18 Strabismus
Strabismus is present when the foveas of both eyes are not simultaneously aligned on the object of regard; for distance fixation this means that the visual axes are not parallel. Strabismus is classified by the direction of the deviation: if the visual axes converge there is esodeviation; if they diverge there is exodeviation. If the visual axes differ in vertical direction there is hyperdeviation or hypodeviation, depending on whether the eye described is higher or lower than its fellow. Strabismus may be manifest—a ‘tropia’—if the deviation is present with both eyes open or latent—a ‘phoria’—when the deviation is demonstrable only with the eyes dissociated and binocular visual reflexes disrupted. Strabismus is concomitant when the angle of deviation remains constant (or nearly so) irrespective of the position of gaze or the eye that fixates or incomitant when the angle of deviation varies with the direction of gaze and fixing eye. Incomitant deviations are generally associated with ocular muscle paresis or mechanical restriction of rotation of the globe.
ANATOMY
Table 18.1 shows the primary, secondary and tertiary actions of the extraocular muscles. Torsional movements are described as intorsional or extorsional in relation to the midline.
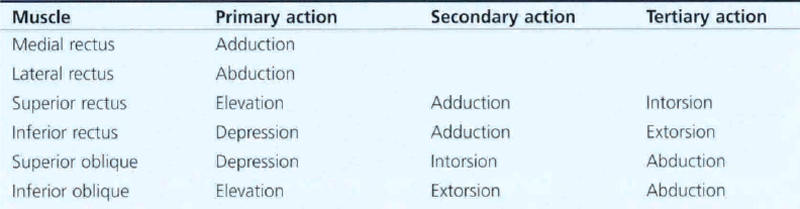
Fig. 18.1 The extraocular muscles consist of two layers: a ‘global layer’ adjacent to the globe, and the ‘orbital’ layer peripheral to this. (Left) Histology of the orbit of a 17-month-old infant stained with Masson trichrome shows the extraocular muscles suspended in blue orbital connective tissue. The orbital layer is more blue and the global layer more red. (Right) Higher magnification of the lateral rectus muscle shows collagen fibrils interspersed in the outer orbital layer; these fibrils are contiguous with the collagenous muscle pulleys of the orbit, explaining the layer’s bluish histological hue.
From Demer JL, Oh SY, Poukens V. Invest Ophthalmol Vis Sci 2000; 41: 1280–1290.
Fig. 18.2 Recent research has shown that the extraocular muscles are attached by connective tissue to the orbital septa just posterior to their insertion on the globe producing a dynamic pulley system that is believed to play an important role in positioning the globe by interacting with the actions of the orbital extraocular muscle layer. For example, on adduction, the medial rectus pulley is displaced posteriorly and the lateral rectus pulley anteriorly.
Reprinted with permission from Denser J F, Oh S Y, Poukens V. Evidence for active control of rectus extraocular muscle pulleys. Invest Ophthalmol Vis Sci 2000; 41:1280–1290. ©2000 Association for Research in Vision and Ophthalmology.
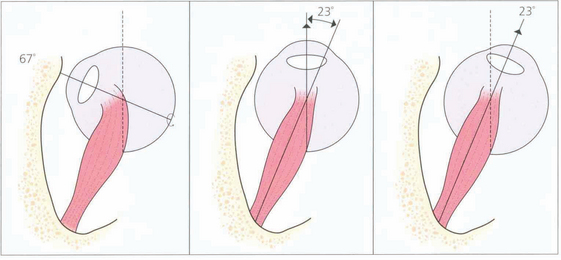
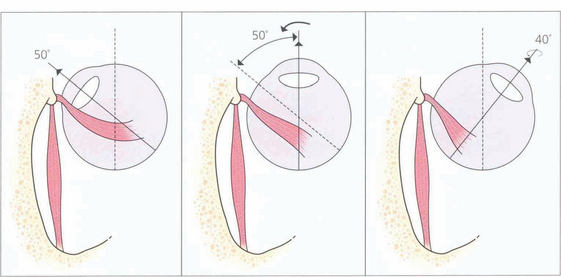
Fig. 18.3 The action of the two horizontal recti is the simplest to understand as they work around a common vertical axis. The action of the vertical recti is more complex because they attach medial to the vertical axis of the globe. As a result they produce pure elevation and depression only when the eye is abducted by 23°. Either side of that angle some torsion is also produced: in a more adducted eye the superior rectus produces more intorsion and the inferior rectus more extorsion. In addition, the vertical recti have a horizontal component to their action.
VISUAL ACUITY AND AMBLYOPIA
Measurement of acuity (see Ch. 1) is critical in the assessment and treatment of amblyopia and strabismus. It should be measured both binocularly and uniocularly, with and without correcting glasses and with and without associated head posture, particularly if nystagmus is present. Testing acuity in children demands time and patience; the method depends on the child’s development (Table 18.2).
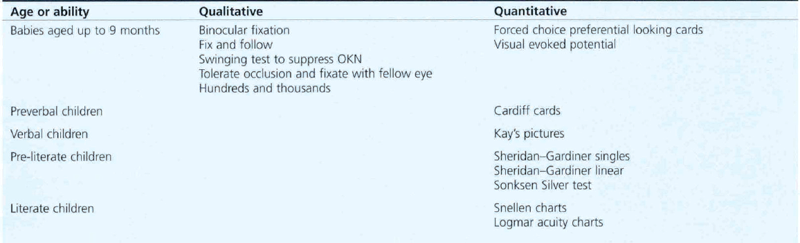
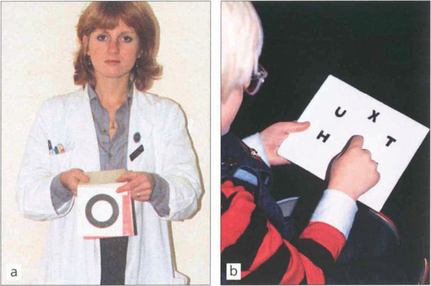
Fig. 18.5 The Sheridan–Gardiner test requires recognition rather than identification of letters and can be performed by cooperative children by the age of 2–3 years. The examiner has a flip-over book of the various Snellen sizes and the child identifies the letter. The main problem with this test is that acuity is overestimated because of the crowding phenomenon when acuity is better for single letters rather than rows.
BINOCULAR SINGLE VISION (BSV)

Fig. 18.6 The synoptophore can be used to assess the objective and subjective angle of horizontal, vertical and torsional strabismus. Each eye is dissociated and views an object that can be moved into each of the nine positions of gaze to test simultaneous macular perception, fusion, stereopsis and suppression. The objective angle of strabismus is measured by making the patient fixate each picture in turn and moving the tubes until there is no movement of the eye on fixation. This can also be measured by means of the prism cover test. The subjective angle is measured by letting the patient move the tubes so that he can perceive, for example, a bird in the cage. With normal retinal correspondence the subjective and objective angles are the same. With abnormal retinal correspondence the objective angle is the angle of deviation but the subjective angle is 0°.
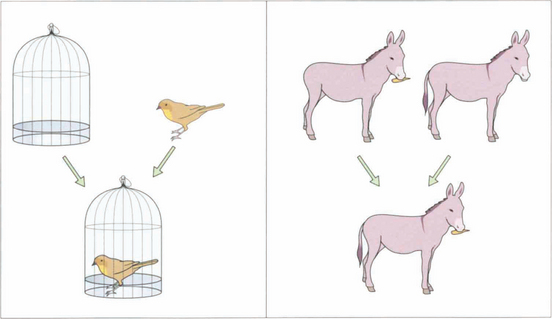
Fig. 18.7 To test simultaneous macular perception, different slides are presented to each eye (e.g. a bird and a cage). The patient is then asked to superimpose the images; for example, to put the bird into the cage. If the patient has no BSV, this will be impossible: the bird will jump from one side of the cage to the other (across the patient’s suppression scotoma). Sensory fusion is tested by getting the patient to superimpose two images that are similar but have uniocular controls. For example, one eye sees a donkey with no tail and a carrot, the other sees a donkey with a tail and no carrot. The tubes are converged and diverged until either the patient gets diplopia or one of the uniocular controls disappears. A normal person has a broad horizontal fusional range of 30Δ eso to 15Δ exo and a narrow vertical range of 3° (Panum’s fusional area). Diplopia is experienced outside these limits. Motor fusion is the ability to use both eyes to fuse similar images through a range of vergences (i.e. convergence and divergence, fusional convergence will control an exophoria and divergence an esophoria. It is usually tested with prisms but can also be tested on the synoptophore.
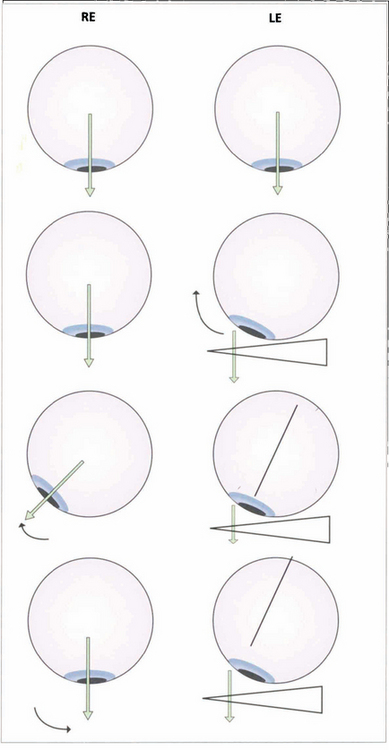
Fig. 18.8 Fusion can be tested with the 20D prism test in small children who cannot cooperate with the synoptophore. The diagram shows a 20D base-out prism being placed in front of the left eye so that the image is moved away from the fovea as the patient fixates a small target. The left eye adducts to maintain fixation. According to Hering’s law, the right eye will abduct but the child then appreciates diplopia and, to maintain BSV, makes an adducting movement of the right eye to overcome the effect of the prism.
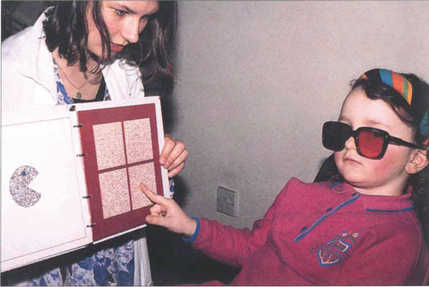
Fig. 18.9 There are a number of tests for stereopsis that rely on polarization or red-green goggles. The TNO test is a popular one in which the patient views an apparently random pattern of red and green dots through red and green glasses. The plates contain a stereo image and with stereopsis a geometrical shape is seen instead of the random pattern. This test has the advantage that it does not involve dissociation of the eyes and still works in colour-blind patients. Stereopsis is measured in seconds of arc; a person with normal vision can fuse more than 60 seconds of arc disparity.
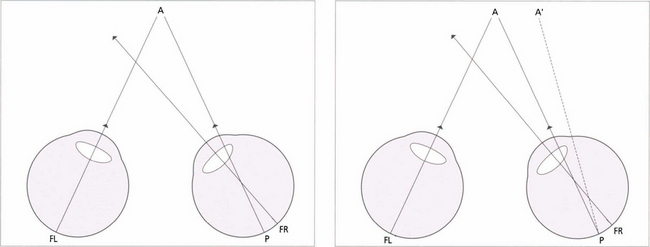
Fig. 18.10 Children with small-angle constant strabismus may develop an abnormal form of BSV known as abnormal retinal correspondence. (Left) This diagram of a small-angled constant right convergent strabismus shows an example of abnormal retinal correspondence: the fovea of the left eye (FL) corresponds to the pseudo-fovea (P) in the right eye, with the fovea of the right eye (FR) being suppressed when strabismus is of early onset. These patients tend to have some BSV despite their strabismus but there is usually mild amblyopia in the deviating eye and worse than 120 seconds of arc of stereopsis. (Right) In a late-onset strabismus the fovea of the right eye (FR) is not suppressed. The image falls at a point P in the right eye, it does not correspond to the fovea of the left eye (FL) and projects to A’. This results in diplopia.
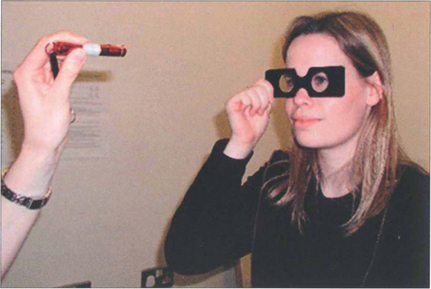
Fig. 18.11 Retinal correspondence is tested with Bagolini glasses which have micro-striations that produce perpendicular streaks of light perpendicular to each other in each eye when viewing a spotlight. A cross of light is seen with binocular vision; in the absence of strabismus this indicates normal retinal correspondence. When a cross of light is seen in the presence of strabismus this indicates abnormal retinal correspondence. If only one streak of light is seen this is consistent with suppression. If the patient sees two lights and two lines, diplopia is present. Worth lights, seen through red and green goggles, work on a similar principle.
AMBLYOPIA

Fig. 18.12 The age at which treatment starts is critical to success: the younger the child, the speedier the response and the better the prognosis for visual improvement. Treatment usually has to be completed by 6–7 years of age, when the visual system matures. The mainstay of treatment is the correction of any refractive error followed by occlusion of the eye with better visual acuity to stimulate the amblyopic eye. The duration of occlusion and the length of treatment depend on the child’s age and response to treatment. Visual acuity must be monitored carefully as there is a real risk of making the good eye amblyopic (occlusion amblyopia). Atropine occlusion is a reasonable alternative for mild and moderate amblyopia.
DIAGNOSIS AND EVALUATION OF STRABISMUS
Strabismus is sometimes associated with other signs, the most common of which is an abnormal head posture. When examining for abnormal head posture it is important that the patient fixates on a distant target. A cover test should be performed with and without the head posture. Not all abnormal head postures are adopted for ocular reasons (e.g. torticollis, vestibular disease, habitual), but those that are usually help the patient to achieve a limited area of binocular vision (Table 18.3). Occasionally a head posture will be used to separate images or to fixate with a better seeing eye.
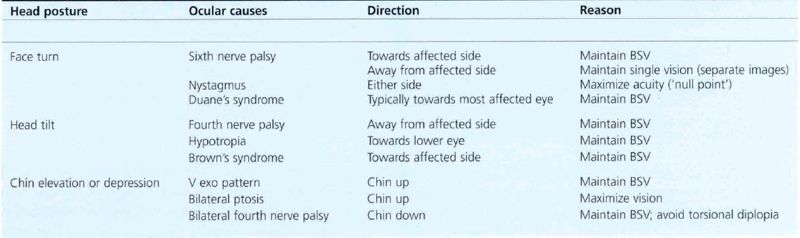

Fig. 18.13 It is extremely important to remember that strabismus is also commonly the presenting feature of structural eye disease. Most infantile strabismus is convergent. It is therefore important to beware of a constant exotropia in an infant—this may signify structural brain or ocular abnormalities. The most serious example of this is shown by this child with strabismus and leucocoria from a retinoblastoma. Exotropia is relatively common in children with hydrocephalus, intellectual impairment and inherited syndromes. Children presenting with an exotropia before the age of 1 year require both ophthalmic and neurological examination.

Fig. 18.14 Longstanding abnormal head postures of many years may cause secondary skeletal abnormalities such as scoliosis or facial asymmetry. This woman has relative maxillary hypoplasia associated with a congenital left fourth nerve palsy.

Fig. 18.15 Strabismus must be distinguished from pseudo-strabismus by demonstrating a manifest deviation on cover testing. Epicanthus is by far the commonest cause of misdiagnosed convergent strabismus. (a) A false impression of convergence is given, particularly on adduction, because the sclera is more covered medially. It should not be forgotten, however, that strabismus can coexist with epicanthus, as demonstrated in (b). Other causes of pseudo-strabismus include a wide interpupillary distance, facial asymmetry, enophthalmos and ptosis.
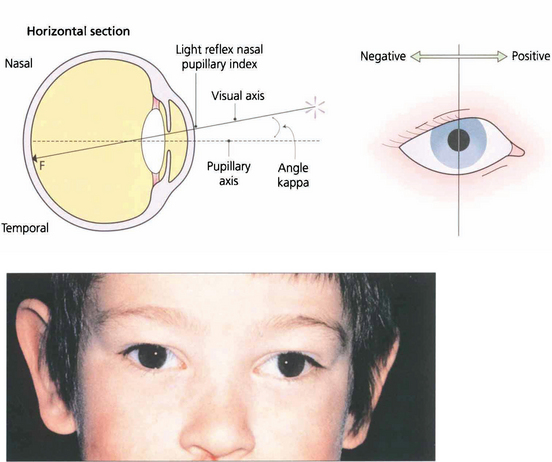
Fig. 18.16 Angle kappa is the angle between the visual axis and the line perpendicular to the cornea. It occurs because the fovea does not lie centrally on the anatomical axis but is usually slightly temporal to it; this accounts for the slightly nasal displacement of the corneal light reflex in a normal eye (normally about 4°). A large positive angle kappa, as in this child, gives an impression of divergent strabismus and a negative angle (which is unusual) denotes apparent convergence. The only way to distinguish between apparent and real strabismus is by a cover test. Angle kappa is also of considerable importance in corneal refracture surgery, which if centred on the pupillary axis can lead to post treatment aberrations and patient dissatisfaction.
THE COVER TEST

Fig. 18.17 This illustrates a cover–uncover test on a child with right esotropia. The fixating left eye is covered forcing the right eye to take up fixation (an interesting accommodative target should be used—a light is insufficient). On removing the cover the right eye does not hold fixation and fixation is preferentially taken up by the left eye again. It can be inferred that the left eye has better acuity than the right eye. The speed and accuracy of refixation gives information about the difference in acuity (faster with better acuity) and also shows the direction and degree of strabismus.

Fig. 18.18 In this child fixation changes from the right to left eye following cover and persists on uncover. This is called alternation; it signifies equal or nearly equal acuity in the two eyes.
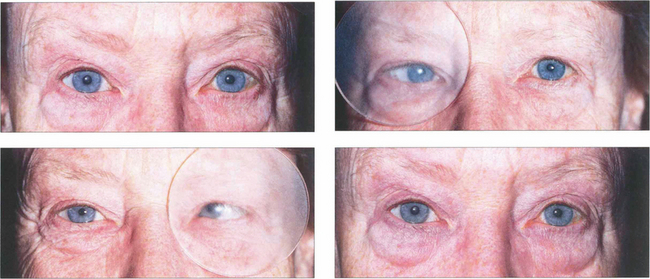
Fig. 18.19 With latent strabismus (phoria) the eyes are straight but tend to deviate if binocular reflexes are interrupted. An alternate cover test detects latent strabismus. In this patient with latent esophoria the right eye becomes convergent when occluded by the Spielman occluder (this is a frosted occluder that is sufficiently opaque to blur vision but allows eye position to be seen through the occluder). When the cover is rapidly transferred to the left eye the right eye refixates and the left becomes convergent. The cover must be moved from one eye to the other without allowing for refixation during the test; several passages are usually needed to dissociate the eyes fully and to reveal the full magnitude of the deviation. Removal of the cover restores binocular vision and allows the rate of binocular recovery and degree of control over the latent strabismus to be assessed. A cover–uncover test of each eye in turn should be performed initially to elicit a manifest strabismus followed by the alternate cover test. Cover tests should be performed for near and distant fixation, with and without an associated head posture, and with and without spectacles.
MEASUREMENT OF STRABISMUS
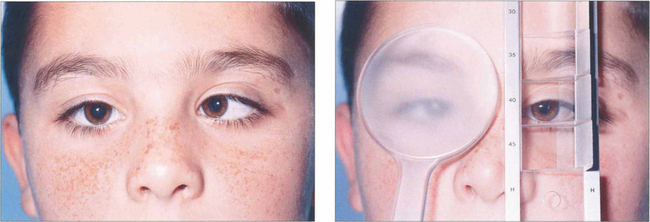
Fig. 18.20 In the prism cover test, a prism bar is used to increase the strength of the prism until there is no recovery movement on alternate cover testing. This is equal to the deviation, expressed in prism dioptres (1 prism dioptre (Δ)= ½° of angle). The test should be performed at 33 cm and 6 m and sometimes at 60 m (for intermittent exodeviations). If spectacles are normally worn the test should be performed both with and without them.




