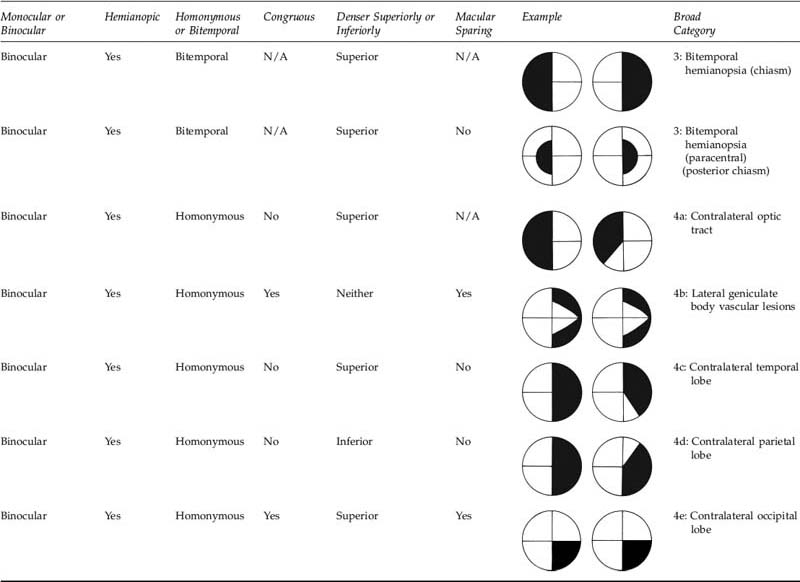
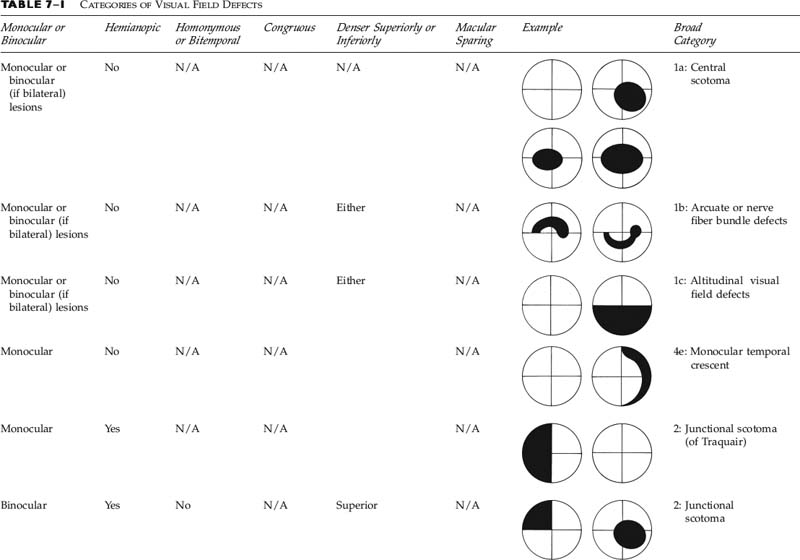
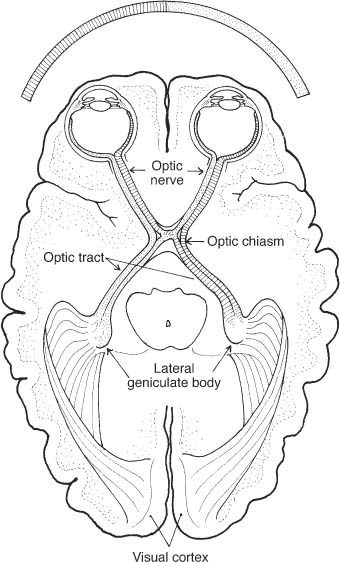
Chapter 7 This chapter can be used to localize visual field defects. Figure. 7–1 shows the topographical anatomy of the visual field correlated with the visual pathway. Before using the figure you should establish the following (Table 7–1): • Is the visual field defect monocular or binocular? • Monocular visual field defects are due to lesions of the ipsilateral retina or optic nerve, with the exception of the monocular temporal crescent (see below). • Binocular visual field defects may be due to bilateral retinal or optic nerve disease or may be chiasmal or retrochiasmal lesions. • Is the visual field defect a monocular temporal crescent? • If binocular, is it hemianopic or not? • Is this junctional visual field loss? • If it is hemianopic, is it bitemporal or homonymous? • Is this a lateral geniculate or optic tract lesion? • Are there other localizing signs present? • If hemianopic, is the field congruous or incongruous? • Is there macular sparing? • Is the field defect denser superiorly or inferiorly? • 50 degrees nasally • 60 degrees superiorly • 70 degrees inferiorly • 80 to 90 degrees temporally • Retinal nerve fiber layer • Optic nerve axons • Optic chiasm • Temporal fibers remain uncrossed in the optic chiasm. • Nasal fibers cross into the contralateral optic tract in chiasm. • Inferonasal fibers enter into the contralateral optic nerve for a short course before continuing on to the contralateral optic tract (Wilbrand’s knee). The knee may not exist anatomically (may be an artifact of fixation), but the finding of a junctional scotoma still has localizing value clinically. • Fibers from the optic tract travel to the lateral geniculate body. • Inferior fibers pass as optic radiations in the temporal lobe. • Superior fibers pass in the parietal lobe radiations. • Radiations reach the occipital lobe (calcarine cortex). • Anterior portion of the occipital lobe fibers represented monocularly as the temporal crescent. • Examiner’s hand or fingers presented in four quadrants. • Examiner’s own visual field serves as the control. • Colored test objects (red) may enhance sensitivity. FIGURE 7–1 Schematic diagram of the visual pathways and possible visual field defects. • Reasonable routine screening test • Testing of central field with the examiner’s face as the test object • Useful test of the central 20 degrees at 30 cm • Especially helpful in macular disease or small central or paracentral scotomas • Tests central 20 to 40 degrees • Helpful in patients who are unable to be tested by formal perimetry • Testing available at various distances (e.g., 1 m and 2 m) • Good test for detecting nonorganic “tunnel” fields (nonorganic field fails to expand appropriately with doubling of the test distance and test object size) • Various-sized test objects can be used. • Different colored test objects may enhance sensitivity (red). • Static or kinetic testing • Advantages and indications • Disadvantages • Advantages • Disadvantages
VISUAL FIELD DEFECTS
NORMAL VISUAL FIELD IN DEGREES METHODS OF TESTING THE VISUAL FIELDS (FIG. 7–2)
TOPOGRAPHIC ANATOMY OF THE VISUAL FIELD (FIG. 7–1)
METHODS OF TESTING THE VISUAL FIELDS
CONFRONTATION TESTING
AMSLER GRID
TANGENT SCREEN
GOLDMANN PERIMETRY
 Useful in unreliable computerized static testing
Useful in unreliable computerized static testing
 Helpful with very poor visual acuity (<20/200)
Helpful with very poor visual acuity (<20/200)
 Can detect peripheral islands of intact visual field
Can detect peripheral islands of intact visual field
 Good for testing for visual field defects in the extreme periphery
Good for testing for visual field defects in the extreme periphery
 Valuable in the evaluation of the shape visual field defects
Valuable in the evaluation of the shape visual field defects
 Technician dependent
Technician dependent
 Not as reliably reproducible as computerized perimetry
Not as reliably reproducible as computerized perimetry
 Time intensive
Time intensive
 Not universally available
Not universally available
AUTOMATED COMPUTERIZED PERIMETRY
 Reliable in patients able to reproducibly be tested
Reliable in patients able to reproducibly be tested
 Standardized data
Standardized data
 Reproducible method of documenting, quantifying, and following visual field defects (Fig. 7–3)
Reproducible method of documenting, quantifying, and following visual field defects (Fig. 7–3)
 Requires cooperative and alert patient
Requires cooperative and alert patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


