety of causes. This deformity can result from congenital abnormalities such as aplasia of the nasal bones. It can be secondary to trauma, which can produce septal hematoma and cartilaginous necrosis or disarticulation of the upper lateral cartilages and resulting in dorsal depression. It can also be the result of atrogenic causes, such as overresection of the quadrangular cartilage in septoplasty surgery. Studies have shown that 39% of patients undergoing extensive septal reconstructive surgery independent of rhinoplasty surgery exhibited some degree of external deformity with time. Cartilaginous saddle-nose deformity in the middle one-third of the nose is frequently the consequence of radical septal surgery. In a review of 153 revision rhinoplasties, Stucker1 noted that 58 patients presented with defects in the bony dorsum and 91 presented with defects of the cartilaginous vault. Approximately 20% of the defects would be classified as saddle-nose deformities requiring some degree of augmentation. Thus, augmentation of the bony or cartilaginous dorsum is not an infrequent consequence of rhinoplasty surgery. Types of Grafts The ideal graft to correct dorsal depressions would exhibit the following qualities: (1) host tolerance, (2) remain unaltered over time,(3) easily carved or molded, (4) no transillumination or discol-oration of supervening tissues, (5) pliable, and (6) easily obtainable. Grafts can be classified as autologous grafts (derived from the host’s own tissues), homologous grafts (derived from another individual of the same species), heterologous or xenografts (derived from a different species), and alloplastic or synthetic implants. Biological materials are called grafts. These living or nonliving tissues are incorporated into the host tissues or are completely replaced by the host tissues. Synthetic or alloplastic materials are synthetic organopolymers that are generally well tolerated by the host’s tissues. Synthetic materials are called implants. They retain their characteristic composition within the tissues. Although their structure may be invaded by host tissues, the implant structures are neither altered nor removed by the host.2 Autologous Grafts Autologous grafts have been the preferred choice for implants for nasal augmentation and reconstruction for more than a century.3 Many surgeons prefer to use the patient’s own septal cartilage as the implant of choice for nasal reconstruction.4, 5 This cartilage is particularly useful for tip support and tip augmentation. However, there is often a problem with availability. Alternative sources of autologous cartilage are the auricle and the rib. There are essentially two types of cartilage for grafting: morphologic and hyaline. Septal cartilage is an example of morphologic cartilage. It has the advantage of maintaining its shape when transplanted. Rib, or costal, cartilage is an example of hya-line cartilage. Hyaline cartilage has a system of interlocking stresses inherent in its molecular structure. There is a balance of internal elastic forces that resist deforming. The protein core and the glycosamine side chain are responsible for this property. Parallel lines of force run through the periphery of the cartilage and counteract the effects of the internal forces. Once the cartilage block is cut, the stress forces on that side of the cartilage are relieved, but they no longer counteract on the opposite side of the graft. This can result in warping of the implant and can be a disadvantage of its use. A technique can be used to minimize warping by shaving only scant amounts from the periphery of the graft, such that the outer restraining forces are not unfettered. Unlike bone, little remodeling of cartilage takes place in a normal state. Chondrocytes are not replaced during adult life. The ability of cartilage to regenerate remains questionable. Cartilage does enjoy some immunologic privilege. Cartilage cells possess antigens of the major H-antigen system. Cartilage grafts are antigenic and feebly immunologic because of the matrix proteoglycan that protects the chondrocyte from the afferent arm of the immune response, thereby preventing attack by immunoglobulins. Thus, there is no immune response or biocompatibility problem. Cartilage grafts, as compared with bone grafts, have been reported to have lower absorption rate and lower metabolic requirements for survival.6 Resorption rates of septal cartilage grafts have been estimated as ranging from 12% to 50%.7 However, resorbed cartilage is often replaced by host fibrous tissue, making resorption clinically undetectable. AUTOLOGOUS SEPTAL CARTILAGE GRAFTS Septal cartilage onlay grafts can be used to correct moderate saddle depressions. Sessions and Stallings8 reported only 15% resorption after 1 year’s experience with this technique. Gunter and Rohrich9 described an excellent technique of using septal cartilage as a frame graft and inserting autologous cartilage remnants underneath the frame to provide increased dorsal augmentation. AUTOLOGOUS AURICULAR CARTILAGE GRAFTS Autologous auricular cartilage grafts can be used when autologous septal cartilage is not available. Auricular cartilage has the disadvantage of requiring the use of a second surgical site. However, incisions can be made in the conchal cavum area with harvesting of the conchal cartilage bowl, which facilitates surgical access and is virtually undetectable when healed. Auricular cartilage can be contoured for use as onlay grafts; its curvature makes it extremely useful for reconstruction of the nasal valve. In contrast to alloplastic implants, auricular cartilage does not have to be buried deeply in soft tissue. Unlike bone, it does not have to be positioned in direct contact with bone or nasal cartilage. Whether it is advantageous to maintain perichondrium on the surface of the autologous auricular cartilage is debatable. However, it does add a degree of stiffness to the cartilage. As a cautionary note, beyond the age of 45 to 50 years, auricular cartilage becomes more brittle and is easily fractured. AUTOLOGOUS COSTAL CARTILAGE GRAFTS
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


