12 Vitreous and Vitreoretinal Disorders
Anatomy and Embryology of the Vitreous
Rhegmatogenous Retinal Detachment
Differential Diagnosis of Rhegmatogenous Retinal Detachment
Special Types of Rhegmatogenous Retinal Detachment
Extraretinal Neovascularization
Macular Vitreoretinal Pathology
Macular Epiretinal Membrane (Pucker)
Principles of Vitreoretinal Surgery for Rhegmatogenous Retinal Detachment
ANATOMY AND EMBRYOLOGY OF THE VITREOUS
During early development the invaginated optic vesicle (optic cup) contains the primary vitreous, a vascularized tissue supplying the lens and retina, both of which are of ectodermal origin. During the third month of gestation the primary vitreous gradually loses its vascularity and is replaced by the secondary vitreous which is derived from the anterior retina and ciliary body. The principal remnants of the primary vitreous are Cloquet’s canal, a central tubular stucture that stretches sinuously between the lens and the optic disc and some epipapillary gliosis. In later life an exaggeration of the latter is seen as Bergmeister’s papilla and a Mittendorf’s dot is a primary vitreous remnant seen on the posterior lens capsule (see Ch. 17). The most common and severe developmental anomaly of the vitreous is persistent hyperplastic primary vitreous. This usually presents in infancy as a microphthalmic squinting eye with leukocoria. Pupil dilatation may demonstrate dragging of the ciliary processes towards a central plaque of fibrovascular tissue; this invades the lens posteriorly and ultimately causes complete cataract and secondary angle closure glaucoma (see Ch. 8).
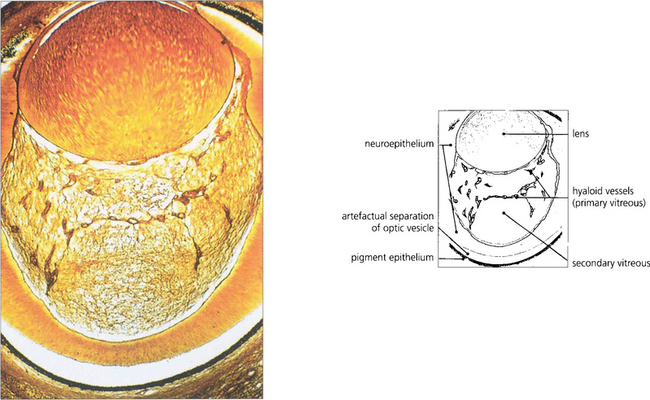
Fig. 12.1 Light micrograph of a section through the eye of a 13-mm human fetus showing primary and secondary vitreous with artefactual re-establishment of optic vesicle (silver stain).
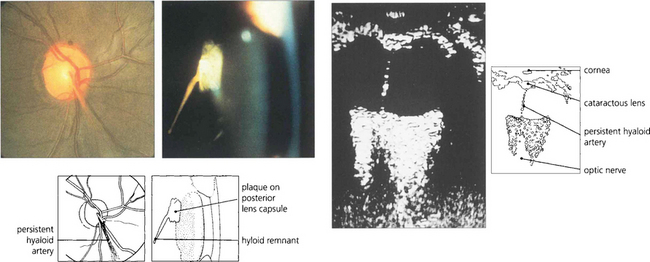
Fig. 12.2 The hyaloid artery may occasionally persist as a vascular channel between the central gel and optic disc (left), or as a glial plaque on the posterior lens capsule (centre). The B scan (right) demonstrates a persistent hyaloid artery.
VITREOUS CHANGES
POSTERIOR VITREOUS DETACHMENT
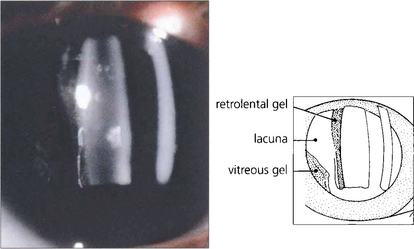
Fig. 12.4 With ageing vitreous degenerates to cause syneresis (condensation) and lacuna (cavity) formation and collapse. At slit-lamp examination the detached posterior hyaloid membrane looks like a wrinkled hanging curtain moving freely on eye movement. It separates from the retina up to the posterior border of the vitreous base (or the posterior aspect of any vitreoretinal adhesions).
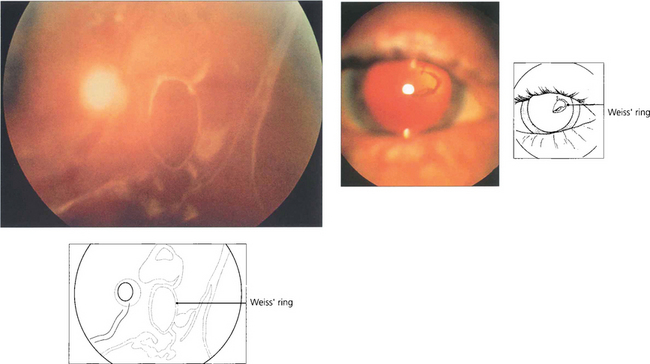
Fig. 12.5 On posterior vitreous detachment epipapillary glial tissue can become avulsed from the disc margin and is seen ophthalmoscopically as a ring of tissue on the detached posterior hyaloid interface situated in front of the optic disc (Weiss’ ring). The patient sees a circular or oval floater (depending on how it tilts) or describes a ‘cobweb’ or ‘spider’ that moves with the eye. Aggregations of collagen fibrils can also produce symptomatic floaters. ‘Lightening flashes’ may be seen in the temporal periphery, each typically lasting for a few seconds and induced by eye movement, possibly because photoreceptors depolarize when the vitreous base tugs on the retina; these flashes are often more noticeable on the transition from light to dark.
VITREOUS HAEMORRHAGE
The blood in the vitreous gel initially forms a localized clot but subsequently disperses throughout the gel following fibrinolysis. During haemolysis biconcave erythrocytes loose haemoglobin to become spheroidal erythroclasts. Biodegraded haemoglobin stains the gel ochre-yellow or orange. Erythroclast clogging of the vitreous cortex produces an ‘ochre membrane’ at the posterior hyaloid face. The mechanisms by which vitreous haemorrhage is spontaneously absorbed are not clear although phagocytosis by macrophages, outflow through the trabecular meshwork and syneretic disintegration of the gel play a part. Erythroclasts in the trabecular meshwork can reduce outflow to produce raised intraocular pressure and ‘erythroclastic glaucoma’ (see Ch. 8). Rarely, vitreous haemorrhage causes ‘synchysis scintillans’, a localized form of cholesterolosis bulbi characterized by cholesterol crystal accumulation in the vitreous cavity. The crystals sediment inferiorly but shower through the vitreous cavity with eye movement.
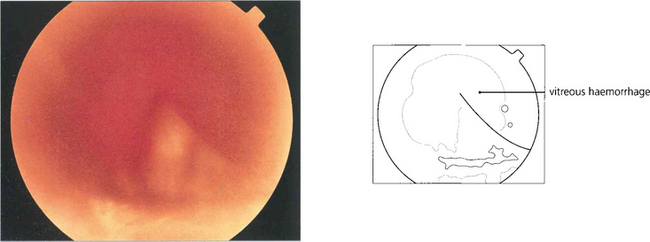
Fig. 12.6 A bulla of subhyaloid haemorrhage forces the posterior hyaloid face forwards into the vitreous cavity.
VITRITIS
Inflammatory cell infiltration of the vitreous is a feature of posterior uveitis, bacterial, viral, yeast and fungal infections, and intraocular lymphoma (see Ch. 10). Vitreous biopsy or vitrectomy has an increasing role in the management of these patients to obtain specimens for cellular diagnosis, microbial culture, removal of the vitreous scaffold and delivery of therapeutic drugs.
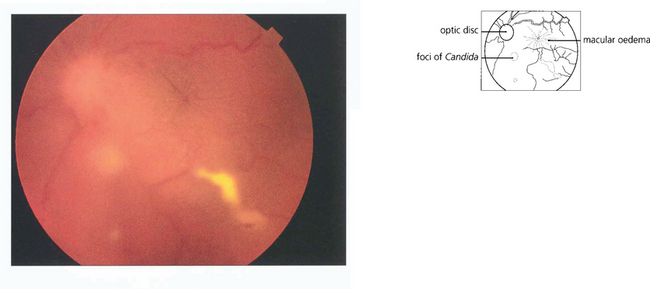
Fig. 12.8 Candidaemia in patients taking broad-spectrum antibiotics or with indwelling intravenous catheters or in intravenous drug users (Candida can grow in the lemon juice that may be used to dissolve heroin), carries a significant risk of metastatic endophthalmitis which manifests as intravitreal white puff-balls. Candida endophthalmitis, although more slowly progressive than bacterial endophthalmitis, usually requires vitrectomy to remove the infected gel, to administer intravitreal medication and to restore vision. Vitreous puff-balls are seen in this intravenous drug user with Candida endophthalmitis.
RHEGMATOGENOUS RETINAL DETACHMENT
FORMATION OF RETINAL BREAKS
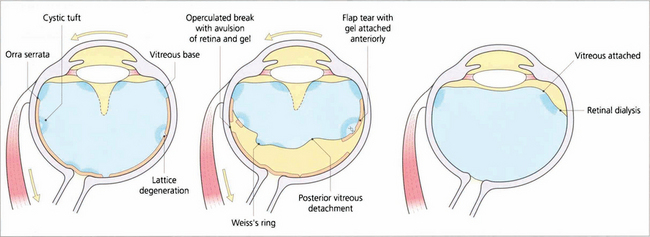
Fig. 12.11 Diagram illustrating the concept of dynamic vitreoretinal traction after posterior vitreous detachment and how this generates a flap-tear or an operculated tear. In contrast with a dialysis the vitreous remains attached and there is no posterior vitreous detachment.
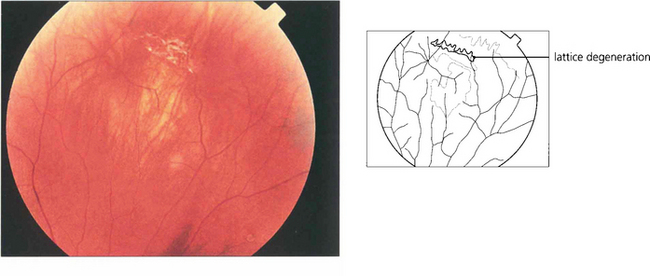
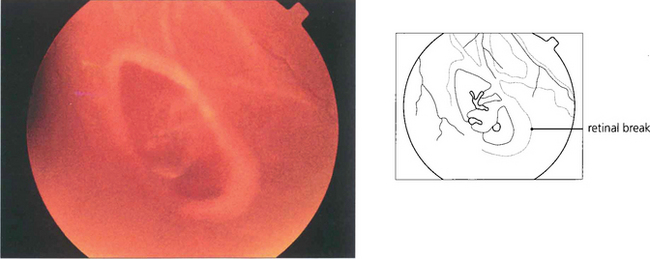
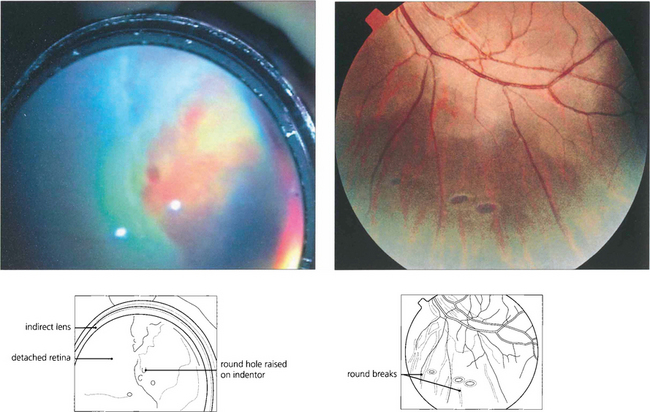
Fig. 12.15 Atrophic round retinal breaks are seen with an attached vitreous gel. They are usually equatorial and often associated with lattice degeneration. Recruitment of fluid with round hole detachment probably occurs by connection of the hole to vitreous lacunae; this may cause a stepwise detachment with multiple demarcation lines in a chronic-looking retinal detachment (see Fig. 12.24). The vast majority will not cause retinal detachment and prophylactic therapy is generally regarded as unnecessary.
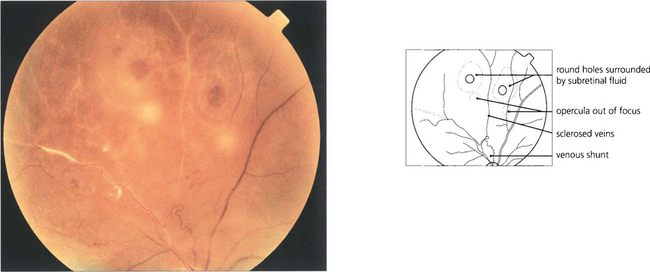
Fig. 12.16 Retinal breaks are seen in a patient with retinal vasculitis in whom the vitreous has separated avulsing small discs of retina that remain attached to the posterior vitreous surface as opercula. Round retinal tears result.
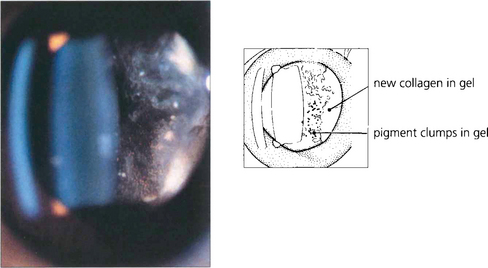
Fig. 12.17 Slit-beam photograph of the anterior gel after a retinal break showing RPE cells in the retrolental gel (the ‘tobacco dust’ or Shafer’s sign). Retinal tears are usually associated with release of RPE cells into the vitreous cavity and, when seen, suggest that a retinal break is present. This is of particular value when assessing a patient following an acute posterior vitreous detachment. These cells transform into fibroblast-like cells in proliferative vitreoretinopathy.