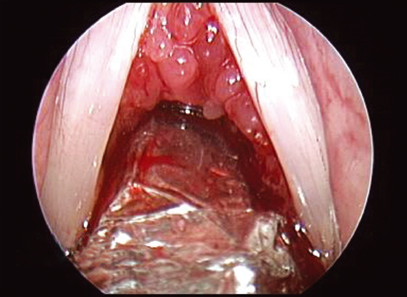
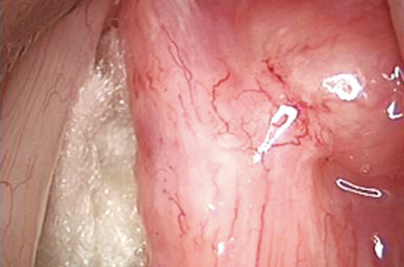
23 Granulomatous Diseases of the Larynx Ever since Manuel Garcia devised the laryngeal mirror in 1854, physicians began to develop an interest in diagnosing and localizing lesions of the larynx. There was a realization that all patients with an altered voice pattern need not have the same pathology. Infections, neoplasms, movement disorders, to name a few, gradually began to be diagnosed by visualizing the larynx and from thereon grew the science of laryngology. The term granuloma is derived from the Latin word “granulum,” referring to a small particle such as a grain. Such granulomas are formed as a result of a systemic immunological response to a specific or nonspecific antigen. Chronic granulomatous conditions of the larynx form a part of such systemic diseases with specific laryngeal lesions. Often, the physical presentations of these conditions mimic laryngeal cancer and hence early diagnosis is of utmost importance to ensure correct treatment. Among the granulomatous diseases affecting the larynx, the ones which are more clinically relevant for a laryngologist will be discussed and elaborated here. These include tuberculosis, sarcoidosis, fungal laryngitis, Wegener granulomatosis, leprosy, syphilis, and rhinoscleroma. As early as in the 17th century, Morgagni described laryngeal lesions caused by tuberculosis. Louis, in the mid-19th century, established the correlation between pulmonary and laryngeal tuberculosis and explained the pathophysiology of such laryngeal lesions. With the ever-increasing incidence of HIV and AIDS leading to an increase in the immunocompromised population, researchers have noted a resurgence in the incidence of tuberculosis in all its manifestations, especially the extrapulmonary variety.1 Laryngeal tuberculosis is a disease commonly affecting young adults. However, studies have shown an increasing incidence in patients in the fifth and sixth decades of life.2 Before the advent of highly efficacious antitubercular chemotherapy, the incidence of extrapulmonary tuberculosis was reported as nearly 30%,3 which has now decreased dramatically. Although laryngeal tuberculosis is now relatively uncommon (accounting for only up to 1 to 10% of all patients having tuberculosis),4 it is, nevertheless, the most common ENT manifestation of the disease, discounting cervical lymphadenopathy. Most chronic granulomatous diseases of the larynx present with hoarseness and vocal fatigue, occasionally associated with cough. Odynophagia and odynophonia are also commonly encountered symptoms. These symptoms stand true also for laryngeal tuberculosis. Most patients usually have coexistent cavitatory lesions in the lungs. Such patients may present with hemoptysis, breathlessness on exertion, and productive cough. Constitutional symptoms such as anorexia, weight loss, evening rise of temperature, and general debility in patients with chronic laryngitis are pointers toward suspecting tuberculosis. In the preantibiotic era, the most common cause of laryngeal tuberculosis was the pooling of secretions in the posterior glottis due to the patient being in the recumbent position. Perhaps for this reason, the posterior larynx was the commonest site of tubercular lesions of the larynx. In recent times, however, as morbidity associated with the disease has reduced, this theory no longer holds true. The spread of the disease to the larynx is thought to be more via the hematogenous and lymphatic route and hence we find lesions more anteriorly, especially over the vocal folds.5 Lindell et al6 have mentioned that the site of the disease is the true vocal folds in 47.1% of the cases, the epiglottis in 39.4%, and the false vocal folds in 29.2%. The disease may even spread to the pharynx, tonsils, or palate; however, its spread to the subglottis is uncommon. Diffuse asymmetric involvement of the vocal folds, which may be unilateral or bilateral, is the typical clinical picture seen in tubercular laryngitis. In the early stages of the disease, there are signs of severe and extensive inflammation and congestion over the vocal folds (Fig. 23.1). There is exudation and round cell infiltration in the subepithelial layers of the superficial lamina propria. The edematous-looking thickened epiglottis has been traditionally referred to as “turban epiglottis.”7 Hermani and Sawitra reported that exophytic lesions are more common than the ulcerative type.4 These lesions, especially if unilateral, might quite often be mistaken for a malignancy. Inflammatory infiltration eventually heals with fibrotic changes. A video laryngoscopic examination using a flexible laryngoscope or a 70-degree Hopkins rod examination is a must. It is important to note the site of the lesion, the involvement of contiguous structures, and also the impairment of vocal fold mobility, if any. A biopsy should be taken from the representative part of the lesion. Mycobacterium tuberculosis bacilli are detected on acid-fast staining of the biopsied tissue. Histopathology shows granulomatous foci intramucosally with lymphocytic infiltrate, epithelioid cells, and Langhans giant cells. Systemic evaluation for tuberculosis should be done in all patients and family members should be screened for possible infection. This includes routine investigations such as complete blood count (which reveals lymphocytosis and an elevated erythrocyte sedimentation rate [ESR]), tuberculin test, and sputum examination for acid-fast bacilli (AFB). Sputum-positive rates may be as high as 90 to 95%.5 Radiological investigations include plain radiographs of the chest and neck as well as computed tomography (CT) and MRI evaluation of the larynx. About 40 to 70% of patients had a fibrotic or fibrocavitatory lesion on chest X-ray.6 It is important to note that the integrity of the laryngeal skeleton is always maintained in cases of laryngeal tuberculosis, unlike malignancies. In untreated or inadequately treated cases, some amount of laryngeal stenosis or cricoarytenoid joint fixation may be noted. Due to the increasing trend of extrapulmonary tuberculosis in immunocompromised patients, all patients of laryngeal tuberculosis must be evaluated for HIV and AIDS. Once the diagnosis is confirmed, appropriate antitubercular chemotherapy should be immediately instituted. The standard HRZE (isoniazid, rifampicin, pyrazinamide, and ethambutol) regimen for extrapulmonary tuberculosis is started. The response to the treatment is usually quite good and, indeed, a favorable response to the therapy is a confirmation of the diagnosis. Monitoring liver enzymes during the treatment is important. Sarcoidosis is a multisystem disease of unknown etiology, characterized by noncaseating epithelioid granulomas. The respiratory system is affected in more than 90% of the cases with granuloma formation within the lung parenchyma as well as the hilar lymph nodes.8 Skin, liver, eyes, and heart are less frequently involved. Sarcoidosis of the upper airway is quite rare. As the pulmonary system is most commonly affected, patients most often present with a persistent dry cough or, in some cases, dyspnea on exertion. Constitutional symptoms such as fatigue and weight loss may also be seen. Pulmonary fibrosis is the most severe complication of the disease. Airway involvement in sarcoidosis initially manifests as mucosal edema, inflammation, and erythema with granuloma formation which heals with fibrosis. Endobronchial granuloma formation may take place which heals with fibrosis, ultimately giving rise to bronchial stenosis in 14% of the cases.8 Among the extrapulmonary manifestations, lymph node enlargement remains the commonest (about 70% of the cases), as with tuberculosis.9 Nasal passages, oropharynx, and larynx are affected in about 6% of sarcoidosis patients.10 Laryngeal lesions may be found on the epiglottis, aryepiglottic folds, false vocal folds, and subglottis (Fig. 23.2). The epiglottis and aryepiglottic folds are thickened with granularity and yellowish red nodule formation. Sometimes the nodular lesions in the supraglottic larynx will lead to airway obstruction and a tracheostomy may be required to relieve the stridor. The true vocal folds are less frequently involved.11 In contrast to tuberculosis, where laryngeal lesions are virtually always associated with a pulmonary focus, laryngeal sarcoid nodules can exist without any pulmonary infiltrates. Confirmation of the disease is only possible by doing a histopathological examination of the tissue. Noncaseating granulomas with a surrounding epithelioid reaction with lymphocytic infiltration are characteristic. Radiological investigations such as X-ray and high-resolution CT of the chest aid in diagnosing the systemic effects of the disease. Asymmetric pulmonary interstitial or parenchymal infiltrates, fibrotic changes with traction bronchiectasis, or luminal narrowing of the airway are noted. Hilar lymphadenopathy, compressing upon the airway causing luminal narrowing, may be seen. Bronchoalveolar lavage fluid shows lymphocytosis with a CD4*/CD8* ratio higher than 3.5 in 50% of the cases. Serum angiotensin-converting enzyme levels are raised and are found to correlate with disease activity.9 Figure 23.2 Granulomatous tissue seen in the subglottis of a patient of laryngeal sarcoidosis.
Laryngeal Tuberculosis
Clinical Features
Investigations
Treatment
Sarcoidosis
Clinical Features
Investigations
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


