Management of the Crooked Nose
Craig S. Murakami
Richard A. Zoumalan
The treatment of a crooked nose remains one of the most challenging problems in rhinoplasty surgery. Inadequate treatment can cause a persistent cosmetic deformity as well as problems with nasal obstruction. There are many techniques currently available for correction of the crooked nasal deformity. Regardless of the method used, revision rates remain significantly high. Patients differ in their goals for surgery, and it is essential that the surgeon understand their needs. While some patients are focused on the aesthetic outcome, others are more concerned with functional improvement. More commonly, patients have a combination of cosmetic and functional concerns.
ETIOLOGY
The crooked nose can be due to congenital, traumatic, or iatrogenic etiologies. A congenitally crooked nose is often associated with overall facial asymmetry. Sometimes the asymmetry is associated with a known syndrome. However, most patients have mild asymmetry that is nonsyndromic. The patient should be informed about these facial asymmetries preoperatively and made aware of how this may or may not affect their outcome. Treatment of the congenitally crooked nose can be difficult since the surrounding deviation of the internal and external facial framework makes it difficult to find a common midline.
Traumatic crooked noses can be the result of a low velocity force that causes a simple unilateral infracturing of the affected nasal wall or a higher velocity force that causes bilateral nasal wall deviations along with deviation of the septum. Severe nasal injuries may also be associated with deformities of the orbits or maxilla.
Iatrogenic crooked nasal deformities caused by previous surgery may be the result of poorly executed osteotomies, excessive resection of bone or cartilage, and/or poor wound healing. The nose can sometimes heal in unpredictable ways due to the effects of soft tissue contracture, cartilage memory, severe bone and cartilage asymmetries, aging, glasses, gravity, and so on.
A severely deviated nose almost always has a major septal deformity. Treating the deviated internal septum is usually necessary to facilitate correction of the deviated external nasal component (1, 2, 3). The nasal septum has a syndesmosis between the quadrangular cartilage and bones of the vomer and ethmoid that is unique in the human body. Cartilage growth occurs in the perichondrium of the anterior bony septum without eventual ossification (4). Disruption of this process in utero or during childhood can result in the loss of vertical growth. This disruption also has implications in pediatric nasal surgery, as violation of the posterior septum at this junction and the bony septum can have deleterious impact on the growth center of the septum.
HISTORY AND PHYSICAL
Making an accurate diagnosis is central to the management of the crooked nose, as there are many potential configurations of crooked noses. The surgeon must begin with a detailed history and physical examination, paying careful attention to all aspects of the nose. The history should include information regarding the patient’s medical conditions, previous nasal surgery, nasal trauma, nasal airway, allergies, and drug and tobacco use. The mechanism of injury may be helpful to know, as it will help to separate the traumatic deviations from the congenital ones. If a patient had previous surgery, it is sometimes helpful to obtain previous operative report and radiographic studies.
To begin the examination, the surgeon should first establish the midline of the face as defined by a vertical line through the menton, the upper incisors, the philtrum, and the glabella. Figure 183.1 shows how a vertical line drawn through from the glabella, through the philtrum, and through the menton can give the doctor a sense of whether the nose is crooked. It can also help identify asymmetries
of the face that were previously unrecognized. The nose is then divided into thirds, that is, the upper, middle, and lower thirds (see Fig. 183.2). For the most part, we can generally say that the upper third is composed of the nasal bones, the middle third is composed of the septum and upper lateral cartilages, and the lower third is the septal angle and lower lateral cartilages. Each third is individually examined in relation to the midline or relative midline. The thirds are classified into right, left, or center of midline. Given the number of possibilities, there are theoretically 26 permutations of crooked noses. The 27th possibility is a center-center-center nose, which is a straight nose. Half of these permutations are mirror images of each other. Figure 183.3 demonstrates five of these permutations (5).
of the face that were previously unrecognized. The nose is then divided into thirds, that is, the upper, middle, and lower thirds (see Fig. 183.2). For the most part, we can generally say that the upper third is composed of the nasal bones, the middle third is composed of the septum and upper lateral cartilages, and the lower third is the septal angle and lower lateral cartilages. Each third is individually examined in relation to the midline or relative midline. The thirds are classified into right, left, or center of midline. Given the number of possibilities, there are theoretically 26 permutations of crooked noses. The 27th possibility is a center-center-center nose, which is a straight nose. Half of these permutations are mirror images of each other. Figure 183.3 demonstrates five of these permutations (5).
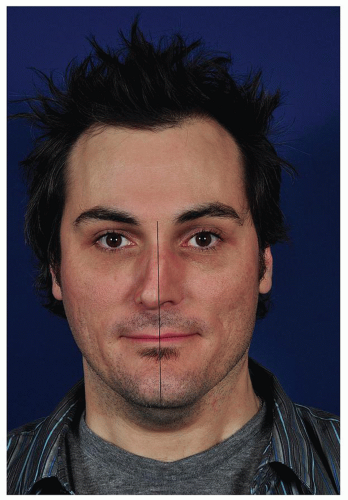 Figure 183.1 A vertical line is drawn from the glabella, through the philtrum, and then through the menton. This line can help identify asymmetries and deviations. One can see that the deviation of the nose lies in the middle and lower third of the nose. In this patient, the vertical lines allow the viewer to see asymmetry of the mandible and midface. His left side is stronger and has more volume than his right side. |
The surgeon should palpate the nose carefully to feel the thickness of the skin and the position of the bones and cartilage and determine tip strength. Convexities, concavities, and buckles in the cartilage can also be determined using palpation. Tip support is determined by manually compressing the tip. Additionally, the surgeon should feel the caudal septum and the septal angle to assess its strength and integrity, as well as the position of the septum in relation to the midline.
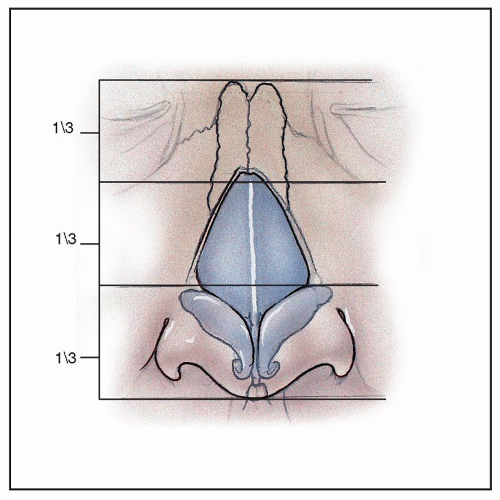 Figure 183.2 The nose can be divided into thirds. This is central to diagnosis and treatment of a crooked nose. The components of the thirds can be seen in this illustration. |
A thorough endonasal exam should be completed in a systematic manner to determine the position, health, and function of the nasal septum, turbinates, the internal and external nasal valves, and nasal mucosa. The patient should be observed while taking normal and accentuated breaths through the nasal airway. The examiner will often see external evidence of nasal valve collapse, and
the area of collapse should be noted. The nasal mucosa should be initially examined without decongestion. This helps assess whether there is an allergic or reactive component. Finally, the nasal mucosa must be decongested with either oxymetazoline or 0.25% Neo-Synephrine. The decongestion may reveal posterior and high dorsal septal deflections that may have been previously hidden by inflamed mucosa. If there is history of previous surgery or trauma, the septum should be palpated with a cotton tip applicator or cerumen loop to determine if the septal cartilage is missing or deficient. In a severely deviated nose, the full extent of the septum may not be able to be visualized without a fiberoptic device. The size of the turbinates must also be analyzed, as many patients can benefit from concomitant turbinoplasty. If the patient has a history that suggests chronic sinusitis, a CT scan may be of benefit.
the area of collapse should be noted. The nasal mucosa should be initially examined without decongestion. This helps assess whether there is an allergic or reactive component. Finally, the nasal mucosa must be decongested with either oxymetazoline or 0.25% Neo-Synephrine. The decongestion may reveal posterior and high dorsal septal deflections that may have been previously hidden by inflamed mucosa. If there is history of previous surgery or trauma, the septum should be palpated with a cotton tip applicator or cerumen loop to determine if the septal cartilage is missing or deficient. In a severely deviated nose, the full extent of the septum may not be able to be visualized without a fiberoptic device. The size of the turbinates must also be analyzed, as many patients can benefit from concomitant turbinoplasty. If the patient has a history that suggests chronic sinusitis, a CT scan may be of benefit.
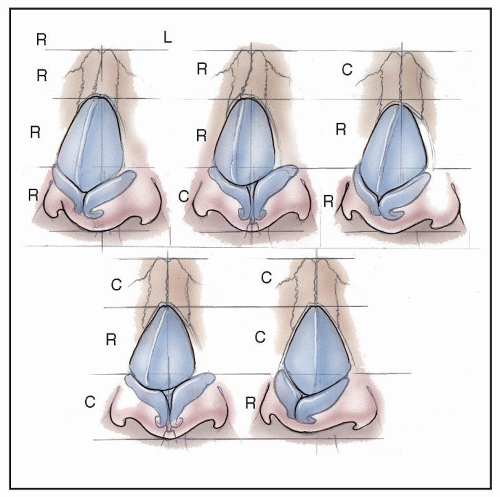 Figure 183.3 Artist-rendered images of five different permutations of crooked noses. There are 26 possible configurations. |
A careful examination of the integrity of the internal and external nasal valve should be performed. When a patient inspires deeply, a weak internal valve can be seen externally by a depression just above the nasal ala or along the piriform aperture. The external valve is composed of the lateral crura, the suspensory ligaments of the lateral crura, and the fibromuscular tissue of the ala. Manually retracting the cheek laterally (the Cottle maneuver) can help assess if there is an element of valve insufficiency. This can also be done using a curette to stent open the internal and external nasal valves to independently determine where the weakness lies.
Radiographic assessment is necessary if a patient has signs and symptoms consistent with paranasal sinus disease or has polyposis. They may be also helpful in patients who previously sustained major trauma that required open reduction and internal fixation of the craniofacial skeleton. This surgical hardware will need to be identified prior to surgery, as it may need to be removed before osteotomies can be performed.
Standard rhinoplasty photographs must be taken for medical documentation and to assist with the evaluation and analysis of the patient. These views include the frontal, profile, three-quarter, and base views. The authors also like to take two additional photographs when patients have crooked noses. One is the bird’s-eye view, which gives the surgeon more information on the shape of the dorsal line (see Fig. 183.4). The use of overhead flash is preferable as it most closely duplicates overhead sunlight, which accentuates deviations. The other is the three-quarter base view where the entire dorsum and nasal walls are visible in relationship to the nasal base (see Fig. 183.5). Photos must be available and easily visible in the operating room during surgery. Due to local anesthetic injections and surgical edema, asymmetries can become masked or imperceptible. Therefore, the surgeon must periodically refer to these photos during the operation. Postoperative photos are usually taken at 6-month and 1-year intervals to track healing progression.
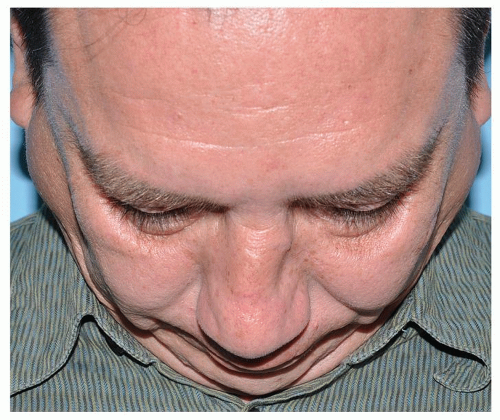 Figure 183.4 This is an example of a bird’s-eye view. This allows one to see another perspective of the dorsal line. |
TREATMENT STRATEGY
Surgical correction of the deviated nose can be conceptually and strategically divided into the upper third, middle third, and lower third. The upper third is composed of the nasal bones and the frontal process of the maxilla. The middle third is composed of the bony cartilaginous junction (called the keystone), the upper lateral cartilages, and the dorsal septum. The lower third is composed of the caudal septum and the lower lateral cartilages.
Septum
Septoplasty surgery in the crooked nose can be approached through a hemitransfixion incision. This incision allows easy access to both sides of the septum and facilitates easy repositioning of the caudal septum to the facial midline. To best mobilize the septum, separation of the posterior and
inferior osseocartilaginous junction plus elevation of the mucoperiosteum of the maxillary crest is often required. Releasing the attachment of the upper lateral cartilages can also help mobilize a septum that is deviated.
inferior osseocartilaginous junction plus elevation of the mucoperiosteum of the maxillary crest is often required. Releasing the attachment of the upper lateral cartilages can also help mobilize a septum that is deviated.
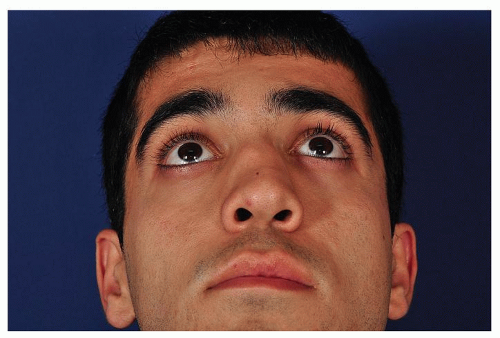 Figure 183.5 This is an example of the three-quarter base view. This view gives a view of the dorsal deviation with relation to the tip. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


