20 The Orbit and Lacrimal System
ANATOMY OF THE ORBIT
The orbit is conical with a volume of approximately 27 ml. It contains the globe and the optic nerve, external ocular muscles, ophthalmic artery and its branches, orbital veins and nerves and the lacrimal gland. Orbital fat fills the remaining space and acts as a supportive cushion and fibrous septa run in planes between the ocular muscles and periosteum to support the orbital contents (see Ch. 18).
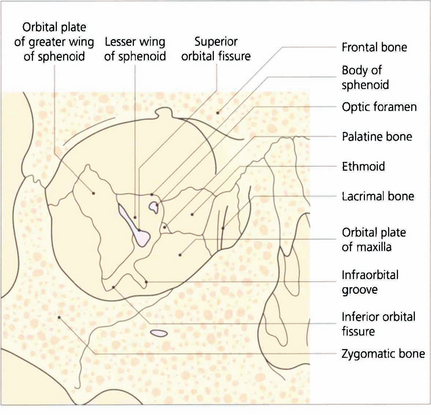
Fig. 20.1 Periosteum covers the orbital bones and adheres firmly at the anterior rim and at the apex around the optic canal. It is continuous with intracranial dura through the superior orbital fissure and optic canal. The lateral wall of the orbit is formed by the zygomatic bone and greater wing of the sphenoid. The frontal bone and part of the lesser wing of the sphenoid make up the roof. The fossa of the lacrimal gland lies superotemporally as a recess in the frontal bone, just above the junction with the zygoma. The floor is formed anteriorly by the maxillary process of the zygoma, centrally by the orbital plate of the maxilla and posteriorly by a small portion of the palatine bone. The infraorbital fissure lies between the greater wing of the sphenoid and the orbital plate of the maxilla and communicates with the pterygopalatine fossa posteriorly. The infraorbital groove carries the infraorbital nerve (Vb) and vessels. The medial wall is formed from anterior to posterior by the frontal process of the maxilla, the lacrimal bone (with the fossa of the lacrimal sac lying between), the ethmoid and the body of the sphenoid.
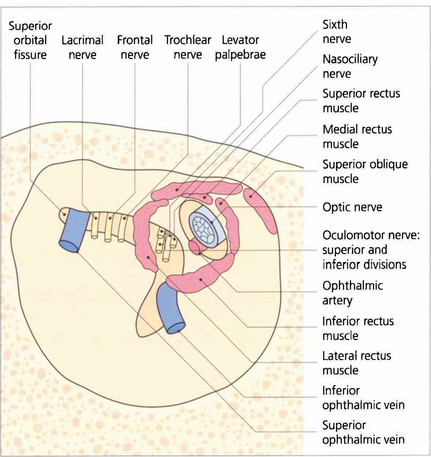
Fig. 20.2 The superior orbital fissure lies between the greater wing of the sphenoid inferiorly and the lesser wing superiorly (see Fig. 20.1). The lacrimal and frontal branches of the fifth nerve, the trochlear nerve and the superior ophthalmic vein are found superiorly and external to the annulus of Zinn; the superior and inferior divisions of the third nerve, the sixth nerve and nasociliary nerve lie within the annulus. The optic canal lies in the body of the sphenoid, medial and superior to the superior orbital fissure. It is lined with dura and transmits only the optic nerve and ophthalmic artery which lies inferior to the nerve. Space-occupying lesions at the orbital apex may compress the optic nerve and ocular motor nerves. Infiltrating lesions can spread through the superior orbital fissure into the cavernous sinus and middle cranial fossa to cause pain and loss of sensation in the distribution of the ophthalmic division of the trigeminal nerve. The sphenoidal sinus lies medial to the optic canal and the two are separated by extremely thin bone, which may even be absent, so that the optic nerve is easily damaged by surgery or disease within the sphenoidal sinus.
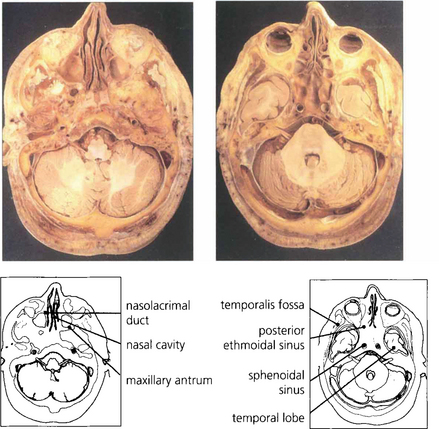
Fig. 20.3 The middle cranial fossa and temporal lobes lie posterior to the orbit and are separated from it by the sphenoidal wings. The temporalis muscles and fossa lie laterally and the maxillary sinus lies inferomedially.
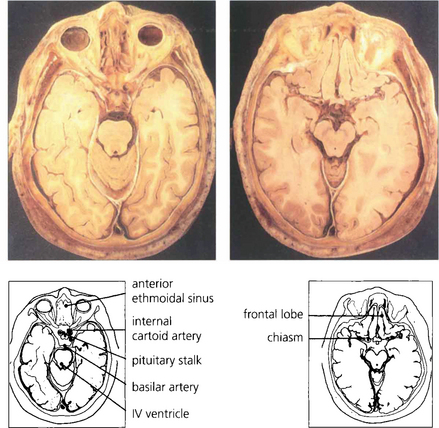
Fig. 20.4 Anatomical sections enable a clear correlation to be made between the orbital anatomy and the computed tomography (CT) appearance. Note the close relationship of the frontal lobes to the orbital roof, the anterior and posterior ethmoidal sinuses to the medial orbital wall and the sphenoidal sinus to the optic canal.
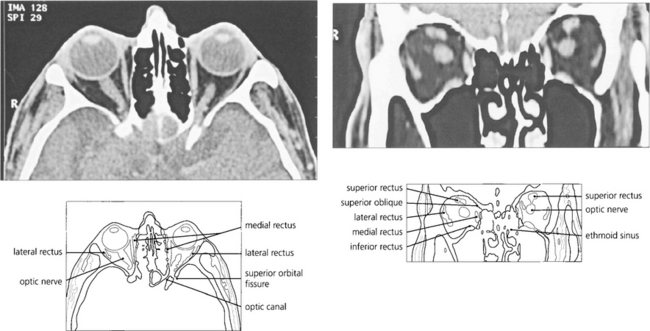
Fig. 20.5 CT scanning still has advantages over magnetic resonance imaging (MRI) in the orbit as the bony anatomy and calcification (an important sign of many pathological processes) is readily seen on CT. Axial scans taken along the line joining the external auditory meatus and inferior orbital rim cut the globe through the lens, optic nerve and optic canal in a single plane. The superior orbital fissure can be mistaken for the optic canal, which lies medially and superiorly, adjacent and medial to the anterior clinoid process. The optic nerve has a sinuous course within the orbit and cannot always be seen on a single cut if the section is thin. Similarly, partial sections of the ocular muscles may resemble a space-occupying mass at the apex if the scan is not interpreted carefully. Coronal scans are frequently much more informative and easier to interpret.
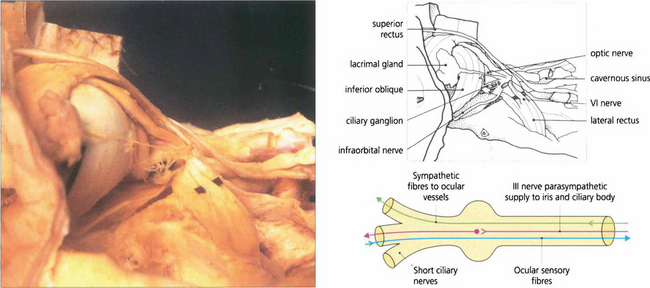
Fig. 20.6 A dissection of the lateral aspect of the orbit shows the orbital lobe of the lacrimal gland and its nerve. The lateral rectus muscle and sixth nerve are retracted to demonstrate the ciliary ganglion and short ciliary nerves. The ciliary ganglion (b) contains not only the synapses of the parasympathetic fibres to the iris and ciliary body from the third nerve, but also the efferent (and nonsynapsing) sympathetic fibres to the ocular blood vessels. Afferent sensory fibres from the cornea, iris and ciliary body pass through the ganglion to the nasociliary branch of the ophthalmic nerve.
ORBITAL BLOOD SUPPLY
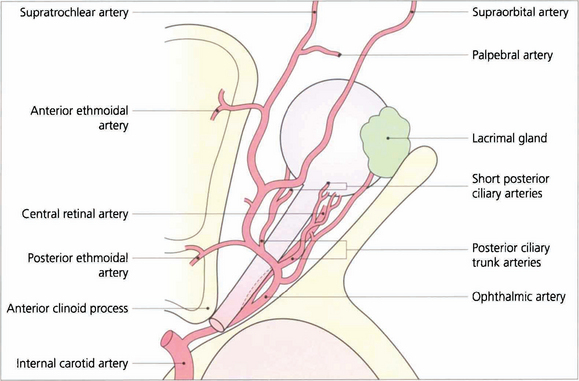
Fig. 20.7 The ophthalmic artery arises from the internal carotid artery immediately above the cavernous sinus and enters the orbit through the optic canal inferior to the optic nerve. It then passes laterally and superiorly over the optic nerve to give branches to the lacrimal gland and ocular muscles. The ophthalmic artery continues anteriorly and leaves the muscle cone to anastomose with branches of the external carotid artery in the lids, face and scalp. These anastomoses are of clinical importance if the internal carotid system is occluded.
The two posterior ciliary arteries leave the ophthalmic artery inferior to the optic nerve at the orbital apex. They pass forwards and divide before entering the globe around the optic nerve as several short posterior ciliary branches to supply the optic nerve head, retrolaminar optic nerve and choroid. The central retinal artery also arises from the ophthalmic artery and passes forwards and inferior to the optic nerve, to penetrate the nerve some 10–12 mm posterior to the sclera (see Ch. 17).
Fig. 20.8 The vortex veins from the choroid drain into the superior and inferior ophthalmic veins which flow into the cavernous sinus posteriorly and the pterygopalatine plexus inferiorly. Apsidal veins join the superior and inferior ophthalmic veins in the orbit. Anteriorly the orbital veins communicate with the frontal vein draining the scalp to form the facial vein which then drains into the external jugular vein. Orbital veins do not have valves and the intracranial and extracranial venous systems communicate freely explaining the facility with which infection can spread intracranially from the orbit. A distended superior orbital vein is seen as a neuroradiological feature of caroticocavernous fistulas
Adapted from Snell RS, Lemp MA. Clinical Anatomy of the Eye. ©1989 Oxford: Blackwell Scientific Publishers.
Table 20.1 Causes of orbital disease
| Children | Adults |
|---|---|
| Orbital cellulitis | Trauma |
| Dermoid and epidermoid cysts | Thyroid eye disease |
| Capillary haemangioma and lymphangioma | Idiopathic orbital inflammatory disease (formerly known as ’pseudotumour’) |
| Neurofibroma* | Lacrimal gland inflammation and tumours |
| Rhabdomyosarcoma* | Cavernous haemangioma |
| Optic nerve glioma* | Varices and lymphangioma |
| Leukaemia* | Lymphoma and lymphoproliferative disease |
| Meningioma (optic nerve or sphenoid wing) | |
| Metastases |
CAUSES OF ORBITAL DISEASE
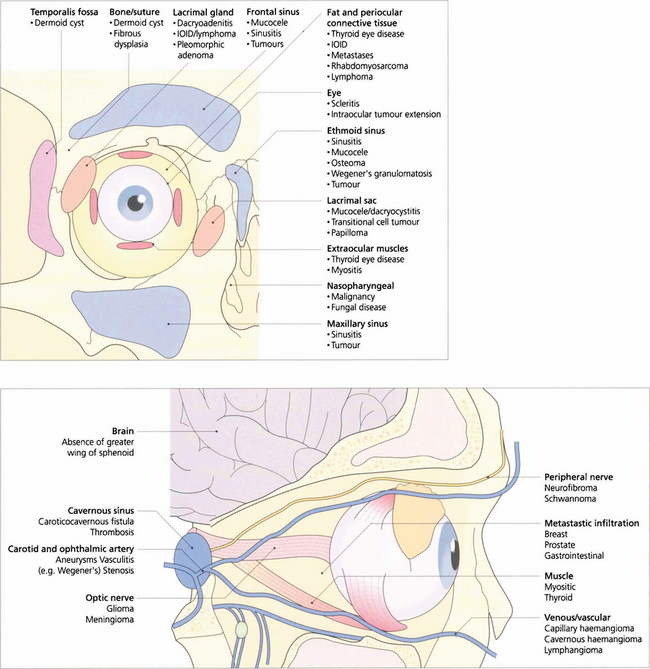
Fig. 20.9 Orbital disease may arise from abnormalities of the normal constituents of the orbit, contiguous spread of disease from adjacent structures, or invasion from haematogenous spread.
EXAMINATION OF THE ORBIT
Proptosis must be distinguished from pseudo-proptosis due to enlargement of the globe, congenital bony deformity or facial asymmetry, enophthalmos of the fellow eye and lid disease such as retraction. Ptosis will occasionally present as ‘proptosis’ of the contralateral eye (see Ch. 2).

Fig. 20.10 The degree of proptosis is measured with an exophthalmometer. The feet of the instrument are placed on each bony lateral orbital margin and the distance between the feet (i.e. the distance between each lateral orbital rim) is recorded for future comparison. The eye of the patient and that of observer are aligned, corrected for parallax (the fellow eye must be occluded if a strabismus is present) and the degree to which the corneal apex protrudes in front of the lateral orbital margin is recorded. Protrusion of the corneal apex varies with facial anatomy and so there is no absolute normal value of proptosis although asymmetrical proptosis of 2 mm or more is usually considered significant.
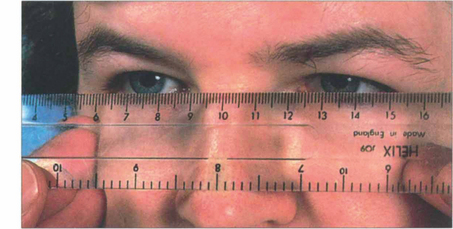
Fig. 20.11 Variation in ocular position and pulsatile proptosis should be sought where appropriate. Proptosis is axial if displacement is along the visual axis and nonaxial if displacement is off the visual axis. This can be judged by placing a clear plastic rule horizontally across the bridge of the nose to measure the horizontal and vertical positions of the visual axis of each eye. The fellow eye should be occluded when strabismus is present.
ACUTE PROPTOSIS

Fig. 20.12 Acute orbital cellulitis presents with fever and malaise, pain, proptosis, restriction of eye movements and conjunctival injection and oedema. This girl has an acutely swollen and painful left upper lid with the globe depressed from cellulitis in the superior part of the orbit secondary to a frontal sinusitis. Patients require hospital admission, nasal and blood cultures and intravenous antibiotics. These should not be delayed for investigations such as imaging. An orbital or subperiosteal abscess generally requires surgical drainage.
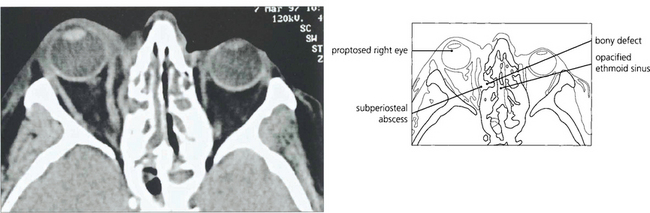
Fig. 20.13 CT scan from another patient showing an infective extension from the ethmoidal sinus into the orbit with a small subperiosteal abscess elevating the periosteum.
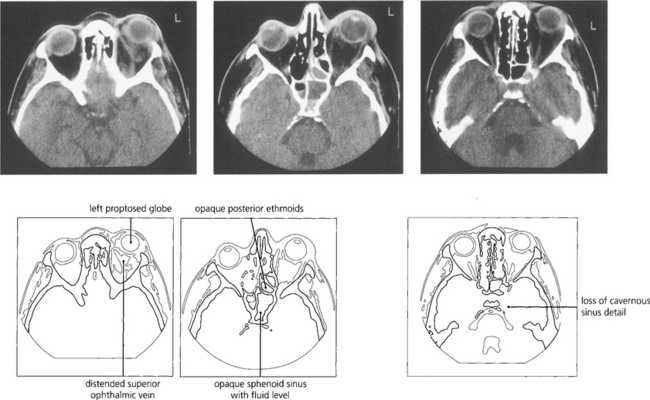
Fig. 20.14 Cavernous sinus thrombosis is now a rare complication of orbital cellulitis but must be considered when clinical signs progress rapidly with associated meningism, ocular motor and pupillary palsies, and signs of acute inflammation in the cerebrospinal fluid. MRI shows the thrombosis in the cavernous sinus better than CT.

Fig. 20.15 Embryonal sarcomas are tumours of mesenchymal cells with the potential to differentiate into striated muscle (striated or nonstriated rhabdomyomatous differentiation). They are commonly known as rhabdomyosarcomas although they do not arise from striated muscle. They are the commonest primary orbital malignancy of childhood. They can grow very rapidly; this child’s proptosis increased almost daily.
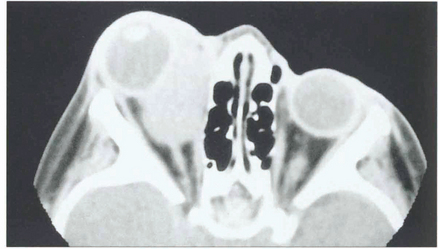
Fig. 20.16 CT scan showing a mass in the region of the medial rectus. After diagnostic biopsy treatment with radiotherapy and chemotherapy carries an excellent prognosis provided the tumour is confined to the orbit. These lesions can invade the orbital walls and metastasize haematogenously to the lung, lymph nodes and bone marrow.
CHRONIC AXIAL PROPTOSIS
THYROID EYE DISEASE
The commonest cause of axial proptosis is thyroid eye disease which can affect the orbits symmetrically or asymmetrically, with the latter producing apparently uniocular proptosis. Patients may be hypothyroid, euthyroid or hyperthyroid. T3, T4 and thyroid autoantibodies should be measured in all patients but about 15 per cent of patients have completely normal findings; in these patients the diagnosis is made clinically and by CT. Patients should be assessed for cosmesis, corneal exposure, diplopia and optic nerve involvement, all of which may occur independently of each other. Patients may have sore, irritable or watery eyes from exposure keratopathy, superior limbic keratitis (see Ch. 5) or disturbance of tear film metabolism. Smoking has been shown to be a significant risk factor for the development of dysthyroid eye disease which may also deteriorate at the time of treatment of hyperthyroidism with I131.
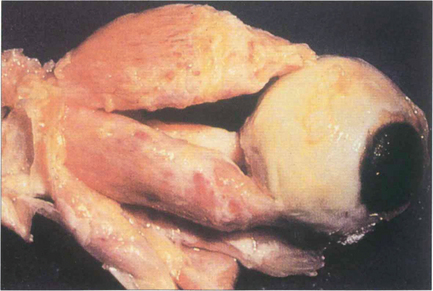
Fig. 20.17 Pathologically, dysthyroid eye disease affects the external ocular muscles rather than their tendinous insertions in contrast to idiopathic myositis. In the early stage inflammatory cells infiltrate the muscle belly causing oedema; as the disease progresses, collagen and glycosaminoglycans are produced by endomysial fibroblasts. Chronically, the muscles become fibrotic from contraction of the collagen and infiltrated by fat and may be expanded by up to eight times their normal size.
By courtesy of Dr R Eagle.
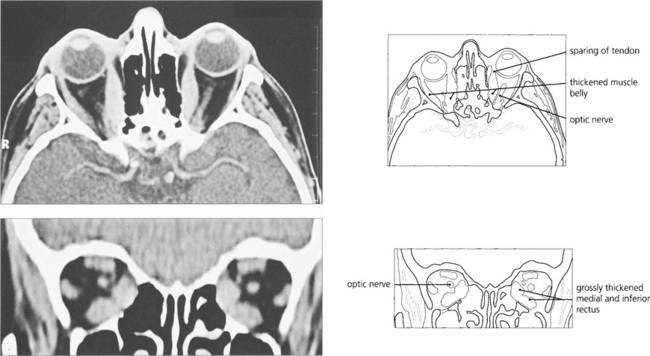
Fig. 20.18 Axial and coronal CT scans demonstrate thickening of the extraocular muscles. The medial and inferior recti are preferentially involved. Note that the muscle tendons are spared.


Fig. 20.20 Symmetrical and inactive (‘burnt-out’) thyroid eye disease. This patient has bilateral proptosis, and upper and lower lid retraction. Upper eyelid retraction is attributed to excessive sympathetic stimulation of Müller’s muscles and fibrosis of the levator complex.

Fig. 20.21 Asymmetrical orbital involvement is extremely common. Dysthyroid eye disease is common in young women. The cosmetic aspects of the disease cannot be overemphasized.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


