18 Vocal Fold Paralysis The principal function of the larynx is to protect the lower respiratory tract. In addition, the larynx facilitates Valsalva maneuver and phonation. These functions are maintained by coordinated action of intrinsic and extrinsic laryngeal muscles and are dependent on an intact neural supply. The term vocal fold paralysis (VFP) is often used to describe the immobile fold; however, an immobile vocal fold is not always paralyzed and may be fixed due to separate pathological process. Historically, no distinction has been made in the literature between neurogenic VFP and mechanical fixation, but their evaluation and management are very different. Until proven otherwise, VFP must be regarded as a sign of underlying disease and not simply as a diagnosis unto itself. Advances in diagnostic techniques, improved clinical assessments, and broadening treatment options have aided in understanding the etiopathogenesis and management of unilateral VFP. By contrast, advances in the treatment of bilateral VFP have been slow to follow. A wide range of disorders can cause VFP (Table 18.1). There is significant bias in the reported incidence of major causes of impaired vocal fold function. Incidence varies with geographical location1 and reporting institution. Traditionally, the etiology is divided into thirds, with one third due to tumor, one third traumatic (surgery), and one third idiopathic.2 This trend is changing, with extralaryngeal malignancy now taking a greater proportion and other surgical causes gradually replacing thyroidectomy as the leading cause of surgical trauma.3 This could be either due to improved diagnostics such as computed tomography (CT) and magnetic resonance imaging (MRI) or due to an increase in oncological skull base, neck, and chest surgeries.4 It is important to note that the laryngoscopic appearance of VFP does not reflect the site of lesion, type of injury, or prognosis. •Malignancy (20 to 40%): Tumors anywhere along the course of the RLN from the skull base to the larynx may lead to vocal fold palsy.3,5 Local tumors of the laryngopharynx can also fix the vocal fold or compress the laryngeal nerve. It is important to be aware that occult tumors in the thyroid, neck, chest, or mediastinum may also lead to VFP. •Surgical trauma (22 to 44%): Surgical trauma accounts for the largest proportion of unilateral lesions. Most are due to purposeful resection of the nerve, though a significant number result from accidental injury.4 Although incidence of recurrent laryngeal nerve (RLN) injury during thyroid surgery is decreasing, it remains the principal cause of iatrogenic injury.3,5 •Nonsurgical trauma (9 to 10%): Blunt and penetrating trauma to the neck and chest can result in nerve injury. Endotracheal intubation injury accounts for 7 to 11% of unilateral vocal cord paralysis3,6 and is the result of excessive cuff pressure, laryngeal mask injury, or hyperextension of the neck. The RLN is usually compressed between the lateralized arytenoid cartilage, thyroid cartilage, and the inflated cuff. The compression injury resulting in paralysis must be distinguished from the immobile vocal fold due to traumatic arytenoid dislocation. •Neurological causes (2 to 3%): Lesions of the cortex rarely give rise to isolated paralysis, whereas lesions involving the medulla or extending to the peripheral nerve produce a flaccid unilateral paralysis. Some of the common central neurological causes are cerebrovascular accidents, syringobulbia, multiple sclerosis, and parkinsonism.5,7 In children, neurological abnormalities such as Arnold-Chiari malformation, meningomyelocele, and hydrocephalus should be considered.8 Other rare conditions such as myasthenia gravis and Eaton-Lambert syndrome may give rise to VFP due to disorders of the neuromuscular junction. Many primary muscle disorders may present with laryngeal dysfunction such as polymyositis and dermatomyositis.9 •Inflammatory and infectious causes (2 to 3%): Laryngeal neuropathy leading to RLN paralysis can be caused by diabetes, rheumatoid arthritis, polyarteritis nodosa, gout, collagen vascular disease, mumps, and other viral diseases. Besides resulting in laryngeal neuropathy, it is important to understand that inflammatory disorders can also affect the cricoarytenoid joint or the larynx as a whole. For example, granulomatous diseases such as tuberculosis, syphilis, and sarcoidosis can affect the larynx locally or affect the laryngeal nerve in its course in the chest. Fibrotic lesions such as cicatricial pemphigoid, granulomatosis with polyangiitis (GPA + Wegener granulomatosis), and relapsing polychondritis can also affect vocal fold function. In young children presenting with a fluctuating polyneuropathy of the IX, X, and XII nerves, sarcoidosis may be an important cause.5 •Idiopathic (12 to 22%): Improved assessment techniques, in particular, advances in the contemporary cross-sectional imaging, have enabled more accurate diagnosis.5,10 This has resulted in the decrease of “idiopathic” causes from around 50 to around 20%. Table 18.1 Etiology of Unilateral Vocal Cord Paralysis
Etiology
Etiology of Unilateral Vocal Fold Paralysis
Surgical trauma • Head and neck ○Thyroid, parathyroid ○Esophageal ○Carotid end-arterectomy ○Cervical spine fusion ○Malignant resections ○Skull base surgery ○Posterior fossa surgery • Thoracic ○Thyroid ○Tracheal ○Cardiac surgery ○Mediastinal |
Nonsurgical trauma • Blunt/penetrating Injuries • Anesthetic intubation: excessive cuffpressure, laryngeal mask • Injury, hyperextension neck • Aortic aneurysm • Cardiomegaly |
Neurological causes • Amyotrophic lateral sclerosis • Bulbar/pseudo-bulbar palsy • Multiple sclerosis • Stroke • Poliomyelitis • Parkinsonism • Wallenberg syndrome |
Neoplastic • Thyroid/lung • Esophageal • Mediastinal • Vagal neoplasms |
Inflammatory and infections • Viral • Sarcoidosis • Diabetes • Systemic lupus erythematosus • Rheumatoid arthritis • Tuberculosis • Drug toxicity, e.g., vincristine, taxol, and organophosphates • Radiation |
Idiopathic |
Congenital |
Patient Evaluation and Assessment
The evaluation and assessment of VFP has evolved in the past few decades. Simpler protocols have now emerged replacing previous exhaustive ones. These are based on clinical evidence provided by extensive analysis of data in patients with VFP.3,5
History
As always, a thorough history of a patient is essential. Evaluation and assessment of the voice begins when the patient enters the physician’s office. It is of utmost importance to obtain a detailed history of the onset, duration, and severity of the dysphonia. Taking a history provides ample time to the physician to make a detailed assessment of the patient’s voice. Qualities such glottic fry, hard glottal attacks, breathiness, diplophonia, pitch breaks, phonation breaks, and tense phonation can be assessed.
Not only is the larynx involved in voice production, but it is also crucial in protecting the lower respiratory tract. Hence, the patient may also present with coughing and choking episodes, aspiration, stridor, dyspnea, dysphagia, or odynophagia. A history of intubation, head and neck surgery, or trauma is very important. Other pertinent medical questions include the presence of seasonal allergies, history of reflux disease, life stress, diabetes, and medications.
A specific vocal history is also important. Many patients who present for an initial evaluation of voice complaints are unfamiliar with questions of vocal use and hygiene. It is important for the physician to explain these concepts to the patient during the questioning to facilitate accurate responses and educate the patient. Questions should include voice demands at home and at work, recreational singing, and episodes of abuse such as shouting at sporting events. Smoking, water intake, caffeine intake, and environmental irritants should be documented. An occupational history is essential. The effect of voice change may be significant for professional voice users and may cause significant distress for the patient.
A patient with unilateral VFP typically presents with a hoarse or weak voice. Attempts to speak loudly will lead to rapid laryngeal and respiratory muscle fatigue and vocal endurance is diminished. The voice cannot be projected easily when there is background noise. Some may complain of an inability to sing. Others may have subclinical symptoms. A compensated VFP may come to light when there is a respiratory infection leading to delayed recovery of hoarseness, or even breathing difficulties. Sometimes, patients may complain of shortness of breath and inability to perform daily routine work. Some may complain of aspiration, especially to liquids. These complaints are due to incomplete glottic closure. Physical activity such as lifting, pulling, or pushing requires extra effort due to lack of Valsalva ability.
The mode of onset can also influence the presenting symptoms. Sudden onset may follow viral illness or following surgery, whereas gradual onset of symptoms may be due to tumor involving the path of the RLN. Tumor may arise anywhere from the posterior fossa to the mediastinum and questions should aim to elicit important clinical signs and symptoms to guide further investigation.
Physical Examination
A thorough physical examination is performed including a full and detailed cranial nerve examination. Inspection and palpation of the neck for masses, with particular attention to the thyroid gland, restriction of movement, excess muscle tension, and scars from previous surgery or trauma should be performed. Normal laryngeal vertical mobility and abnormal laryngeal tilt and fixity, if any, should be noted. During palpation of the neck, the laryngeal framework should be assessed. The “manual compression test” is an easy, noninvasive clinical procedure that can evaluate several voice disorders. The lateral manual compression test may be useful in determining whether a patient with a wide glottic gap from unilateral VFP or vocal bowing will benefit from a medialization thyroplasty.11
Dynamic and static laryngeal assessment is performed using flexible laryngoscopy, and ideally videostroboscopy. The laryngoscopic findings in a patient with unilateral VFP due to RLN involvement will reveal the paramedian position of the ipsilateral vocal fold with the opposite cord active on abduction and adduction. Complete immobility is usually seen. Rarely, decreased range of motion may be seen due to the pull of the interarytenoid, incomplete paralysis, or due to reinnervation of the RLN. The vocal fold may appear atrophic or “noodle-like.” The ventricle may look more capacious and the conus may demonstrate some loss of tissue fullness.
The arytenoid cartilage on the paralyzed side may have a prolapsed appearance tipping anteriorly into the airway, but this rarely causes airway obstruction in practice. This abnormal position of the cartilage may be mistaken for dislocation. Sometimes, the lax-infolded aryepiglottic fold may be drawn into the airway causing obstruction. All these features may give the paralyzed fold a shortened or bowed appearance. The paralyzed fold may also be at a lower vertical level compared with the functioning fold during phonation.12
The opposite mobile fold tends to adjust its length to match the paralyzed fold by shortening, so that the vocal processes are opposite each other. This compensatory mechanism closes the glottic chink, but abnormal configuration of the posterior glottis persists.
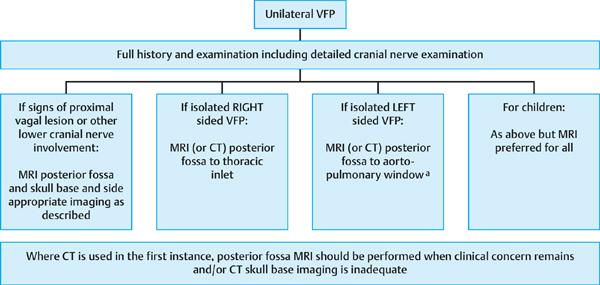
aProceed to formal chest imaging if any chest abnormality detected on screening scan.
The severity of the paralytic dysphonia is determined by the distance of the vocal folds from the midline, the degree of bowing, the size of the glottic gap, vertical relationships, and compensatory mechanisms.
Stroboscopy is useful in assessing the vibratory pattern of the vocal fold and provides valuable information on the effect of VFP on glottic closure. Vibratory patterns are influenced by the presence or absence of reinnervation, reduction in the mass of the vocal fold, and glottic gap.
Investigations
Over recent decades there has been a dramatic change in the investigation of patients with VFP. Historically, a comprehensive battery of tests was included in an attempt to evaluate all possible causes in a rather broad differential diagnosis. In recent years emphasis has been placed on a more focused approach based on the most probable cause.
Nearly one-third of the causes of VFP can be diagnosed on the basis of history of surgery and trauma alone,13 with the cause of the paralysis being evident at presentation.14
Tests relevant to the etiology or metabolic diseases are performed only if indicated from the history. Routine hematological studies have a low diagnostic yield and are not recommended routinely.
Radiology/Imaging
Modern imaging techniques are highly sensitive and a CT scan will detect masses not seen on a plain chest film. In cases where paralysis is limited to the left vocal fold with no detectable lesion clinically, a contrast CT covering the course of the RLN from the posterior fossa to the aortopulmonary window is indicated. For lesions on the right side, imaging should again include the posterior fossa and extend inferiorly as far as the clavicle. If other branches of the vagus are involved, or other cranial neuropathies are present, or if clinical doubt remains, then a gadolinium-enhanced MRI of the posterior fossa and skull base, neck, and if necessary the brain, is advised. If dysphagia coupled with the suspicion of an esophageal lesion is suspected (not due to aspiration), a contrast esophagogram or an esophagoscopy may be performed (Fig. 18.1).
Objective Measures of Voice
A more detailed description of objective measures of voice (Table 18.2) may be found in Section C, Chapter 10, “The Evaluation of Voice Outcome and Quality of Life Measures.”
Management Principles
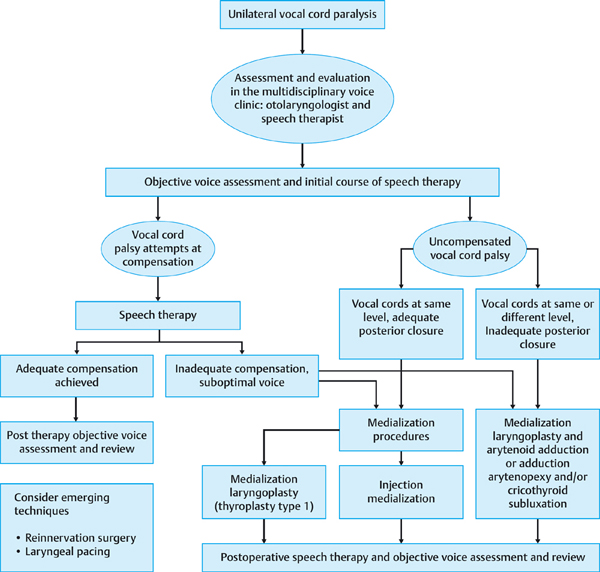
The management of VFP requires a multidisciplinary approach from otolaryngologists, speech therapists, voice coaches, and other professionals. Active patient involvement with clear, realistic goals is crucial. The specific management for a patient has to be tailored to his or her individual needs. An overview of the clinical management algorithm for patients with unilateral vocal fold palsy is shown in Fig. 18.2.
Table 18.2 Objective Measures of Voice That May Be Considered for Patients with VFP
Measure | Description | Effect of VFP on Measure |
Phonation airflow | •Airflow rates in speech are measured. •Useful in pre- and postoperative evaluation of thyroplasty or arytenoid adduction procedures. | •Elevated in unilateral VFP due to air escape. |
Subglottal air pressure16 | •Evaluation of the pressure in the subglottis (the opening force for vocal fold oscillations) •Useful in assessing the ability of the vocal fold to close effectively to contain the subglottal pressure and the available air resource. | •Reduced due to air escape. |
Maximum phonation time | •Thought to give an index of glottal efficiency. •Refers to the maximum length of time which a patient can sustain a vowel sound on a single breath. •May be difficult to interpret. •Restoration of the glottic closure can dramatically increase the MPT to normal levels17 | •Reduced due to air escape. •Normal values > 20 s. •In VFP values of < 12 s are typical. |
Acoustic assessment | •Objective recording of the salient perceptual characteristics of voice such as the average fundamental frequency (F0) and intensity, the amount of harmonics noise ratio and the percentage of perturbations (jitters and shimmers) •Integral in the evaluation of the voice in patients with VFP18 | •Variable. •Useful for baseline analysis and to assess response to treatment. |
Laryngeal EMG19 | •Addresses important questions such as the prognosis of return of vocal fold function.20 •Allows differentiation of neurogenic paralysis from mechanical vocal fold fixity. •Helps pinpoint the site of a neurological lesion and aids in the identification of incomplete neural injury or synkinesis. •Assists in determining the timing and type of surgery on the paralyzed fold. •In post-reinnervation surgery, the EMG is helpful in demonstrating return of function/innervation of the paralyzed muscles.21 | •No polyphasic reinnervation potentials at 6–12 wk postinjury suggests good prognosis and observation versus temporary injection augmentation of the fold can be considered. •If by 3 mo reinnervation is not demonstrable on EMG, early medialization surgery may be undertaken, rather than waiting the standard 6 mo to 1 y. |
VFP, vocal fold paralysis; s, second(s); EMG, electromyography; wk, week(s); mo, month(s); y, year.
The initial assessment in the multidisciplinary voice clinic confirms the presence of a VFP. Objective and subjective voice and laryngeal assessment with particular attention to the glottal chink and level of the vocal folds are performed. Many patients with small glottic defects will benefit from early speech therapy. Subsequent management depends on the initial response to speech therapy intervention, and further therapy is indicated in those cases where the normal vocal fold is attempting to compensate adequately. In this situation, surgical intervention may be avoided.
In those cases where the voice is found to be suboptimal and compensation unlikely to occur, appropriate surgical management is considered. Various surgical techniques have been developed ranging from open thyroplasty to endoscopic injection techniques. Recent evidences suggest a combination of techniques give better results.22
Injection Medialization
(Please refer to section “Injection Medialization Procedures for the Vocal Fold,” in Chapter 14 for detailed description of technique and materials.)
Injection medialization was introduced in 1911 by Bruenings.23 The principle is to medialize the paralyzed vocal fold by injecting a substance lateral to the vocal fold. It remains the most common procedure performed for managing VFP. A variety of materials are available and can be broadly grouped into those providing a temporary or more permanent treatment effect. Examples include polytetrafluoroethylene (PTFE) (Teflon) paste, DuPont, United States) (rarely used nowadays), hydroxyapatite, collagens, and silicone, among others. Injections may be performed under general or local anesthesia. Local anesthetic techniques (with or without sedation) offer the advantage of direct auditory feedback and lessen the risk of overinjection with resultant airway compromise. Ultimately, the choice of material and the method of injection depend on expertise of the surgeon, availability of materials, patient factors, and cost.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


