Voice: Anatomy, Physiology, and Clinical Evaluation
Lucian Sulica
The Larynx is a biologic valve located at the junction of the respiratory and the digestive tracts. Its evolutionary origins lie in the need to protect the lungs of amphibious organisms from water, and airway protection remains its most important biologic task. The development of the larynx into a phonatory organ arose because its position atop the tracheobronchial tree and its valving function gave it a unique ability to regulate expiratory airflow. Human voicing is the result of complex interactions among all of the elements of the upper aerodigestive tract, but it depends on precise and finely modulated glottic closure for sound.
The human larynx has a number of features that are specially adapted to its role as a sound source, including unique tissues capable of sustained high-speed oscillation and neuromotor specializations for fine control of vocal fold movement. As laryngology grows increasingly sophisticated and ambitious, especially with regard to restoration and even enhancement of voice quality, these details of anatomy and physiology have taken on a new clinical relevance. Increased insight into these has developed hand in hand with a better appreciation of factors leading to dysphonia. To be most effective, the otolaryngologist must understand all of these elements—anatomy, physiology, and clinical evaluation as a reflection of both—as an integrated whole that forms the foundation of any effort to treat the patient with a voice disorder.
ANATOMY
The Laryngeal Framework
The supporting framework of the larynx consists of one bone, the hyoid, and four cartilages: the cricoid, thyroid, and paired arytenoids (Fig. 65.1). The external framework is formed by the hyoid, the thyroid, and the cricoid, linked together by the thyrohyoid and cricothyroid membranes. All of these elements are suspended from the skull base and mandible by means of soft tissue attachments. The mylohyoid, the geniohyoid, the hyoglossus, and the stylohyoid muscles; the stylohyoid ligament; and the sling of the digastric insert into the superior aspect of the hyoid and exert cephalad traction. This is counterbalanced by the caudad pull of the omohyoid, sternohyoid, thyrohyoid, and sternothyroid muscles, all except the last inserting into the hyoid as well. The larynx thus moves vertically as a unit, dependent from the hyoid, its most superior element. This displacement is important not only in protecting the airway during swallowing but also in modifying the shape of the supraglottal resonating tract in voice production.
The cricoid cartilage may be considered the base of the larynx. As the only complete ring in the entire airway, it is particularly important in maintaining airway patency. However, the rigidity of this segment appears to predispose it to mucosal injury from endoluminal pressure, such as that from an endotracheal tube cuff and consequent stenosis. The thyroid cartilage rests atop the cricoid. Its inferior horns articulate with the outer surface of the cricoid posteriorly, and its V-shaped body envelops the soft tissue of the glottis. The angle at which the two halves of the thyroid cartilage join at the anterior midline is more acute in men than in women, and this accounts for its increased prominence in the male neck.
The paired arytenoids rest on the cephalic rim of the posterior cricoid and are the anchors for the mobile ends of the vocal folds, each one stretching from an anterior projection known as the vocal process to the anterior midline of the thyroid cartilage, just below the root of the epiglottis. Functionally, the arytenoid serves to translate the vectors of force of all of the individual intrinsic laryngeal muscles (but for the cricothyroid) into adductory and abductory vocal fold motion. Its eccentric shape is well suited to the task. A posterolateral projection from its body constitutes its muscular process, receiving insertions from both the lateral cricoarytenoid and the posterior
cricoarytenoid muscle and acting as a lever to amplify their actions. Its anterolateral face offers a broad attachment for the thyroarytenoid muscle, which functions to adduct and shorten the vocal fold. Scalloped facets face one another on the posteromedial surfaces of the arytenoids and house the attachments of the adductory interarytenoid muscle. The anteriorly projecting vocal process finally converts the action of laryngeal muscles into vocal fold motion.
cricoarytenoid muscle and acting as a lever to amplify their actions. Its anterolateral face offers a broad attachment for the thyroarytenoid muscle, which functions to adduct and shorten the vocal fold. Scalloped facets face one another on the posteromedial surfaces of the arytenoids and house the attachments of the adductory interarytenoid muscle. The anteriorly projecting vocal process finally converts the action of laryngeal muscles into vocal fold motion.
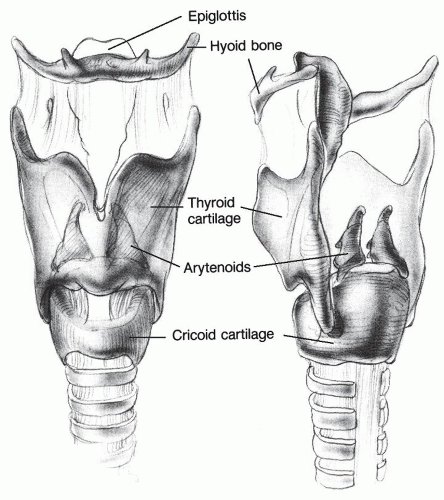 Figure 65.1 Laryngeal framework. |
The epiglottis, an elastic cartilage that has no structural role in the adult, is secured to the supporting elements of the larynx by means of the thyroepiglottic and hyoepiglottic ligaments. It is passively deflected to hood the laryngeal introitus during swallowing and serves as an accessory barrier to laryngeal entry. Finally, small cartilages of indeterminate and probably inconsequential function are found about the superior rim of the larynx. The corniculate cartilages (of Santorini) rest atop the arytenoid apices, and cuneiform cartilages (of Wrisberg) are contained within the superior rim of the aryepiglottic fold just anterolateral to the arytenoid mound. Whatever height and rigidity these may add to the aryepiglottic rim is probably not functionally significant in humans. Triticeal cartilages are sometimes found at the posterior border of the thyrohyoid membrane and are significant only because they may be mistaken for a foreign body on radiography.
In addition to bony and cartilaginous elements, two fibroblastic membranes are structurally important in the larynx (Figs. 65.2 and 65.3). The conus elasticus originates on the upper border to the cricoid cartilage and rises to the glottic aperture. Superiorly, its thickened free edges form the vocal ligaments. The conus elasticus defines the convergent shape of the subglottis, which is of considerable physiologic importance in phonation. The supraglottic quadrangular membrane extends inferiorly from the aryepiglottic fold to the leading edge of the ventricular folds, similar to an inverted conus elasticus in shape, although not in functional importance. Both the conus and the quadrangular membrane, in addition to supporting the shape of the vocal fold and the ventricular fold, respectively, are barriers that may influence the spread of malignant disease.
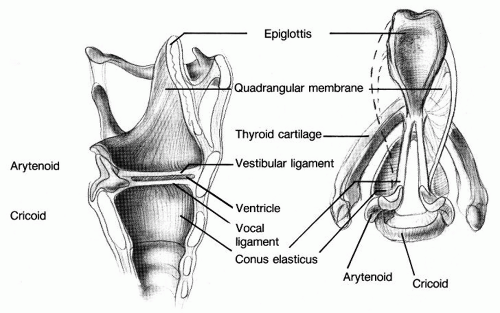 Figure 65.2 Fibroelastic membranes. |
Covered on the outside only by strap muscles and skin, the external bony and cartilaginous elements of the larynx are usually easily palpable. The most prominent points are the anterior arch of the cricoid and the superior notch of the thyroid in the anterior midline, and laterally,
the superior horns of the thyroid and greater horns of the hyoid. From these landmarks, the location of most of the structures of the larynx can be extrapolated for purposes of manipulation, placement of surgical incisions, electromyography, injection, or other intervention. Tethered above and below by the strap muscles, the normal larynx may usually be rotated or displaced from side to side without difficulty or much discomfort. The latter motion normally produces a crepitus that is felt by the examiner’s hand and the patient rather than heard and that results from the cartilaginous structures of the larynx sliding over the bony elements of the cervical spine.
the superior horns of the thyroid and greater horns of the hyoid. From these landmarks, the location of most of the structures of the larynx can be extrapolated for purposes of manipulation, placement of surgical incisions, electromyography, injection, or other intervention. Tethered above and below by the strap muscles, the normal larynx may usually be rotated or displaced from side to side without difficulty or much discomfort. The latter motion normally produces a crepitus that is felt by the examiner’s hand and the patient rather than heard and that results from the cartilaginous structures of the larynx sliding over the bony elements of the cervical spine.
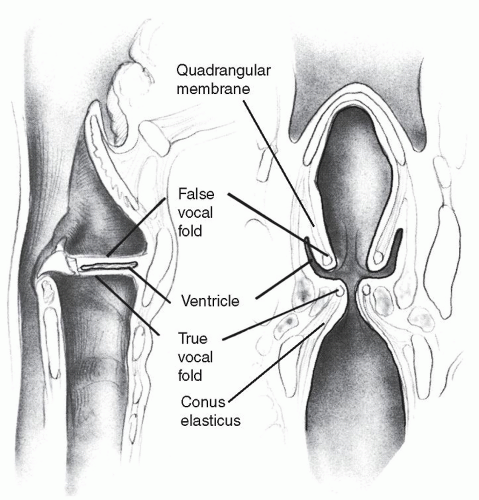 Figure 65.3 Vertical section through the larynx. |
The nature of the articulations of the laryngeal cartilages determines the range and trajectory of motion of the vocal folds and are thus worth some attention. Each cricothyroid joint consists of a shallow articulatory facet that seats the tuberculum of the inferior horn of the thyroid cartilage. These paired structures permit a rotatory motion between the thyroid and the cricoid cartilage, resulting in a visorlike approximation of their anterior portions on cricothyroid muscle contraction. As the anterior arch of the cricoid rises, the posterior plate drops, carrying with it the arytenoids. In consequence, the vocal folds lengthen and thin, which is a principal method of increasing phonatory pitch. The ligaments of the cricothyroid joint also seem to permit a ventrodorsal sliding motion, particularly when the articular facet on the cricoid cartilage is poorly defined or absent, as may be the case in as many as 70% of larynges (1). This sliding might account for as much as 40% of the increase of vocal fold length on cricothyroid contraction.
The cricoarytenoid joint is the principal articulation for vocal fold adduction and abduction. Arytenoid cartilage motion is sometimes presented as simple rotation around a vertical or helical axis, although it has long been known to be more complex. This oversimplification is likely the result of two factors. First, available means of clinical examination of the larynx, which renders vertical height differences between the vocal folds notoriously difficult to assess, create the impression of vocal fold motion in a single plane. Second, this misperception was of little or no practical consequence prior to relatively recent advances in laryngeal framework surgery.
Accounts also generally break down arytenoid motion into three axes, but this creates an artificially fragmented notion of the movement, which according to all evidence is smooth across its entire trajectory.
The arytenoid rests atop a convex articular surface on the cephalic edge of the cricoid. The joint surface faces more laterally at its posterior end and rotates superiorly as it extends anteriorly (2). It functions as a slipway for motion of the arytenoid body. The arytenoid body thus shifts anteromedially as it is pulled closed but posterolaterally when pulled open. The first motion depresses the vocal process, so that its adduction is not only medial but also inferior. Conversely, its abduction is lateral and superior, so that the vocal fold does not move into the body of the thyroarytenoid muscle but upward toward the ventricle. Vertical vocal process displacements, measured in cadavers, range up to 2.4 mm. The cricoarytenoid joint facets and consequently the paths of motion of the vocal process are often not symmetric, which should warn us against ascribing pathologic significance to small asymmetries of vocal fold motion. Wang (2) has noted correctly that symmetry is of functional importance only when the vocal folds are in adduction.
Understanding the three-dimensional nature of vocal fold motion is important to clinical evaluation and rehabilitation of glottic insufficiency because a denervated vocal fold may rest at any point along its normal sweep (3,4). (The classic terms for the position of an immobile vocal fold—median, paramedian, cadaveric, etc.—are purely descriptive; they have no physiologic or topognostic significance, contrary to time-honored belief.) In fact, with muscle traction diminished or even absent, it may even lie outside of this trajectory, as in the case of a so-called prolapsed arytenoid, when the vocal process may lie below the inferiormost extent of normal motion. Laryngoscopy may not readily reveal the height difference, and simple medialization, like that achieved by a thyroplasty implant alone, may not approximate the vocal folds at the same level.
The cricoarytenoid joint is remarkably stable for a structure that permits so many degrees of freedom in arytenoid motion. Dissection has revealed a layered network of articulatory ligaments that provide substantial stability in most directions. Multiple muscular and ligamentous attachments must be severed to produce subluxation (2). In cadaver experiments, even without active muscular support, the joint is extremely resistant to dislocation, both by endotracheal tube and direct manual manipulation (5,6). Available evidence suggests that cricoarytenoid joint dislocation is a very rare clinical condition.
Muscles and Nerves
The intrinsic muscles of the larynx—those that originate and insert on the laryngeal cartilages—are responsible for vocal fold motion (Fig. 65.4). The sole abductor of the vocal fold is the posterior cricoarytenoid muscle, which reaches from the posterior surface of the cricoid superolaterally to the muscular process of the arytenoid. Its principal antagonist is the thyroarytenoid muscle, which stretches from the inner surface of the thyroid to the arytenoid body. Together with the lateral cricoarytenoid muscle, it forms the principal adductory muscle complex of the vocal fold. It is aided in adduction by the interarytenoid, which is the only nonpaired laryngeal muscle. The thyroarytenoid also shortens the vocal folds by means of anterior traction on the arytenoid. The cricothyroid muscle, stretching from the external anterior surface of the cricoid to attach broadly on the caudal rim of the thyroid, functions as an antagonist to the thyroarytenoid in this respect. It elongates the vocal folds by effecting torsion at the cricothyroid joint, as
we have already seen. Minor aryepiglottic muscles, as well as a cephalad projection of the thyroarytenoid, serve to constrict the ventricular folds and supraglottic structures, which are accessory means of glottic valving that usually come into play during voicing only under pathologic circumstances.
we have already seen. Minor aryepiglottic muscles, as well as a cephalad projection of the thyroarytenoid, serve to constrict the ventricular folds and supraglottic structures, which are accessory means of glottic valving that usually come into play during voicing only under pathologic circumstances.
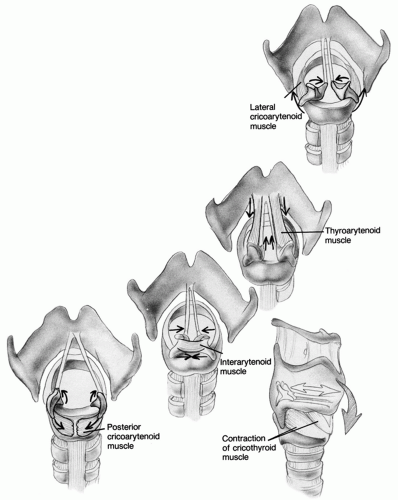 Figure 65.4 Intrinsic laryngeal muscles. |
There is considerable evidence that the thyroarytenoidlateral cricoarytenoid muscle complex, the posterior cricoarytenoid muscles, and the cricothyroid muscles are divided into functionally separate compartments distinguished by fascial barriers and corresponding arborization patterns of laryngeal nerves (7,8,9,10). This impression is reinforced by differences in the concentration of muscle fiber types and specialized proprioceptors among these compartments (11). For instance, the medial division of the thyroarytenoid, known as the vocalis, contains fatigue-resistant slowtwitch fibers (12). These imply that it is especially suited to activity that requires fine-tuned tonic contraction, such as phonation. In contrast, the lateral compartment has a high concentration of fast-twitch fibers, better suited to rapid movement, such as that demanded by reflexive glottic closure for airway protection. A similar difference exists between the horizontal and the vertical compartments of the posterior cricoarytenoid. No muscle fiber distinctions seem to exist among the two compartments of the cricothyroid, but each exerts a different vector of force on the cricothyroid joint by virtue of differences in fiber origin, insertion, and direction (10,13).
Each hemilarynx receives its innervation from ipsilateral branches of the vagus. The superior laryngeal nerve arises from the bottom half of the nodose ganglion, about 36 mm below the jugular foramen (14). It travels medial to both the internal and external carotid arteries and splits into two branches after some 15 to 20 mm. The internal branch pierces the thyrohyoid membrane in company with the superior thyroid artery and ramifies to the mucosa of the ipsilateral laryngeal mucosa by means of a variable number of branches. The external branch runs lateral to the inferior constrictor muscle until it curves anteriorly at approximately the level of the inferior edge of the thyroid lamina to reach the cricothyroid muscle. Its path in relation to the apex of the thyroid lobe and its blood supply is of obvious clinical significance. Most nerves cross the superior thyroid artery well away from the superior pole of the thyroid. However, up to 30% cross that vessel within 1 cm of the gland, and up to 20% actually pass under the gland itself, representing the situation of considerable risk during thyroidectomy (15,16).
On the right side, the recurrent nerve arises from the main trunk of the vagus as it passes anterior to the subclavian artery and loops underneath that structure to travel toward the larynx. For purposes of investigation of rightsided vocal fold paralysis, it is important to understand that the course of the nerve can thus extend into the superior mediastinum; diagnostic imaging studies should not be restricted strictly to the neck. The left-sided nerve follows a similar path but loops around the aorta instead of the subclavian artery, as the result of differences in embryologic vascular development from one side to the other (17). These pathways in large part determine the vulnerability of each nerve to injury, be it from surgical manipulation, tumor compression, or other disease.
Classic descriptions hold that the recurrent nerve supplies motor input to all of the intrinsic muscles but for the cricothyroid, which receives its innervation from the external branch of the superior laryngeal nerve. Sensory information from the level of the glottis and above travels to the central nervous system via the internal branch of the superior laryngeal nerve and from below the glottis via the recurrent laryngeal nerve. This view, although essentially correct, may not capture the full complexity of the neuromuscular system of the larynx. Historically, the ansa of Galen, an extension of a branch of the internal branch of the superior laryngeal nerve running underneath the mucosa of the medial wall of the piriform sinus, has been regarded as the only anastomosis between the superior and recurrent laryngeal nerves. By means of neurospecific stains, inconsistent but relatively common connections have been found between the external branch of the superior nerve and the recurrent nerve within the thyroarytenoid muscle (7,18,19). Some investigators have asserted that the bilaterally innervated interarytenoid muscle contains anastomosis between the contralateral nerve populations, which may include contributions from the internal branch of the superior nerve (20,21).
The precise physiologic significance of such insights into nerve and muscle anatomy remains to be determined, but traditional concepts of laryngeal anatomy are being revised by an increased appreciation for fine muscular specialization and for the possibility of a more complex scheme of innervation, featuring more anastomotic pathways than previously suspected, interdigitating nerve branches, and terminal plexuses. This evolving picture may help to explain not only the robust tendency for reinnervation in the human larynx but also why such innervation is so often dysfunctional and why dynamic surgical reinnervation remains such a challenging clinical problem.
The Membranous Vocal Fold
The paired shelves of tissue formed by the thyroarytenoid muscles and their soft tissue cover, which extend from the vocal process of the arytenoids to the anterior midline of the thyroid cartilage, are known as the vocal folds. These form the principal valve for glottic closure and, of special interest to us, for glottic resistance necessary for phonation. This latter function is dependent on the unique and delicate microarchitecture of the leading edge of the vocal fold (Fig. 65.5).
The vocal fold is covered by a thin layer of stratified squamous epithelium, in contrast to the respiratory epithelium of other surfaces of the larynx and trachea. Below this lies the lamina propria, a pliable layer of fibrous proteins, including elastin, collagen, and other extracellular elements, which together account for its unique biomechanical properties. A sparse cell population composed principally of fibroblasts, thought to be responsible for the production and regulation of the components of the lamina propria, is also present (22




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
