Increased thickness of the epithelium imparts a white appearance to the oral mucosa by increasing the distance to the underlying blood vessels. Usually this thickening is a result of the increased formation of keratin. Some other less common causes of white lesions are acanthosis or a thickening of the spinous cell layer, edema of the epithelium, or increased fibrosis of the connective tissue thereby reducing blood vessels. Occasionally the surface of an ulcer may appear white, due to collection of fibrin on the surface. In this article the authors discuss white lesions based on putative etiology, that is, hereditary, reactive, inflammation related, immunologic, traumatic, infection related, and idiopathic.
Increased thickness of the epithelium imparts a white appearance to the oral mucosa by increasing the distance to the underlying blood vessels. Usually this thickening is a result of the increased formation of keratin. Some other less common causes of white lesions are acanthosis or a thickening of the spinous cell layer, edema of the epithelium, or increased fibrosis of the connective tissue thereby reducing blood vessels. Occasionally the surface of an ulcer may appear white, due to collection of fibrin on the surface. In this article the authors discuss white lesions based on putative etiology, that is, hereditary, reactive, inflammation related, immunologic, traumatic, infection related, and idiopathic. Because many other lesions that may appear white have overlapping etiology and/or clinical nature (eg, candidiasis, carcinoma, smokeless tobacco associated lesions), they are discussed in other articles.
Developmental white lesions
Leukoedema
Leukoedema is a common developmental mucosal alteration of unknown cause, rather than a true pathologic change. Leukoedema is seen in 90% of all black adults and 50% of black teenagers. This condition has also been reported over a wide range in white adults (10%–90%) but the changes are far less pronounced. Tobacco smoking and chewing are reported to enhance the whiteness and extent of the lesion. Similar edematous changes have been seen in the mucosa of the larynx, the vagina, and other mucosal surfaces.
Clinical features
Leukoedema typically presents as a bilateral, diffuse, milky, gray-white asymptomatic area with numerous surface folds, on the buccal mucosa ( Fig. 1 ). Rarely it may involve the floor of the mouth and palatopharyngeal tissues. Mucosal changes start as early as age 3 to 5 years and by the end of the teen years, 50% of blacks present with mucosal alterations. An important diagnostic feature of leukoedema stems from its disappearance on stretching.
Histopathologic features
Epithelial hyperplasia with significant intracellular edema of the spinous cells, and broad and elongated rete ridges are evident. Keratinization of the surface is also noted.
Differential diagnosis
White sponge nevus, frictional keratosis, smokeless tobacco keratosis, and hereditary benign intraepithelial dyskeratosis.
Treatment
None indicated. No malignant changes have been reported.
White Sponge Nevus
White sponge nevus is a rare autosomal dominant disorder resulting from point mutation of either keratin 4 or keratin 13 genes. These mutations result in defective keratinization of the oral mucosa, with alterations that may also be seen in the nasal, esophageal, laryngeal, and anogenital mucosa. A high degree of penetration and variable expression is seen. White sponge nevus typically presents early in life and there is no gender predilection.
Clinical features
White sponge nevus presents as asymptomatic, white, soft and spongy bilateral plaques or macules, typically on the buccal mucosa, but other sites such as the lip, ventral surface of the tongue, and floor of the mouth may also be involved. Rare cases of mild discomfort due to secondary infections have been reported.
Histopathologic features
Parakeratosis, marked epithelial thickening, and intracellular edema with perinuclear condensation of keratin is seen. Clear cell changes begin at the parabasalar layer and extend close to the surface.
Differential diagnosis
Leukoplakia, candidiasis, pachyonychia congenita, hereditary benign intraepithelial dyskeratosis, Darier disease, dyskeratosis congenita, lichen planus, lupus erythematosus, chemical burns, and syphilis.
Treatment
None indicated. No malignant changes seen. Treatment of the condition with topical tetracycline has been reported.
Hereditary Benign Intraepithelial Dyskeratosis
Hereditary benign intraepithelial dyskeratosis (HBID) is a rare autosomal dominant disease exhibiting incomplete penetration, characterized by early onset of bulbar conjunctivitis preceded by bilateral gelatinous plaques and asymptomatic oral lesions. Also known as Witkop disease, HBID is primarily seen among the descendents of a triracial isolate of whites, Indians, and African Americans in North Carolina. HBID usually presents at birth or early childhood. Recent studies have linked the gene responsible for HBID to chromosome 4 (4q35).
Clinical features
Oral lesions of HBID are usually asymptomatic and present as white spongy macules or plaques seen on the buccal and labial mucosa, lateral tongue, floor of the mouth, gingiva, and palate, very similar to those seen in white sponge nevus. These lesions usually intensify until the mid-teens, after which they stabilize. The ocular lesions of HBID are particularly interesting; they develop early in life and may vary seasonally. These gelatinous plaques are seen bilaterally on the bulbar conjunctiva. Unlike the oral lesions, ocular lesions are frequently symptomatic. Tearing, redness of the eyes, photophobia, and itching are commonly encountered during the active phase. Blindness has also been reported as a result of vascularization of the cornea.
Histopathologic features
Microscopic similarities are seen between oral and ocular lesions. Marked epithelial keratosis and acanthosis are seen. A dyskeratotic process in the form of enlarged hyaline keratinocytes is seen in the upper half of the epithelium. Some of the cells appear to be “engulfed” by surrounding cells forming a “cell within a cell” pattern. The lower half of the epithelium appears normal, with a well-defined epithelium-connective tissue interface.
Differential diagnosis
Leukoedema, dyskeratosis follicularis, focal epithelial hyperplasia, hereditary mucoepithelial dyskeratosis, leukoplakia, and white sponge nevus.
Treatment
None indicated for oral lesions because this is a self-limiting benign condition with no malignant potential. Patients with symptomatic ocular lesions should be referred to an ophthalmologist for surgical removal of the plaques. However, these plaques tend to recur.
Dyskeratosis Congenita
Dyskeratosis congenita is a rare inherited disorder characterized by mucosal leukoplakia, nail dystrophy, and hyperpigmentation of the skin. Although it exhibits autosomal dominant, autosomal recessive, or x-linked inheritance patterns, most cases are of the x-linked form. Mutation of the DKC1 gene has been determined to be the cause of the x-linked form. The condition manifests itself during the first decade of life. Patients with this disorder are susceptible to developing bone marrow failure as well as malignant transformation of oral and skin lesions. Hence identification of the condition is important for early referral and appropriate treatment. Oral leukoplakic lesions are seen in 80% of cases. These lesions are seen most frequently on the tongue but can also involve the buccal mucosa, lingual mucosa, and palate.
Clinical features
Oral lesions begin with bullae formation on affected surfaces, followed by erosion and finally leukoplakic plaques. Superimposed candidal infection is often seen. Discomfort may be associated with the consumption of spicy and hot foods. The oral lesions are considered to be premalignant and may transform to malignancy over a 10- to 30-year period. Squamous cell carcinoma is the most common malignancy to arise in these lesions. Skin and nail changes increase with age. The most significant clinical manifestation of the disease is bone marrow failure. By the second decade of life patients typically develop anemia, and 94% of patients develop bone marrow failure by the age of 40 years.
Histologic features
Early lesions display hyperkeratosis with epithelial dysplasia, and frank malignant changes are seen eventually as the lesion develops.
Differential diagnosis
Leukoplakia, white sponge nevus, lichen planus, dyskeratosis congenita, candidiasis, hyperkeratosis, epithelial dysplasia, early invasive squamous cell carcinoma, thrombocytopenia, and aplastic anemia.
Treatment
Periodic examination of oral lesions to monitor malignant changes and avoidance of smoking and drinking are of utmost importance. Current treatment for bone marrow failure is allogenic hematopoietic stem cell transplantation. Prognosis is guarded.
Pachyonychia Congenita
Pachyonychia congenita is a rare autosomal dominant disorder mainly characterized by nail dystrophy, subungual and palmoplantar hyperkeratosis, and oral leukoplakic lesions. Two major subtypes include pachyonychia congenita type 1 (Jadassohn-Lewandowsky form) and pachyonychia congenita type 2 (Jackson-Lawler form). Oral lesions characterized by leukoplakic lesions of the tongue and buccal mucosa as well as dental abnormalities in the form of neonatal teeth are seen only on pachyonychia congenita type 1. Mutations of keratin 16 gene and keratin 17 gene have been implicated as the cause of pachyonychia congenita type 1 and pachyonychia type 2, respectively. The condition manifests itself at birth or very early in life. Cases of late onset, called pachyonychia tarda, have also been reported.
Clinical features
Nail changes are the most outstanding feature, and changes are typically seen at birth. Palmoplantar and follicular keratosis are observed. Oral leukoplakic lesions seen on the tongue, buccal mucosa, or rarely the gingiva are not precancerous.
Histologic features
Mild to moderate hyperkeratosis and acanthosis of the epithelium are evident.
Differential diagnosis
Leukoplakia and focal palmoplantar keratodermas.
Treatment
None indicated for oral lesions, as there is no malignant potential. General treatment forms are directed at symptom relief, and there is no satisfactory treatment regimen to date.
Reactive inflammatory lesions
Physical and Chemical Injuries
Linea alba
Linea alba is a very common oral finding characterized by a white line on the buccal mucosa at the level of the occlusal surface of teeth, and extends from the commissure to as far back as the molar teeth. It is often bilateral ( Fig. 2 ). This condition is related to pressure or sucking trauma from teeth on the buccal mucosa. According to one study its incidence is seen in up to 13% of the population. Linea alba is typically restricted to teeth-bearing areas of the buccal mucosa.

Clinical features
Linea alba usually presents as asymptomatic, bilateral linear white lines, which may be scalloped and may be more intense in the posterior region.
Histologic features
Hyperkeratosis overlying normal mucosa is seen.
Differential diagnosis
Frictional keratosis and cheek chewing.
Treatment
None indicated. Condition may regress spontaneously in some cases.
Frictional, chemical, and thermal keratosis
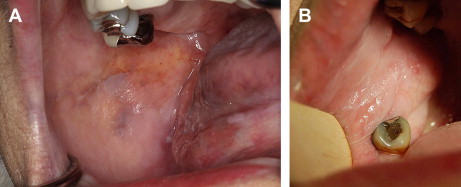
These lesions are characterized as white plaques that arise as a result of an identifiable source and usually resolve once the causative factor is eliminated. The sources of friction resulting in hyperkeratosis may be an ill-fitting denture, malocclusion, parafunctional habits ( Fig. 3 A), or poor brushing techniques. Frictional keratosis is usually seen in young adults. Lips, lateral surface of tongue, and buccal mucosa are common sites.
Thermal keratosis can be due to thermal burns in the oral cavity caused by excessively hot (microwaved) foods or heat generated from smoking. Lesions are commonly seen on the tongue and palate. Nicotine stomatitis is a tobacco-related form of keratitis causing both chemical and thermal keratosis. Heat and carcinogens are the causative factors.
Chemicals causing burning of the mucosa and resultant hyperkeratosis include aspirin, sodium hypochlorite, hydrogen peroxide, formocresol, paraformaldehyde, cavity varnish, or mouthwashes, to name a few. Lesions are typically located on the mucobuccal fold or the gingiva.
Clinical features
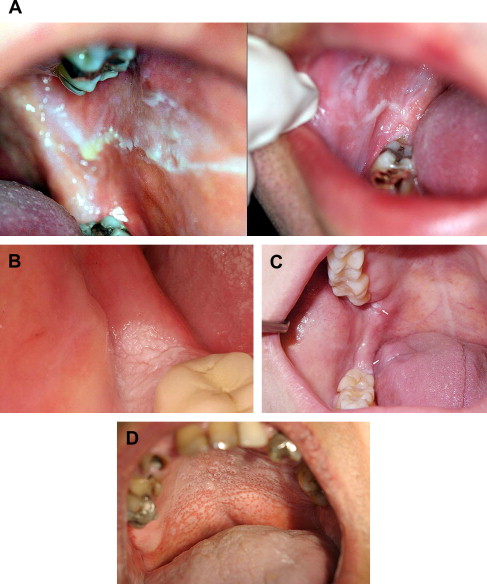
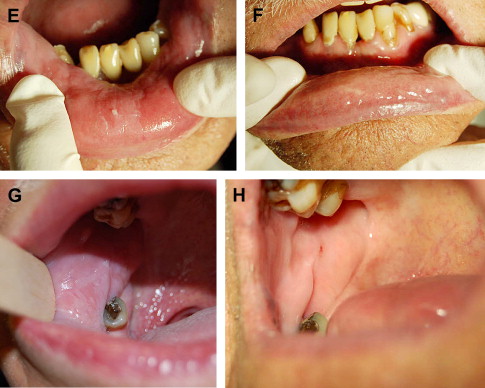
Frictional keratosis is typically characterized by a poorly demarcated rough area, which can be peeled off occasionally, leaving focal areas of pink mucosa (see Fig. 3 A). Masticatory trauma often results in thick white corrugated lesions on the retromolar pad areas (see Fig. 3 B and C). Trauma from mastication or sharp cuspal edges of teeth may also cause similar lesions. Thermal keratosis is characterized by a white lesion with focal areas of ulceration associated with mild to moderate pain. Nicotine keratosis causes opacification of the hard palate with red punctuate spots representing inflamed and metaplastically altered salivary duct openings (see Fig. 3 D). Chemical keratosis is characterized by a white, irregularly shaped, asymptomatic or variably symptomatic lesions (see Fig. 3 E–H). Thermal and chemically induced lesions are almost always painful.
Histologic features
Fractional keratosis lesions simply exhibit hyperkeratosis and acanthosis with fraying and shredding of the keratin layers. These lesions do not show any epithelial dysplasia. Chemical and thermal keratoses display a superficial pseudomembrane composed of necrotic tissue and an inflammatory exudate.
Differential diagnosis
Leukoedema, leukoplakia, candidiasis, white sponge nevus, dysplasia, carcinoma in situ, squamous cell carcinoma, oral hairy leukoplakia, and lupus erythematosus.
Treatment
Removal of the causative factor leads to resolution of the lesions (see Fig. 3 G and H). These lesions do not show any malignant potential.
Uremic stomatitis
Uremic stomatitis is a rare oral manifestation of advanced renal failure, typically characterized by an abrupt onset of adherent white plaques on the ventral and dorsal surfaces of the tongue, floor of the mouth, buccal and labial mucosa, as well as the gingiva. The etiology is still unclear but it has been suggested that salivary urease hydrolyzes urea in saliva and converts it into ammonia and its compounds, which in turn cause mucosal irritation and burn, resulting in oral lesions.
Clinical features
Four forms have been described: erythemopultaceous (characterized by the formation of a pseudomembrane), ulcerative, hemorrhagic, and hyperkeratotic. Some patients complain of severe burning pain in the lips and tongue, and an unpleasant taste. Patients’ breath may be laced with the smell of urea and ammonia. Lesions may be seen anywhere in the oral mucosa ( Fig. 4 ).

Histologic features
Hyperkeratotic-type lesions demonstrate hyperkeratosis and acanthosis of the epithelial layer. Ballooning keratinocytes are also seen with minimal inflammatory infiltrate in the underlying connective tissue. Ulcerative-type lesions demonstrate epithelial necrosis and a dense inflammatory infiltrate in the underlying connective tissue.
Differential diagnosis
Frictional keratosis, leukoplakia, carcinoma, and oral hairy leukoplakia.
Treatment
Lesions resolve with the lowering of blood urea nitrogen (BUN) levels and treatment of renal failure. Because calculus may contain urease, scaling of teeth may be of help. Hydrogen peroxide mouthwashes have also been shown to resolve the lesions.
Reactive inflammatory lesions
Physical and Chemical Injuries
Linea alba
Linea alba is a very common oral finding characterized by a white line on the buccal mucosa at the level of the occlusal surface of teeth, and extends from the commissure to as far back as the molar teeth. It is often bilateral ( Fig. 2 ). This condition is related to pressure or sucking trauma from teeth on the buccal mucosa. According to one study its incidence is seen in up to 13% of the population. Linea alba is typically restricted to teeth-bearing areas of the buccal mucosa.
Clinical features
Linea alba usually presents as asymptomatic, bilateral linear white lines, which may be scalloped and may be more intense in the posterior region.
Histologic features
Hyperkeratosis overlying normal mucosa is seen.
Differential diagnosis
Frictional keratosis and cheek chewing.
Treatment
None indicated. Condition may regress spontaneously in some cases.
Frictional, chemical, and thermal keratosis
These lesions are characterized as white plaques that arise as a result of an identifiable source and usually resolve once the causative factor is eliminated. The sources of friction resulting in hyperkeratosis may be an ill-fitting denture, malocclusion, parafunctional habits ( Fig. 3 A), or poor brushing techniques. Frictional keratosis is usually seen in young adults. Lips, lateral surface of tongue, and buccal mucosa are common sites.
Thermal keratosis can be due to thermal burns in the oral cavity caused by excessively hot (microwaved) foods or heat generated from smoking. Lesions are commonly seen on the tongue and palate. Nicotine stomatitis is a tobacco-related form of keratitis causing both chemical and thermal keratosis. Heat and carcinogens are the causative factors.
Chemicals causing burning of the mucosa and resultant hyperkeratosis include aspirin, sodium hypochlorite, hydrogen peroxide, formocresol, paraformaldehyde, cavity varnish, or mouthwashes, to name a few. Lesions are typically located on the mucobuccal fold or the gingiva.
Clinical features
Frictional keratosis is typically characterized by a poorly demarcated rough area, which can be peeled off occasionally, leaving focal areas of pink mucosa (see Fig. 3 A). Masticatory trauma often results in thick white corrugated lesions on the retromolar pad areas (see Fig. 3 B and C). Trauma from mastication or sharp cuspal edges of teeth may also cause similar lesions. Thermal keratosis is characterized by a white lesion with focal areas of ulceration associated with mild to moderate pain. Nicotine keratosis causes opacification of the hard palate with red punctuate spots representing inflamed and metaplastically altered salivary duct openings (see Fig. 3 D). Chemical keratosis is characterized by a white, irregularly shaped, asymptomatic or variably symptomatic lesions (see Fig. 3 E–H). Thermal and chemically induced lesions are almost always painful.
Histologic features
Fractional keratosis lesions simply exhibit hyperkeratosis and acanthosis with fraying and shredding of the keratin layers. These lesions do not show any epithelial dysplasia. Chemical and thermal keratoses display a superficial pseudomembrane composed of necrotic tissue and an inflammatory exudate.
Differential diagnosis
Leukoedema, leukoplakia, candidiasis, white sponge nevus, dysplasia, carcinoma in situ, squamous cell carcinoma, oral hairy leukoplakia, and lupus erythematosus.
Treatment
Removal of the causative factor leads to resolution of the lesions (see Fig. 3 G and H). These lesions do not show any malignant potential.
Uremic stomatitis
Uremic stomatitis is a rare oral manifestation of advanced renal failure, typically characterized by an abrupt onset of adherent white plaques on the ventral and dorsal surfaces of the tongue, floor of the mouth, buccal and labial mucosa, as well as the gingiva. The etiology is still unclear but it has been suggested that salivary urease hydrolyzes urea in saliva and converts it into ammonia and its compounds, which in turn cause mucosal irritation and burn, resulting in oral lesions.
Clinical features
Four forms have been described: erythemopultaceous (characterized by the formation of a pseudomembrane), ulcerative, hemorrhagic, and hyperkeratotic. Some patients complain of severe burning pain in the lips and tongue, and an unpleasant taste. Patients’ breath may be laced with the smell of urea and ammonia. Lesions may be seen anywhere in the oral mucosa ( Fig. 4 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


