17 The Optic Disc
THE NORMAL OPTIC DISC
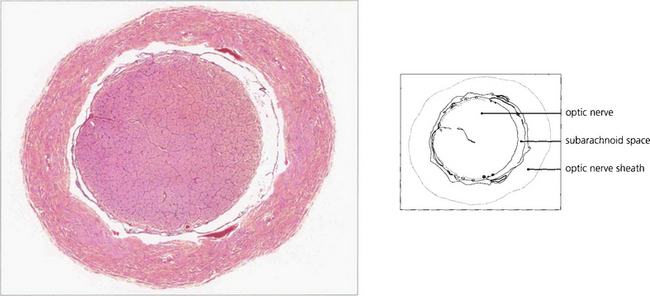
The scleral opening is rigid and nonexpansible. Behind the cribriform plate the axons acquire a myelin sheath and the optic nerve enlarges to a diameter of 3–4 mm. The nerve fibres are arranged roughly topographically in both the retinal nerve fibre layer and the optic nerve (see Ch. 19). The optic nerve sheath is a continuation of the meninges and the axons in the nerve are divided into approximately 1000 bundles by fibrous septa (derived from the pia mater) which also carry centripetal blood vessels. The subarachnoid space communicates intracranially so that the nerves are surrounded by the cerebrospinal fluid (CSF) which transmits the intracranial pressure.
BLOOD SUPPLY
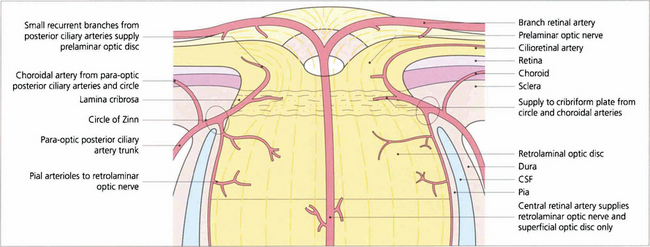
Fig. 17.1 Schematic diagram illustrating the arterial supply of the optic disc and distal optic nerve.
By courtesy of Miss Jane Olver.
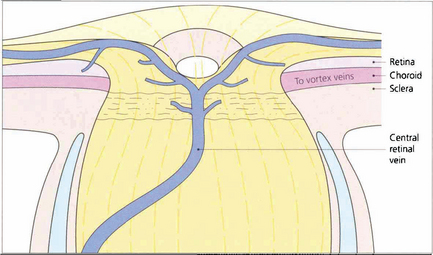
Fig. 17.2 Schematic diagram of the venous drainage of the retina, optic disc and distal optic nerve.
By courtesy of Miss J Olver.
Fig. 17.3 Digest preparations of a human optic disc. (Left) Posterior view showing the circle of Zinn which sends branches to the peripapillary choroid, the retrobulbar nerve and recurrent branches to the prelaminar region. (Right) A lateral view shows the circle of Zinn providing branches to the choroid and retrobulbar nerve.
Reproduced by permission of ED of IOVS.
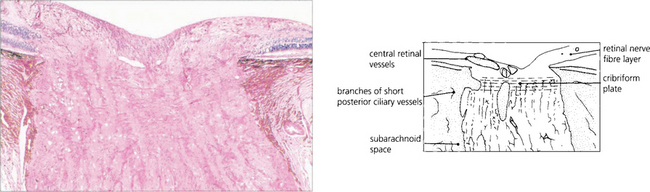
Fig. 17.4 Low-power micrograph showing an anteroposterior section of the distal part of the optic nerve, disc and retina. There is a considerable increase in the transverse diameter of the optic nerve after it passes through the sceral canal due to myelination. This is mostly completed by about the time of birth, although there is possibly some increase in myelination during the first two decades of life.
CONGENITAL ABNORMALITIES OF OPTIC DISC SIZE AND SHAPE
GLIAL REMNANTS
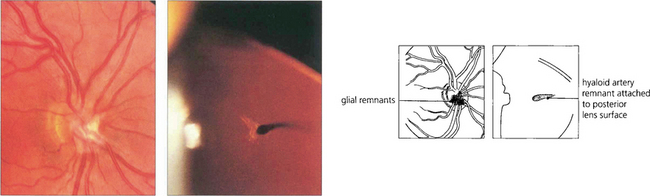
Fig. 17.6 Glial remnants are derived from either hyaloid artery remnants or vitreous condensations and lie in front of the blood vessels (left). Depending on their form and distribution they can simulate swelling or tumours of the disc. Occasionally, fibrous remnants of the hyaloid artery can be seen in the vitreous, sometimes attached to the posterior pole of the lens (right). Remnants of the embryological tunica vasculosa lentis are sometimes seen more peripherally on the lens as a Mittendorf dot (see Ch. 12).
COLOBOMAS OF THE DISC
A coloboma is a congenital defect resulting from a malclosure of the fetal cleft. Colobomas vary in size and shape; the disc is usually larger than normal although it may contain fewer nerve fibres. Colobomas usually occur inferiorly with varying involvement of the retina and uveal tract (see Ch. 9). Colobomas are occasionally inherited in an autosomal dominant fashion and may also be a feature of a number of genetic and maldevelopmental syndromes such as the CHARGE syndrome (coloboma, heart defects, anal atresia, retardation of growth, genital and ear defects) which is caused by dysgenesis at 5–6 weeks’ gestation.
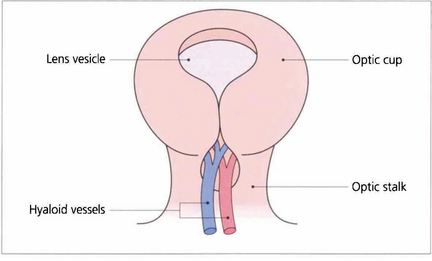
Fig. 17.7 The fetal fissure of the optic cup lies inferiorly and normally closes (starting at the middle and spreading anteriorly and posteriorly) at about 5–7 weeks of gestation. Defects in this process produce a coloboma. These can occur in many shapes and sizes, and typically involve the inferior temporal part of the disc and sometimes the retina and choroid.
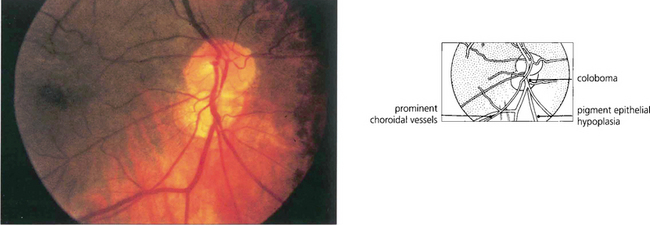
Fig. 17.8 A small coloboma of the disc associated with sectorial hypoplasia of the inferior retinal pigment epithelium in a pigmented eye. The disc appears slightly smaller vertically and is wider horizontally than normal. Choroidal vessels can be seen more easily through the thinned pigment epithelium inferiorly.
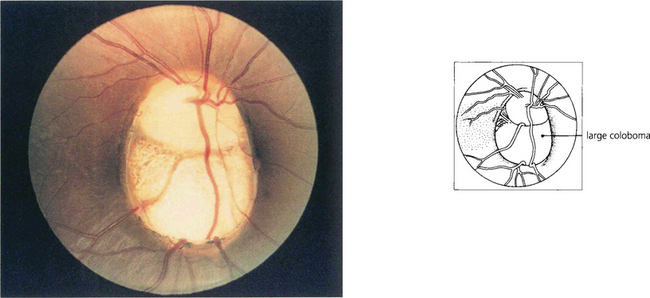
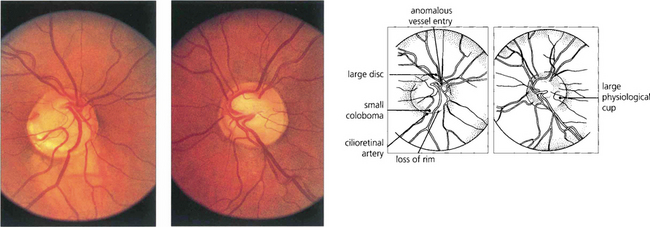
Fig. 17.9 A large coloboma of the disc. There may also be associated colobomas of the retina and choroid, lens or iris (see Ch. 9). A field defect is common and acuity may be poor if macular fibres are affected.
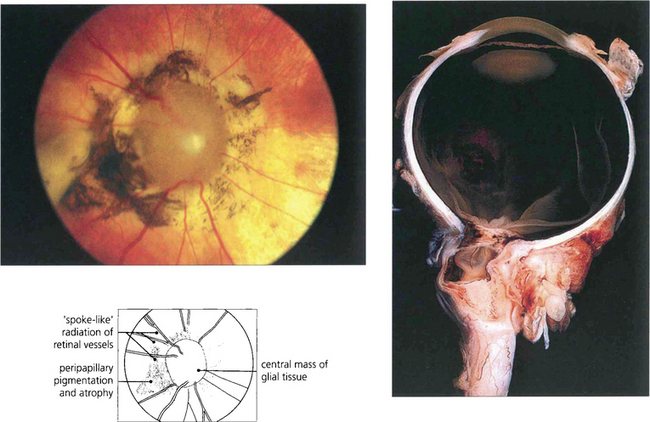
Fig. 17.10 A variant of coloboma is the morning glory disc. This rare congenital deformity of the disc is characterized by a mass of central glial tissue with radiating blood vessels, peripapillary atrophy and pigmentation. It is sometimes called a central coloboma of the disc. In these eyes the optic disc lies posterior to the globe ‘within’ the optic nerve, creating a funnel-shaped defect plugged by a central glial mass.
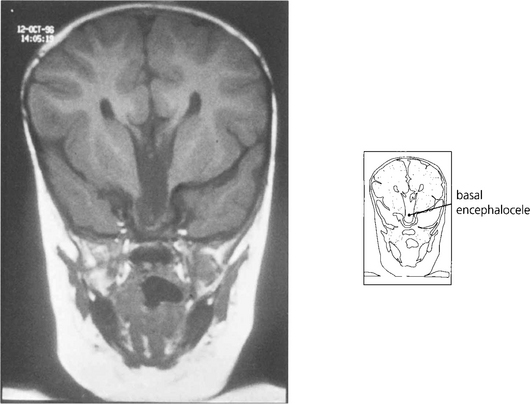
Fig. 17.11 In these patients the vision in the affected eye is poor and there may be associated midline intracranial anomalies such as a basal encephalocele. This is especially true if there are signs of malclosure of the fetal facial clefts, such as palatal deformity or telecanthus.
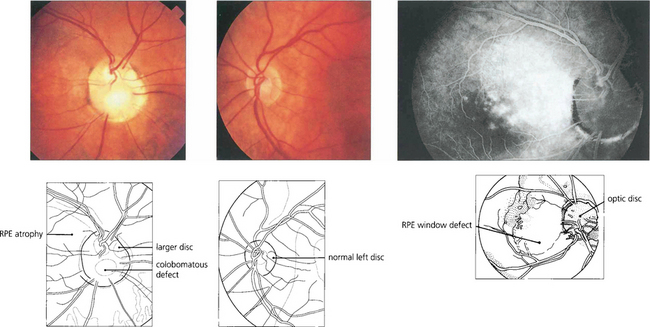
Fig. 17.12 Colobomas can be associated with serous macular detachments. This patient has an anomalous disc with a colobomatous area inferiorly associated with longstanding serous detachment of the macula with subsequent retinal pigment epithelial changes.
OPTIC DISC PITS
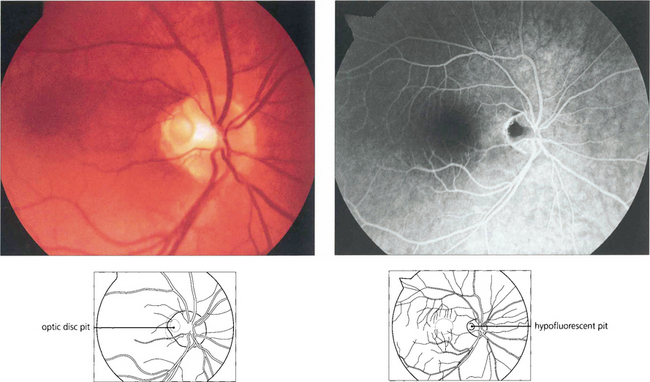
Fig. 17.14 (Left) A pit of the optic disc has a greyish appearance and lies in the temporal or inferior border of the disc (which is of normal or slightly larger diameter), penetrating deeply into its substance. Pits centred on the papillomacular bundle are frequently associated with a centrocaecal field defect; inferior pits produce superior arcuate field defects. Some patients, as in this example, have serous detachment of the macula and usually present with visual loss in early adulthood. (Right) A late-stage fluorescein angiogram shows hypofluorescence of the pit. The aetiology of macular detachment is thought to be transmission of fluid from the vitreous through the pit producing a retinal schisis.
OPTIC DISC HYPOPLASIA
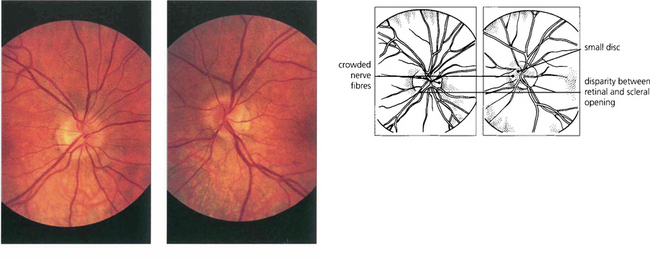
Fig. 17.15 This patient was referred with suspected papilloedema. Both optic discs are small, the left more so and slightly tilted, and the disparity between the retinal and scleral openings can be seen in both eyes. The right disc is small and full. There is crowding of the nerve fibres on the nasal side of each disc, simulating swelling.
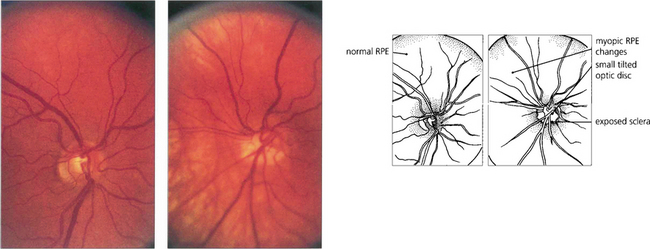
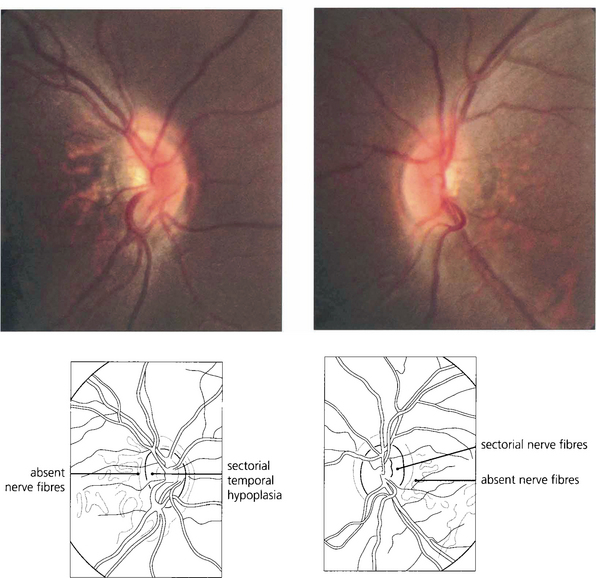
Fig. 17.16 Tilted discs are commonly seen in highly myopic eyes. This patient has a rather small disc in the right eye but the left eye is myopic with a tilted hypoplastic disc.

Fig. 17.17 The same patient had an associated cleft palate defect suggesting that the optic disc anomaly is part of a maldevelopment defect.
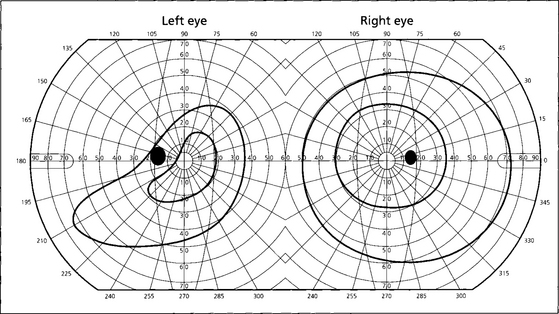
Fig. 17.18 These are the visual fields of the same patient. Fewer axons than normal enter the disc in the defective area and there is corresponding fundus ectasia (as shown by the thin retinal pigment epithelium in Fig. 17.16); together these features result in a visual field defect. As the defect is usually inferonasal this produces a superotemporal field defect simulating chiasmal compression. Such defects, however, cross the vertical meridian, a feature never seen with neurological causes of field loss. Furthermore, the refractive component can be corrected by additional myopic correction and these characteristics allow the correct diagnosis to be made.
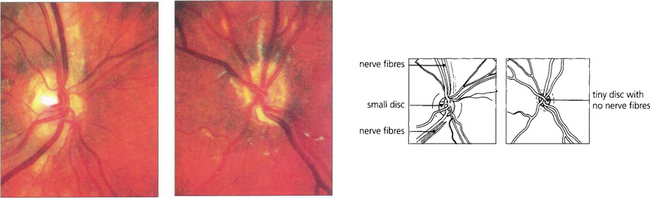
Fig. 17.19 Optic nerve hypoplasia is seen in its most severe form as part of the rare syndrome of septo-optic dysplasia. These children have very poor vision and associated midline intracranial anomalies, of which an absent septum pellucidum is typical. Abnormalities of pituitary hormonal function, especially growth hormone deficiency, are common. The right optic disc is grossly hypoplastic, although some nerve fibres are present; the left contains virtually no nerve fibres at all. This child had short stature as a result of growth hormone deficiency and acuity of 20/40 and PL.
By courtesy of Professor D Taylor.
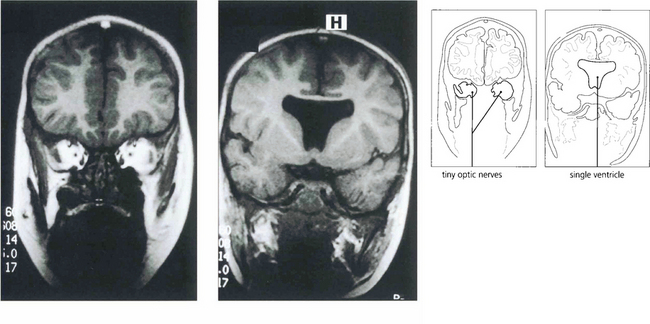
Fig. 17.20 Magnetic resonance image of another child shows tiny optic nerves in the orbit. The septum pellucidum is absent, resulting in a single lateral ventricle.
By courtesy of Dr R Hoare.
ANOMALIES ASSOCIATED WITH AXIAL LENGTH
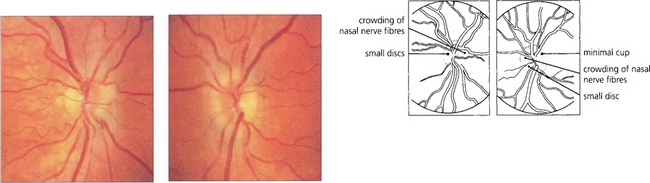
Fig. 17.22 The appearance of the optic discs in a patient with +6D of hypermetropia in each eye and axial lengths of 21 and 20.7 mm. The discs are small and full with a crowded nerve fibre pattern and minimal cupping.
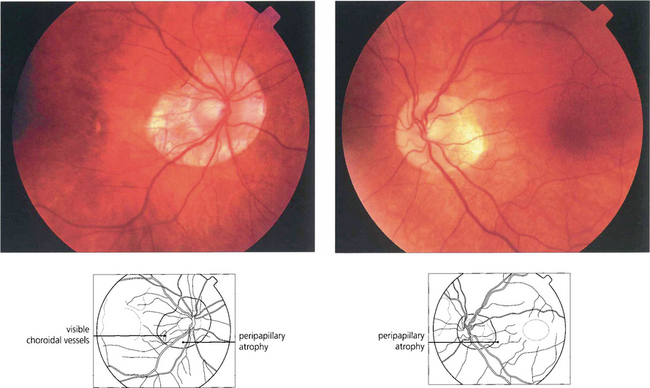
Fig. 17.23 Myopic discs have associated peripapillary atrophy and a temporal crescent. Because of the larger intraocular surface area, the retinal pigment epithelium and choroid appear to be thinned and pale and sometimes the temporal retinal vessels are stretched into a posterior pole staphyloma (see Ch. 15).
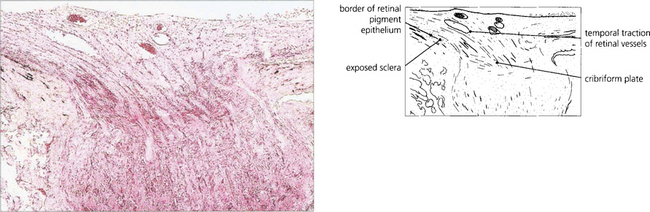
Fig. 17.24 Histological examination of a myopic disc shows that the retinal aperture of the optic disc is larger than the scleral aperture with a deficiency of retina and choroid on the temporal side revealing the bare sclera. There is temporal traction of the blood vessels caused by the stretching or pulling of the retina into the expanded posterior pole of the eye.



