Any student of neck dissection must understand the vascular supply of the skin of the neck and the anatomic characteristics and relationships of certain structures that are encountered within the course of performing a neck dissection.
Vascular Supply to the Skin of the Neck
To avoid complications such as wound breakdown, skin flap necrosis, and exposure of the carotid artery after neck dissection, the incisions must be placed correctly.
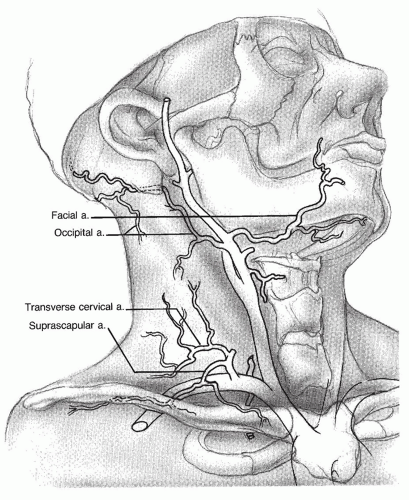
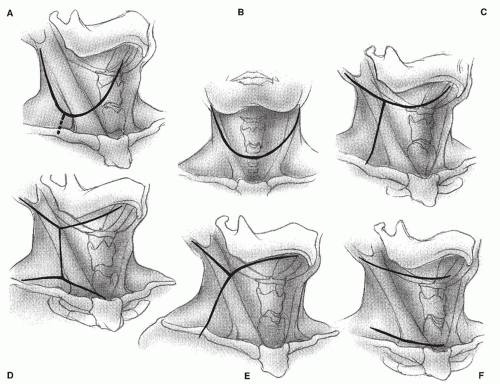
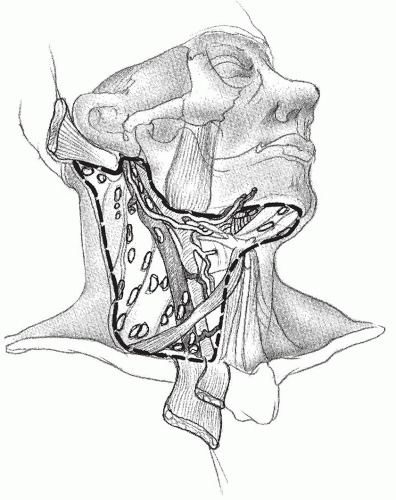
The skin of the anterior lateral aspect of the neck is supplied by descending branches of the facial, submental, and occipital arteries and by ascending branches of the transverse cervical and suprascapular artery (Fig. 117.1). These arterial branches anastomose, forming a superficial network of vessels that runs predominantly in a vertical direction. Although some or all the main arteries or their perforating branches may be ligated or divided during a neck dissection, the superficial, predominantly vertical, vascular plexus must remain intact to ensure adequate blood supply to the skin flaps. Thus, the incisions in the neck that are more likely to safeguard the blood supply to the skin flaps are the single transverse incision in the mid portion of the neck, the superiorly based apron-like incision from mastoid to mentum for combined neck dissection with intraoral procedures (Fig. 117.2A), and the apron-like incision used when a neck dissection is performed in conjunction with a laryngectomy (Fig. 117.2B).
The Y incision and the double-Y incision jeopardize the blood supply to the inferior and middle skin flaps, respectively, and suffer from placing a trifurcate incision over the carotid artery (Fig. 117.2C and D). The modification of the Schobinger incision creates a long anterior medial flap, the tip of which may necrose as a result of the limited ascending blood supply (Fig. 117.2E). The MacFee double transverse incision transects the ascending and descending blood supply to the central portion of the flap (Fig. 117.2F). This flap, however, usually fares well even in the previously irradiated patient.
Platysma Muscle
Located in the anterolateral aspect of the neck, the platysma is a wide, quadrangular, sheet-like muscle that extends obliquely from the upper chest to the lower face. This muscle, a remnant of the panniculus carnosus, is located immediately deep to the subcutaneous tissue and thus provides an easily identifiable plane to raise skin flaps during neck surgery. In most neck dissections, flaps are elevated by dissecting in a plane immediately deep to the platysma; however, when the extent of the disease is such that the platysma must be left attached to the specimen, flaps can be elevated easily in a plane immediately superficial to this muscle. The beginning head and neck surgeon must remember that, because of its oblique direction, the platysma does not cover an inferiorly based triangle in the anterior aspect of the neck and most of the posterolateral aspect of the neck. Here, flaps must be elevated in a subcutaneous plane created by the surgeon. While making the incisions for a neck dissection and elevating the skin flaps, it is helpful to remember that the posterior border of the platysma is either over or slightly anterior to the external jugular vein and the greater auricular nerve.
Marginal Mandibular Branch of the Facial Nerve
Identifying the marginal mandibular branch is essential to perform an adequate excision of the lymph nodes in the submandibular triangle. The practice of ligating the anterior facial vein low in the submandibular triangle and retracting it superiorly to “protect the marginal branch” can also result in elevation of the prevascular and retrovascular lymph nodes, thus precluding their appropriate removal. When indicated, it is preferable to identify the nerve and thoroughly remove these lymph nodes.
Figure 117.1 Vascular supply of the neck skin. (Adapted from Freelend AP, Rogers JH. The vascular supply of the cervical skin with reference to incision planning. Laryngoscope 1975;85:714, with permission.)
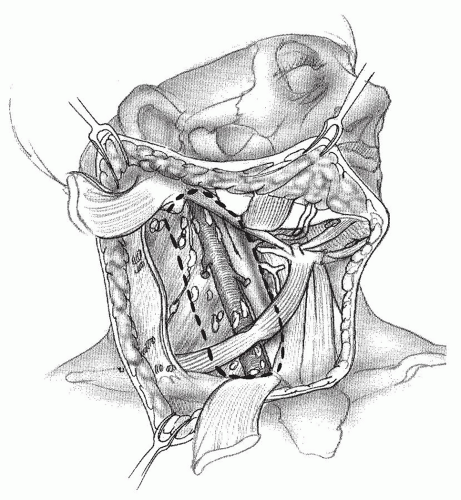
The nerve can be identified about 1 cm in front of and below the angle of the mandible by incising the superficial layer of the deep cervical fascia that envelops the submandibular gland, immediately above the gland, in a direction parallel to the direction of the nerve. The incised fascia then is gently pushed superiorly, exposing the nerve that lies deep to it but superficial to the adventitia of the anterior facial vein. The submandibular retrovascular lymph nodes are usually near the nerve and must be carefully dissected away from it. As this is done, the facial vessels are exposed and can be divided.
Spinal Accessory Nerve
Below the jugular foramen, the external branch of the spinal accessory nerve is located medial to the digastric and stylohyoid muscles and lateral or immediately posterior to the internal jugular vein (IJV). Occasionally, the uppermost portion of the nerve is posteriomedial to the vein. From here, the nerve runs obliquely downward and backward to reach the medial surface of the sternocleidomastoid muscle (SCM) near the junction of its superior and middle thirds (two to three finger breadths below the tip of the mastoid). Although the nerve can continue its downward course entirely medial to the muscle (18%), more commonly, it traverses and appears in the posterior border of it (82%) (1). Here, the nerve is always located above the point where the greater auricular nerve turns around the posterior border of the SCM, also known as Erb point (2). The mean distance between Erb point and the spinal accessory nerve is 10.7 mm, SD ± 6.3. It then runs through the posterior triangle of the neck and crosses the anterior border of the trapezius muscle. The mean distance between this point and the clavicle is 51.3 mm, SD ± 17 (2). Two anatomic characteristics of this portion of the nerve are relevant to avoid injuring it in the course of a neck dissection. First, the spinal accessory nerve is located rather superficially as it courses through the middle and low posterior triangle of the neck, and it can be easily injured while elevating the posterior skin flaps. Second, the nerve does not enter the trapezius muscle at the anterior border of it but courses along the deep surface of the muscle in close relationship with the transverse cervical vessels. Therefore, isolating the nerve to the level of the anterior border of the trapezius does not ensure its preservation during surgical dissection below this point, particularly in a bloody operative field.
The levator scapulae is a triangular muscle located deep in the lateral aspect of the neck, anterior and medial to the splenius capitis muscle. It extends from the transverse process of the atlas and the next three cervical vertebrae to the superior angle and the spine of the scapula. The action of levator scapulae is to raise the medial angle of the scapula and incline the neck to the corresponding side with rotation of the neck in the same direction. With the trapezius muscle, the levator scapulae makes a shrug possible.
The nerves to the levator scapulae, which vary in number from 1 to 3, branch off the fourth and fifth cervical nerves and travel posteriorly and inferiorly. They cross the anterior border of the levator scapulae and remain on the surface of the muscle for a short distance. The nerves to levator scapulae are under the fascia of this muscle; thus, in the course of any neck dissection, but especially in a radical neck dissection (RND) or a modified radical neck dissection (MRND), it is crucial to keep the plane of dissection superficial to the fascia of the levator in order to preserve these nerves. The dorsal scapular nerve is inconsistent in its anatomic relations in the posterior triangle of the neck and contributes to the innervation of the levator scapulae in a minority of cases (3). Because one of the functions of the levator is to draw the scapula and the shoulder upward and medially, inadvertent or unnecessary resection of the nerves to it during an RND may add to the resulting deformity and functional disability of the shoulder.
Thoracic Duct
At the base of the neck, the thoracic duct is located medial to and behind the left common carotid artery and the vagus nerve. From here, it arches upward, forward, and laterally, passing behind the IJV and in front of the anterior scalene muscle and the phrenic nerve. It then opens into the IJV, the subclavian vein, or the angle formed by the junction of these two vessels. The duct is anterior and medial to the thyrocervical trunk and the transverse cervical artery. Precise knowledge of these anatomic relationships is important to avoid injuring the duct during a neck dissection. It is even more important when the surgeon is called on to search for and repair a chyle leak during or after a neck dissection. To prevent a chyle leak, the surgeon also must remember that the thoracic duct may be multiple in its upper end and that at the base of the neck it usually receives a jugular, a subclavian, and usually other minor lymphatic trunks, which must be ligated or clipped individually.
Fascial Compartments of the Neck
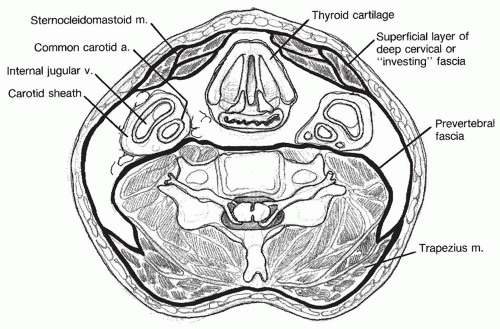
The deep cervical fascia of the neck is divided into three layers: superficial, middle, and deep (Fig. 117.3). The superficial or investing layer surrounds the entire neck. It arises from the vertebral spinous processes and the ligamentum nuchae and encircles the entire neck to attach itself again to the spinous processes on the opposite side. This fascia divides to enclose the trapezius muscle. At the anterior border of this muscle, the two layers fuse into a single layer that crosses the posterior triangle of the neck. It divides again to surround the inferior belly of the omohyoid muscle and the sternomastoid muscle. At the lateral border of the strap muscles, it sends fibers between them before fusing in front of them as it extends onto the other side of the neck. This fascia also envelops the submandibular and parotid glands.
Figure 117.3 Layers of the cervical fascia.
The middle layer of the deep cervical fascia, also called the visceral fascia, surrounds the visceral structures of the anterior portion of the neck. The deep layer of the deep cervical fascia or prevertebral fascia surrounds the deep muscles of the neck. Among them, it covers the splenius capitis, the levator scapulae, and the scalene muscles. It extends onto the other side of the neck, covering the prevertebral muscles.
The carotid sheath encircling the jugular vein, common carotid artery, and vagus nerve is formed by all layers of the deep cervical fascia. The carotid sheath originates superiorly at the jugular foramen, where it attaches to the skull base. It then follows the course of the vessels, traversing the anterior cervical triangle and extending inferiorly into the thoracic inlet.
Lymphatics of the Neck
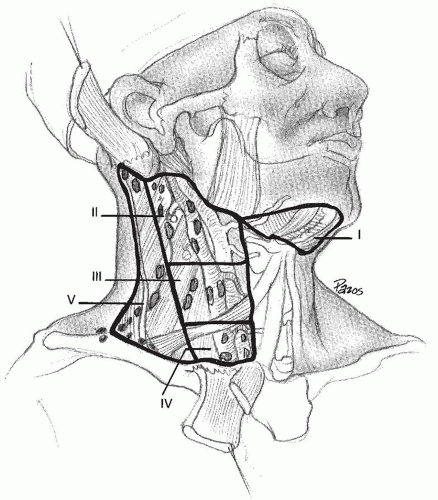
The lymph node regions of the neck are shown in Figure 117.4. The six levels currently used encompass the complete topographic anatomy of the neck. The concept of sublevels has been introduced into the classification since certain zones have been identified within the six levels, which may have clinical significance.
Level I is divided in two sublevels: sublevel IA (submental), which includes the lymph nodes within the triangle bound by the anterior bellies of the digastric muscles and the mylohoid muscle, and sublevel IIB (submandibular), which includes the lymph nodes with the boundaries of the triangle formed by the anterior and posterior bellies of the digastrics and body of the mandible.
Level II (upper jugular) includes the lymph nodes located around the upper third of the IJV and adjacent spinal accessory nerve extending from the level of the skull base to the level of the inferior border of the hyoid. The anterior/medial boundary is the stylohyoid muscle (the radiologic correlate is the vertical plane defined by the posterior surface of the submandibular gland), and the posterior (lateral) boundary is the posterior border of the SCM. Two sublevels are recognized in level II: sublevel IIA contains nodes in the region anterior to the spinal accessory nerve (SAN) and sublevel IIB contains nodes posterior to the SAN.
Figure 117.4 Lymph node regions of the neck.
Level III (midjugular) includes the lymph nodes located around the middle third of the IJV extending from the inferior border of the hyoid bone to the inferior border of the cricoid cartilage. The anterior/medial boundary is the lateral border of the sternohyoid muscle, and the posterior/lateral boundary is the posterior border of the SCM.
Level IV (lower jugular) encompasses the lymph nodes located around the lower third of the IJV extending from the inferior border of the cricoid cartilage to the clavicle.
The anatomic boundary that separates the medial border of levels III and IV from the lateral border of level VI has traditionally been the lateral border of the sternohyoid muscle, a landmark that cannot be easily discerned on imaging studies. Therefore, the medial aspect of the common carotid artery has been suggested as an alternate boundary to separate these levels in an axial plane in imaging studies (4).
Level V (posterior triangle) comprises predominantly of the lymph nodes located along the lower half of the spinal accessory nerve and the transverse cervical artery. The supraclavicular nodes are also included in posterior triangle group. The superior boundary is the apex formed by convergence of the sternocleidomastoid and trapezius muscles, the inferior boundary is the clavicle, the anterior boundary is the posterior border of the SCM, and the posterior boundary is the anterior border of the trapezius muscle. A horizontal plane marking the inferior border of the anterior cricoid arch separates two sublevels. Sublevel VA, above this plane, includes the spinal accessory nodes. Sublevel VB, below this plane, includes the nodes that follow the transverse cervical vessels and the supraclavicular nodes with the exception of Virchow node, which is located in level IV.
Level VI (anterior compartment): Lymph nodes in this compartment include the pre- and paratracheal nodes, precricoid (delphian) node, and the perithyroidal nodes including the lymph nodes along the recurrent laryngeal nerves. The superior boundary is the hyoid bone, the inferior boundary is the suprasternal notch, and the lateral boundaries are the common carotid arteries.
Other lymph node groups: Lymph nodes involving regions not located within these levels should be referred to by the name of their specific nodal group; examples of these are the superior mediastinum, the retropharyngeal, the periparotid, the buccinator, the postauricular, and the suboccipital lymph nodes.
TABLE 117.1 PERCENTAGE OF METASTATIC LYMPH NODES INVOLVED IN ELECTIVE AND THERAPEUTIC RNDs
Primary Site
Level of Metastatic Lymph Nodes
Oral Cavity
Oropharynx
Hypopharynx
Larynx
Elective
Therapeutic
Elective
Therapeutic
Elective
Therapeutic
Elective
Therapeutic
I
58
61
7
17
0
10
14
8
II
51
57
80
85
75
78
52
68
III
26
44
60
50
75
75
55
70
IV
9
20
27
33
0
47
24
35
V
2
4
7
11
0
11
7
5
Modified from Shah JP. Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg 1990;160(4):405-409.
Patterns of Lymph Node Metastases
Lindberg first described the clinical pattern of cervical metastases for various primary sites in 1972 (5). Shah (6), in 1990, examined the distribution of nodal metastases in 1,119 RNDs performed both electively and therapeutically for squamous cell carcinoma (SCCA) of the oral cavity, oropharynx, hypopharynx, and larynx. He found a consistent distribution of cervical metastases (Table 117.1). The majority of metastases from cancer of the oral cavity were found in lymph nodes in levels I, II, and III. On the other hand, most metastases from carcinomas of the oropharynx, hypopharynx, and larynx were found in levels II, III, and IV. The lymph nodes in level V were not involved in the absence of metastases at other levels.
The significance of other lymphatic groups, such as the retropharyngeal lymph nodes (RPLNs) and paratracheal nodes, has also been characterized (7). Metastases to the RPLNs can occur with SCCA of the hypopharynx, tonsil, soft palate, posterior and lateral oropharynx, nasopharynx, and supraglottis.
Metastases from cancers of the larynx can occur to the paratracheal lymph nodes (PTLNs). In a study of 91 selected patients with carcinoma of the larynx who underwent PTLN dissection, Weber et al. (8) found that metastases to these lymph nodes occurred primarily in patients with subglottic and transglottic tumors, but they also occurred in patients with glottic tumors. In a prospective study of 45 patients with advanced glottic cancers, who underwent bilateral paratracheal node dissection as part of their treatment, Shenoy et al. (9) found metastases in the ipsilateral paratracheal nodes in 4% of the cases and contralateral metastases in 2%. Failure to address the paratracheal nodes for laryngeal cancer is a known cause of stomal recurrence.
PHYSIOLOGY
The trapezius is a fan-shaped muscle composed of upper, middle, and lower segments, each of which functions in a different but complementary manner. The trapezius and the other muscles that insert on the scapula stabilize and control the shoulder girdle during arm movement. The levator scapulae acts synergistically with the upper division of the trapezius to elevate the scapula; the rhomboid assists the middle part of the trapezius in retracting and stabilizing the scapula against the posterior thoracic cage. The simultaneous action of the upper and lower divisions of the trapezius muscle results in a unique rotatory action of the scapula. The upward rotation of the scapula, in combination with abduction of the arm at the glenohumeral joint, permits elevation of the arm beyond 90 degrees at the shoulder level. As is discussed in detail later in this chapter, paralysis of the trapezius muscle causes a syndrome characterized by weakness and deformity of the shoulder girdle, usually accompanied by pain.
DIAGNOSTIC EVALUATION
Clinical Examination
Clinical examination of the neck by palpation is not uniformly reliable in the detection of cervical lymph node metastases, particularly of lymph nodes minimally involved by the tumor. The reported error rate in assessing the presence or absence of cervical lymph node metastases by palpation ranges from 20% to 50%. The factors responsible for this variation are not only the ability and experience of the examiner but also the patient’s habitus and previous treatment to the neck with surgery or radiation therapy. With the advent of modern imaging techniques, it was hoped that the clinician would not have to rely solely on clinical examination to make decisions in the treatment of the neck.
Imaging Studies
Using the histologic demonstration of metastasis in a lymph node as the gold standard, several studies have shown that ultrasonography (US), computed tomography (CT), and magnetic resonance imaging (MRI) have a higher sensitivity and specificity than clinical examination in the detection of metastases in lymph nodes. In a prospective study of 48 patients who were to undergo neck dissection, Haberal et al. (10) found that the sensitivity and specificity of palpation for the detection of metastases in the lymph nodes were 64% and 85%, respectively, while the corresponding values were 72% and 96% for US and 81% and 96% for CT. Adams et al. (11) reported similar results for US and CT; in addition, they reported a sensitivity of 80% and a specificity of 79% for MRI. What these observations indicate is that a “negative” US, CT, or MRI of the neck cannot be relied to withhold elective treatment of the cervical lymph nodes, since they cannot detect metastases in 19% to 28% of the patients staged clinically N0. Obviously the imaging criteria used to diagnose metastasis in a lymph node are not absolutely reliable. The imaging criterion used most often to consider a cervical node suspicious for metastasis is size larger than 1.5 cm in maximum diameter for nodes located in levels I and II and larger than 1 cm for nodes in other regions of the neck (12). Although a correlation exists between the size of a lymph node and the presence of histologic metastasis (Table 117.2), it is clear that not all enlarged lymph nodes contain metastatic deposits and that nodes smaller than 1 or 1.5 cm can indeed contain metastases. Thirty-three percent of all metastases from SCCAs of the head and neck are found in lymph nodes smaller than 1 cm, 10% of tumor-positive neck dissection specimens contain only metastases less than 3 mm in diameter, and, more importantly, 25% of all clinically occult lymph node metastases are too small to be detected by any of the currently available imaging techniques (13). DiNardo (14) demonstrated that 88% of metastases from the carcinomas of the floor of the mouth were found in nodes that were 1 cm or less in diameter.
The presence of a central area of lucency within a node shown on CT was at one time considered equivalent to the presence of necrotic tumor within a node; however, such a finding can be caused by an artery with plaque formation or a fatty inclusion in a lymph node. Another imaging criterion used to “diagnose” metastasis in a lymph node is the shape of the node, as determined by the ratio of its long (l) and short (s) axis diameters. In a study by Steinkamp et al. (15), 730 enlarged cervical lymph nodes in 285 patients were examined using ultrasound, and the l/s ratio was calculated. Histologic examination after neck dissection revealed that 95% of the enlarged cervical nodes, shown on ultrasound to have a l/s ratio of more than 2, were correctly diagnosed as benign. Nodes presenting with a more circular shape and a l/s ratio of less than 2 were diagnosed correctly as metastases with 95% accuracy.
TABLE 117.2 NODAL SIZE AND PRESENCE OF HISTOLOGIC METASTASES
Histologic Status (%)
Node Size (cm)
Negative
Positive
Positive with Extranodal Extension
1
67
33
14
2
38
62
26
3
19
81
49
4
12
88
71
5
0
100
76
From Hamakawa H, Fukizumi M, Bao Y, et al. Genetic diagnosis of micrometastasis based on SCCA antigen mRNA in cervical lymph nodes of head and neck cancer. Clin Exp Metastasis 1999;17(7):593-599, with permission.
Ultrasound Guided Fine-Needle Aspiration Biopsy
In an attempt to overcome the lack of sensitivity of morphologic imaging criteria, US was combined with fine needle aspiration biopsy (US-FNAB). This technique appeared more promising for the preoperative evaluation of the N0 neck as it enables sampling of lymph nodes as small as 3 mm in diameter and adds the advantages of cytologic evaluation (16). However, the usefulness of this technique is strongly dependent on the skill and time of the ultrasonographer and on the experience of the cytopathologist. Furthermore, the outcomes of a wait-and-see policy after negative US-FNAB have been disappointing. In a study of 92 patients with tumors of the oral cavity, staged T1 and T2, who were observed after a negative US-fine-needle aspiration (US-FNA), metastases in neck nodes became apparent subsequently in 19 (21%) (17). In a more recent study, Wensing et al. (18) found that palpation and US with or without US-FNAB missed occult lymph node metastases in 22% of the patients with oral cavity SCCA. These figures are troubling because the incidence of lymph node metastases in patients with such tumors, who are observed without any intervention to the neck, is about 25%.
Positron Emission Tomography
Prospective studies using 18-fluorodeoxyglucose (FDG) positron emission tomography (PET) to assess lymph node metastases from SCCAs of the oral cavity have shown a sensitivity and specificity higher than MRI, CT, and US. However, current FDG-PET techniques are also limited in the detection of tumor foci smaller than 1 cm (19,20). Kyzas et al. (21) performed a meta-analysis of 32 studies that assessed the diagnostic performance of PET scans in patients with SCCA of the head and neck. In patients staged clinically N0, the sensitivity of 18 PET scan was only 50% (95% CI: 37% to 63%), whereas specificity was 87% (95% CI: 76% to 93%). These authors also compared the performance of PET scan with that of “conventional diagnostic methods,” that is, CT, MRI, and ultrasound with fine-needle aspiration (FNA) by analyzing studies that had also used these diagnostic methods on the same patients. The sensitivity and specificity of PET scans were 80% and 86%, respectively, and of “conventional diagnostic tests” were 75% and 79%. Thus, at the present time, the role for PET scan in the evaluation of the N0 neck is limited as it will not detect metastases in 20% to 50% of the cases.
In another effort to overcome the limitations of current imaging techniques, particularly their inability to differentiate a tumor-infiltrated lymph node from a normal or a reactive one, de Bree et al. (22) have experimented with radioimmunoscintigraphy (RIS). With this technique, SCCA specific monoclonal antibodies labeled with 99mTc were given intravenously to patients with SCCA who underwent neck dissection. Unfortunately, RIS was not superior to CT and MRI for the detection of lymph node metastases.
CT and MRI are valuable in the evaluation of lymph nodes that are not easily accessible to the hands of the examiner, such as the retropharyngeal, upper mediastinal, and, in some patients, the PTLNs. They are also valuable in the assessment of resectability of large metastatic deposits in the neck, because in most instances they can define the relationship of a metastatic tumor with critical structures, such as the common and the internal carotid artery, the cervical spine, the vertebral artery, and the brachial plexus. If tumor involvement of the common or the internal carotid artery is suspected, a systematic preoperative evaluation should include four-vessel cerebral angiography to determine the status of the contralateral carotid and to assess collateral intracerebral circulation. In addition, an attempt should be made during the angiography to measure carotid back pressure and to assess dynamically the collateral circulation by using balloon occlusion techniques while monitoring the patient for evidence of neurologic deficits under normotensive and hypotensive conditions.
Fine-Needle Aspiration
FNA has become a valuable diagnostic tool in patients with a mass in the neck in whom metastatic carcinoma is suspected. According to numerous recent reports, the specificity of FNA ranges from 94% to 100% and the sensitivity ranges from 92% to 98%. The interobserver variability between cytopathologists in one series has been reported as 8%. FNA has been found to be most accurate in the diagnosis of epithelial malignancies, achieving nearly 100% accuracy.
FNA is indicated in the patient with a solid mass in the neck after a thorough examination of the mucosal surfaces and skin of the head and neck region fails to reveal a primary tumor. If the mass is located in the supraclavicular area, FNA is essential in the initial evaluation of the patient. The cytopathology findings then can guide the clinician’s search for a primary tumor below the clavicles.
Sentinel Node Biopsy
Sentinel lymph node biopsy (SLNB) is feasible and useful as a staging procedure in patients with early carcinomas of the oral cavity and in particular for patients with cancers of the oral tongue. Proponents of this technique point out that it allows accurate histopathologic staging of the neck by examining the sentinel lymph node (SLN) with serial sectioning and immunohistochemistry, and it avoids unnecessary neck dissection and its possible complications.
The SLNB is based on the belief that cancers metastasize via lymphatics to regional lymph nodes in an orderly fashion, that this process is embolic in nature, and that the lymph node that first receives lymphatic drainage from the primary site can be identified and excised for histologic analysis (23).
Early studies in patients with SCCAs of the mucosal surfaces of the head and neck investigated the methodology and feasibility of SLNB (23,24,25,26). In general, the primary cancer should be accessible to infiltration with a radioisotope-labeled colloid to perform a lymphoscintigraphy and a blue dye to aid in intraoperative localization of the sentinel node. These localizing methods have been shown to be complementary. Ross et al. (26) in a multicenter study investigated SLNB in 134 patients with SCCA of the oral cavity and oropharynx, staged T1/T2 N0. Lymphoscintigraphy was performed preoperatively; blue dye and a gamma probe were used intraoperatively to aid in the identification of sentinel nodes. Sentinel nodes were identified in 93% of the cases. The number of sentinel nodes varies, but in a series of 48 patients studied by Ross et al. (24), the mean number of sentinel nodes harvested was 2.4.
Subsequent studies have examined the utility of SLNB in patients with oral cavity or oropharyngeal cancers staged T1/T2 N0. The sensitivity of the procedure is 90% when the histopathology of the sentinel node is compared with that of the neck dissection specimen (27). It results in histopathologic upstaging of the clinically N0 neck in 36% of the patients when the nodes are examined with routine hematoxylin-eosin staining; serial sectioning and immunohistochemistry upstage an additional 8% of the cases (24). The detection of micrometastases can be further enhanced by using highly specific tumor markers and molecular methods (28,29).
Recently, Civantos et al. (30) reported the results of a North American Multi-Institutional Prospective Study that evaluated the utility of SLNB in T1/T2 oral SCCAs. The study included 140 patients (68% oral tongue, 19% the floor of the mouth) from 25 institutions who underwent SLNB and selective neck dissection (SND) (levels I-IV). The negative predictive value (NPV) was 94% when the SLNs were examined with hematoxylin-eosin stains and 96% when they were examined with serial sectioning and immunocytochemistry (30). The NPV among experienced surgeons was 100% versus 95% for less experienced ones. The SLN was the only positive node in 51% of the cases with a positive SLN. The false-negative rate was 9.8% overall. Interestingly, however, the false-negative rate was 10% in patients with cancers of the oral tongue but was 25% in patients with cancers of the floor of the mouth. In the experience of the University of Miami (31), the NPV of SLNB was 88.5% in patients with cancers of the floor of mouth (FOM) and 95.8% when these patients were excluded. Similarly, Ross et al. (26) have reported that the identification of SLNB in patients with FOM cancers was lower (86%) than in patients with tumors in other locations (97%); the sensitivity of SLNB in FOM cancers was also lower (80%), compared with other tumor locations (100%). It appears that lymphoscintigraphy in cancers of the FOM is not as helpful in identifying the SLN due to the shine-through effect of the radioactivity at the primary site; it obscures the lymph nodes in level I, which are one of the primary echelons of lymphatic drainage for the FOM and lower gum. Obviously, this limits the utility of SLNB in patients with tumors in these locations.
STAGING
At completion of the clinical evaluation of a patient with SCCA of the head and neck region, the disease should be classified according to stage. The staging for the lymph nodes proposed by the American Joint Committee on Cancer in 2009 (32) is outlined below:
NX: Regional lymph nodes cannot be assessed.
N0: No regional lymph node metastasis.
N1: Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension.
N2: Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension; or in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension; or in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension.
N2a: Metastasis in a single ipsilateral lymph node more than 3 cm but not more than 6 cm in greatest dimension.
N2b: Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension.
N2c: Metastasis in bilateral or contralateral nodes no more than 6 cm in greatest dimension.
N3: Metastasis in a lymph node more than 6 cm in greatest dimension.
Staging of the neck in nasopharyngeal carcinoma patients is different because the distribution and the prognostic impact of regional lymph node spread from nasopharynx cancer, particularly of the undifferentiated type, are different from those of other head and neck mucosal cancers and justify the use of the following scheme:
NX: Regional lymph nodes cannot be assessed.
N0: No regional lymph node metastasis.
N1: Unilateral metastasis in lymph node(s), 6 cm or less in greatest dimension, above the supraclavicular fossa.
N2: Bilateral metastasis in lymph node(s), 6 cm or less in greatest dimension, above the supraclavicular fossa.
N3: Metastasis in a lymph node(s) greater than 6 cm and/or to supraclavicular fossa.
N3a: Greater than 6 cm in dimension.
N3b: Extension to the supraclavicular fossa.
CLASSIFICATION OF NECK DISSECTIONS
Several cervical lymph node dissections are currently used for the surgical treatment of the neck in patients with cancer of the head and neck region. To standardize the nomenclature used to refer to these operations, it is essential to adopt a common nomenclature for the lymph node groups of the neck, such as the one outlined earlier in this chapter. The current classification of neck dissections recommended by the American Academy of Otolaryngology-Head and Neck Surgery (Table 117.3) takes into account the lymph node groups of the neck that are removed and secondarily the anatomic structures that may be preserved, such as the spinal accessory nerve and the IJV. Analyzing neck dissections from these two points of view, there are essentially four anatomic types of neck dissections: radical, modified radical, selective, and extended. Recently, clinicians from around the world have proposed a nomenclature for neck dissection that, if recognized internationally, would be “logical, unambiguous, precise, and easy to remember” (33).
In this classification, the following three descriptors are used to label a neck dissection:
“ND” to represent neck dissection that is prefaced by either “L” or “R” for side. If bilateral, both sides must be classified independently.
The levels and sublevels of lymph nodes removed designated by Roman numerals I through VII in ascending order. For levels that contain sublevels (I, II, and V), listing of the level without a sublevel indicates that the entire level (both A and B) was excised.
The nonlymphatic structures removed designated by their internationally recognized initials, that is, SCM for sternocleidomastoid muscle, IJV for internal jugular vein.
It is hoped that this new classification system will convey precisely the extent of lymphatic and nonlymphatic structures removed in a neck dissection that will then allow better comparison of results between studies.
TABLE 117.3 CLASSIFICATION OF NECK DISSECTIONS
2001 Classification
2010 Proposed Classification
1.
Radical neck dissection
1.
ND (I-V, SCM, IJV, CNXI)
2.
Modified radical neck dissection
2.
ND (I-V, SCM, IJV), ND (I-V, IJV, CNXI), ND (I-V)
3.
Selective neck dissection (SND):
3.
SND (I-III/IV)
ND (I, II, II/IV)
SND (II-IV)
ND (II-IV)
SND (II-V, postauricular, suboccipital)
ND (II-V, postauricular, suboccipital)
SND (level VI)
ND (VI)
4.
Extended neck dissection
4.
ND (levels removed, nodes or structures removed)
Lastly, the surgeon must orient the surgical specimen for the pathologist and identify the different lymph node groups it contains. Only then can the pathologist be expected to generate a clinically and prognostically meaningful report that describes the location and number of lymph nodes examined, the number of nodes that contain the tumor, and the presence or absence of extranodal extension of the tumor.
ND (I-V, SCM, IJV, CN XI)
Radical Neck Dissection
This operation is defined as the en bloc removal of the lymph node-bearing tissues of one side of the neck, from the inferior border of the mandible to the clavicle and from the lateral border of the strap muscles to the anterior border of the trapezius. Included in the resected specimen are the spinal accessory nerve, the IJV, and the SCM (Fig. 117.5). A comprehensive description of the surgical technique of this operation was recently provided by McCammon and Shah (34).
Rationale
The first description of the systematic en bloc removal of the lymphatics of the neck was published by Crile in 1906. The operation he described came to be known as the RND. Although Crile believed that removing the IJV was essential because of the intimate relation of this structure with the lymph nodes of the neck, it is interesting to note that the drawings that illustrate his publication indicate that the spinal accessory nerve and the ansa hypoglossi were preserved. It was Martin et al. in the 1950s who championed the concept that a cervical lymphadenectomy for cancer was inadequate unless all the lymph node-bearing tissues of one side of the neck were removed and that this was impossible unless the spinal accessory nerve, the IJV, and the SCM were included in the resection. In fact, they categorically stated, “any technique that is designed to preserve the spinal accessory nerve should be condemned unequivocally.”
In describing the RND, Crile contended that an en bloc removal of the primary tumor and the lymphatic system of the neck should be carried out in a manner similar to the Halstead operation for breast cancer. He believed that normal lymph flow is interrupted by metastasis in a lymph node, causing further tumor dissemination to occur in any direction, and that a less radical “incomplete” operation would disseminate and stimulate the growth of the tumor. Like Crile, Martin et al. believed that it was impossible to remove the lymphatics of the neck completely without resecting the SCM and IJV because of the close association of the lymphatics in this area with the vein walls.
Removing the SCM unquestionably facilitates access to the jugular vein and the removal of the lymph node-bearing tissues of the neck. In some instances, the muscle must be removed because it is involved by the tumor. However, removal of this muscle is no longer justified for ease or exposure alone.
Figure 117.5 Radical neck dissection.
An RND is not indicated in the absence of palpable cervical metastases (i.e., in the treatment of the N0 neck). Currently, RNDs represent less than 20% of all neck dissection done at many institutions (35), as familiarity with the other types of neck dissection has increased.
Indications
An RND is indicated when there are multiple clinically obvious cervical lymph node metastases, particularly when they involve the lymph nodes of the posterior triangle of the neck and are found to involve or to be tightly related to the spinal accessory nerve. An RND is also indicated when there is a large metastatic tumor mass or when multiple matted nodes are present in the upper part of the neck. In such instances, it is unwise to preserve the sternocleidomastoid or the internal jugular or to dissect the spinal accessory nerve and risk entering the tumor. A similar situation can be created by the inflammation, hematoma, or ecchymosis that follows ill-advised excisional biopsies of neck metastases. An RND may be the safest option in such patients.
ND (I-V, SCM, IJV, CN XI)
Modified Radical Neck Dissection (MRND)
This category includes modifications of the RNDs developed with the intention of reducing the morbidity of the operation by preserving one or more of these structures: the spinal accessory nerve, the IJV, or the SCM.
The three neck dissections that can be included in this category are outlined in Table 117.3. They differ from each other only in the number of neural, vascular, and muscular structures that are preserved. Therefore, they can be subclassified as follows:
Figure 117.6 MRND (type I) with preservation of the spinal accessory nerve.
ND (I-V, SCM, IJV) (MRND type I) with preservation of the spinal accessory nerve
ND (I-V, SCM) (MRND type II) with preservation of the spinal accessory nerve and the IJV
ND (I-V) (MRND type III) with preservation of the spinal accessory nerve, the IJV, and the SCM. This corresponds to the operation often called “functional neck dissection.”
ND (I-V, SCM, IJV)
Modified Radical Neck Dissection with Preservation of the Spinal Accessory Nerve
This operation is defined as the en bloc removal of the lymph node-bearing tissues of one side of the neck, from the inferior border of the mandible to the clavicle and from the lateral border of the strap muscles to the anterior border of the trapezius, preserving the spinal accessory nerve. The IJV and the SCM are included in the resected specimen (Fig. 117.6). The surgical technique is essentially the same as that of the RND.
Rationale
The following observations have compelled surgeons, for several decades, to explore and develop alternatives to the RND:
The morbidity associated with the RND, especially the shoulder disability that results from the resection of the spinal accessory nerve and, to a lesser extent, the cosmetic deformity that results from this operation, particularly when it is done on both sides of the neck
The realization that in many instances the spinal accessory nerve is not in close proximity to the nodes grossly involved by the tumor and that its preservation does not compromise the oncologic soundness of the operation
Indications
This type of neck dissection is used in the surgical treatment of the neck of patients with clinically obvious lymph node metastases when the spinal accessory nerve is not directly involved by the tumor, regardless of the number, size, and location of the involved lymph nodes. The decision to preserve the spinal accessory nerve is, therefore, a delicate intraoperative judgment call. Much like the philosophy about preservation of the facial nerve during surgery for parotid tumors, the spinal accessory nerve can be preserved whenever there is a clearly identifiable, not an artificially created, plane of dissection between the tumor and the nerve. The reported rate of recurrence in the neck when used for the treatment of the N+ neck in combination with postoperative radiation is 8.1% (36).
ND (I-V, SCM)
Modified Radical Neck Dissection with Preservation of the Spinal Accessory Nerve and the Internal Jugular Vein
In this type of dissection, the lymph node-bearing tissues of one side of the neck are removed en bloc, preserving the spinal accessory nerve and the IJV. This operation is seldom planned. It is done occasionally when in the course of a neck dissection the metastatic tumor in the neck is noted to be adherent to the SCM but away from the accessory nerve and the jugular vein. This situation occurs occasionally in patients with hypopharyngeal or laryngeal tumors with metastases under the middle third of the SCM.
Figure 117.7 MRND (type III) with preservation of the spinal accessory nerve, the internal jugular vein, and the SCM.
ND (I-V, SCM, IJV, CN XI)
Modified Radical Neck Dissection with Preservation of the Spinal Accessory Nerve, the Internal Jugular Vein, and the Sternocleidomastoid Muscle
This operation consists of the en bloc removal of the lymph node-bearing tissues of one side of the neck, including lymph nodes in levels I through V, preserving the spinal accessory nerve, the IJV, and the SCM. The submandibular gland may or may not be removed (Fig. 117.7). A description of the operative technique of this operation, as it is currently advocated by most European surgeons, can be found in a publication by Gavilan et al. (37).
Rationale
The muscular and vascular aponeurosis of the neck demarcate compartments filled with fibroadipose tissue that contains lymph nodes. In the early 1960s, Suárez observed that the lymph nodes of the neck are not located within the muscular aponeurosis of the SCM and do not form part of the adventitia of nearby blood vessels, particularly veins. He then showed that it was technically feasible and oncologically sound to perform a comprehensive removal of the lymph node-bearing tissues of one or both sides of the neck without removing the SCM, the submandibular gland, and the IJV (38). It should be pointed out that the nerves of the neck do not follow the aponeurotic compartment distribution, except for the vagus nerve that is contained within the carotid sheath. The phrenic nerve and the brachial plexus are partially within a compartment; the hypoglossal and the spinal accessory nerves run across several compartments. Unless these nerves are directly involved by the tumor, they can be dissected free and preserved.
Indications
This operation was widely used, particularly in Europe, as the neck dissection of choice for the treatment of the N0 neck in patients with SCCA of the upper aerodigestive tract, especially when the primary tumor was in the larynx or hypopharynx. It is now considered an unnecessarily extensive procedure for the treatment of the clinically negative neck in patients with head and neck cancers. A multi-institutional prospective randomized study comparing MRND to ND (levels II-IV)) in patients with laryngeal cancer was performed by the Brazilian Head and Neck Cancer Study Group (39). All patients had previously untreated T2-T4 N0M0 supraglottic and transglottic squamous carcinoma. Pathologically positive nodes were found in 26% of the patients, and most positive nodes were located at levels II and III. There were six ipsilateral neck recurrences (four in the MRND group and two in the lateral neck dissection ND II-IV group). Five-year actuarial survival calculated by the Kaplan-Meier method was 72.3% in the MRND group and 62.4% in the ND (II-III) (log-rank test P = 0.312). Another prospective study and a recent retrospective study also support the practice of not dissecting level V in patients with clinically N0 laryngeal and hypopharyngeal cancers (40,41).
According to some surgeons, this operation is indicated for the treatment of the N1 neck, when the metastatic nodes are mobile and no greater than 2.5 to 3 cm. The reported rates of recurrence in the neck with this type of neck dissection range between 0% and 16.6% for the clinically N0 neck and between 3.7% and 25% for the N+ neck (42,43,44,45,46,47).
This type of MRND remains the operation of choice for most patients with differentiated carcinoma of the thyroid who have palpable lymph node metastases in the lateral compartment of the neck.
Selective Neck Dissections
The SNDs consist of the removal of only the lymph node groups at highest risk of containing metastases according to the location of the primary tumor, preserving the spinal accessory nerve, the IJV, and the SCM. There are four main types of SNDs:
SND of levels I-III or ND (I-III) (commonly referred to as “supraomohyoid” neck dissection) (Fig. 117.8) and SND of levels I-IV or ND (I-IV) (also referred to as “extended supraomohyoid” neck dissection). These are the neck dissections commonly used in the treatment of patients with SCCA of the oral cavity. The lymph nodes removed are those contained in the submental and submandibular triangles (level I), the upper jugular region (level II), and the midjugular region (level III). The posterior limit of the dissection is marked by the cutaneous branches of the cervical plexus and the posterior border of the SCM. The inferior limit is the omohyoid muscle as it crosses the IJV. Some surgeons prefer to perform an SND of level I-IV in cases with cancer of the oral tongue (48). For cancers of the oral cavity that are close to or involve the midline, either type of SND is done bilaterally, since the lymph nodes in both sides of the neck are at risk. These operations have been described in detail by Medina and Byers (49).
Figure 117.8 Supraomohyoid neck dissection.
SND of levels II-IV or ND (II-IV) (Fig. 117.9). This neck dissection, commonly referred to as the “lateral” neck dissection, is used in the treatment of patients with SCCA of the larynx, oropharynx, and hypopharynx. It consists of the removal of the upper (level II), middle (level III), and lower (level IV) jugular lymph nodes. The superior limit of the dissection is the digastric muscle and the mastoid tip. The inferior limit is the clavicle. The anteriomedial limit is the lateral border of the sternohyoid muscle. The posterior limit of the dissection is marked by the cutaneous branches of the cervical plexus and the posterior border of the SCM. For tumors of the supraglottic larynx and posterior pharyngeal walls, the dissection is often bilateral. A recent description of the technique of this operation has been provided by Khafif (50).
Figure 117.9 Lateral neck dissection.
SND of level VI or ND (VI). This operation is also called “anterior” neck dissection or “central compartment” dissection. It is used in the treatment of patients with cancer of the midline structures of the anterior inferior aspect of the neck and thoracic inlet, such as the thyroid, the glottic and subglottic regions of the larynx, the pyriform sinus, and the cervical esophagus and trachea. It consists of the removal of the prelaryngeal, pretracheal lymph nodes, as well as the PTLNs on both sides. However, using a single denomination (i.e., SND of level VI) to refer to any dissection of the lymph nodes in this region is confusing. For instance, if the surgeon elects to remove the prelaryngeal, pretracheal, and the right PTLNs, the operation would have the same designation as one in which only the left paratracheal nodes are removed. Therefore, until consensus is reached about grouping of the lymph nodes in this area (i.e., level VIA and VIB), it is best to describe the operation in terms of the specific lymph nodes removed (e.g., left thyroid lobectomy with dissection of level VI that included the pretracheal and left paratracheal nodes) (51). These operations have been described recently by Weber and Holsinger (52).
SND for cutaneous malignancies of the head and neck. The extent of the regional node dissection in patients with cutaneous malignancies depends on the location of the primary lesion and the lymph node groups that are likely to harbor metastases. For skin cancers originating from the posterior scalp and the upper-lateral aspect of the neck, the operation most commonly done is an ND (levels II-V, retroauricular, suboccipital), which is also known as the “posterolateral” neck dissection (Fig. 117.10). The superior limit of this dissection is the posterior belly of the digastric muscle and the mastoid tip anterior laterally and the nuchal line/ridge posteriorly. The inferior limit is the clavicle. The anteriomedial limit is the lateral border of the sternohyoid muscle. The posteriolateral limit of the dissection is marked by the anterior border of the trapezius muscle inferiorly and the posterior midline of the neck superiorly (53). The regional node dissection often performed for cutaneous malignancies originating from the periauricular skin, anterior scalp, and temporal region is an SND (parotid, facial and external jugular nodes, levels II, III, VA).
Rationale
In the 1960s, surgeons at The University of Texas MD Anderson Cancer Center modified the concept of the RND by selectively removing only those lymph node groups that, based on the location of the primary tumor, were at highest risk of containing metastases” (54). These operations were eventually called “SNDs” (55) and their current use is based on the following observations:
Figure 117.10 Posterolateral neck dissection.
1. Anatomic, pathologic, and clinical investigations (5,6,48,56,57,58,59,60,61,62,63,64) and recent prospective studies (39,40
Only gold members can continue reading. Log In or Register to continue