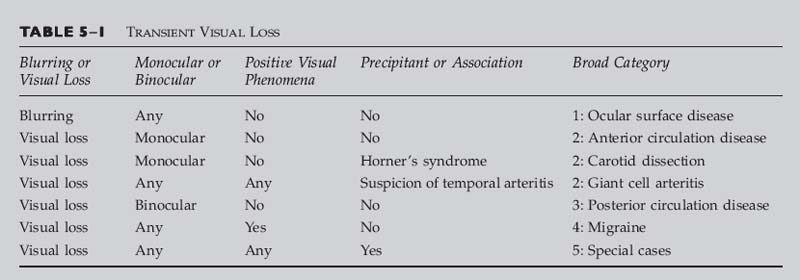
Chapter 5 This chapter discusses how to efficiently initiate a workup of a patient with transient visual loss by collecting key points in the history and examination. The major causes of transient visual loss are described, with attention to the characteristic signs and symptoms, as well as suggestions for further investigation. Many older patients with transient visual loss are eventually found to have either carotid artery or coronary disease as an underlying cause. In younger patients, vasospasm, occasionally associated with migraine, is a common cause. Other causes of transient vision loss include hypercoagulable states, vertebrobasilar insufficiency, and giant cell arteritis. One should attempt to determine if the visual loss was monocular or binocular, keeping in mind that the reports of patients are not always accurate; a homonymous hemianopic visual field loss may be interpreted by the patient as monocular visual loss on the side of the hemianopia. Monocular visual loss is referable to the eye and optic nerve and is termed transient monocular blindness or amaurosis fugax (“fleeting blindness”). Binocular visual loss implies a homonymous visual field loss and must be related to the visual pathways posterior to the optic chiasm. A history of hypertension, diabetes, cardiac disease, peripheral vascular disease, or smoking should increase one’s suspicion that the cause of the patient’s symptoms is vascular. A personal or family history of deep venous thrombosis, pulmonary embolism, or multiple miscarriages raises the possibility of a hypercoagulable state. Associated eye pain, brow ache, or headache may also direct the investigation. In addition to a complete eye examination and a neurologic examination, as appropriate, the following additional information should be gathered: Vital signs, looking for hypertension or an irregular pulse Auscultation of the heart for murmurs Auscultation of the carotid arteries for bruit Examination of the fingernail beds, looking for splinter hemorrhages (Fig. 5–1) Obtaining formal perimetry can be very helpful because patients may have a persistent defect in their vision that they are unaware of. When examining the retina, a careful search for emboli should also be undertaken. Patients with a visible plaque in the retinal vasculature have an increased rate of both mortality and stroke. However, most of these patients eventually die from cardiovascular disease, rather than stroke.1 The workup of a patient depends largely on the age of the patient and whether the patient’s symptoms are thought to be monocular or binocular. Use the flowcharts in this chapter as a guide to your evaluation. Table 5–1 is used for transient loss of vision. Before using this table, you should establish the following: It is important to distinguish between transient visual blurring and transient visual loss. Patients with transient blurring describe out-of-focus vision that lasts only a few seconds, and often clears with blinking, whereas patients with transient visual loss describe a complete loss of vision, a curtain coming down over their vision, a scotoma, an area of bluish or purple discoloration in their field of vision, or a loss of color perception or saturation. Their symptoms usually last minutes to hours. FIGURE 5–1 Splinter hemorrhages of the fingernails. Although classically associated with endocarditis, splinter hemorrhages of the fingernails have also been observed in patients with the hypercoagulable state associated with antiphospholipid antibodies. (Photograph courtesy of Dr. Kathleen B. Digre.) Determine if the visual loss was in one or both eyes. Remember that patients may confuse a homonymous hemianopic visual field loss with visual loss in the ipsilateral eye. For example, a right homonymous hemianopia may be misinterpreted as loss of vision in the right eye. Unless the patient actually covered each eye in turn, the history may not be accurate. Was the visual loss associated with scintillations or other positive phenomena? Determine if the visual loss was associated with a particular precipitating event or other symptom. Is there a Horner’s syndrome (suggests carotid dissection)? If the patient is over 60, are there any symptoms of temporal (giant cell) arteritis, or is there an elevated erythrocyte sedimentation rate or C-reactive protein? • A loss of sharpness to vision without darkening, graying, or change in brightness sense • The most common cause of blurring is dry eye. • Often worsened by concurrent blepharitis • Dry-eye patients often say that they can read for several minutes, but after that their vision blurs and they’re no longer able to read. • Symptoms resolve after several minutes, only to recur with attempted reading or other use. • An ocular foreign body sensation, itching, or burning may be present. • Anterior segment examination reveals dry eyes. • Relief with artificial tears is helpful in confirming diagnosis. Carotid artery disease can cause monocular visual loss when an embolus reaches the eye. The most common cause of retinal artery occlusion is embolization of an atheromatous carotid plaque.2 Nonatherosclerotic disease of the carotids, such as dissection (see later in this chapter), or fibromuscular dysplasia should also be considered, especially in younger patients. • Monocular loss of vision lasting up to 30 minutes • A Hollenhorst plaque or evidence of a branch retinal artery occlusion may be visible on ophthalmoscopy (Fig. 5–2). • In young patients, consider carotid dissection, especially if associated with Horner’s syndrome. Carotid dissection can cause monocular visual loss when an embolus forms at the distal end of the clotted artery and travels to the eye. • Monocular loss of vision lasting up to 30 minutes • Ipsilateral Horner’s syndrome • A Hollenhorst plaque or evidence of a branch retinal artery occlusion may be visible on ophthalmoscopy (Fig. 5–2). Although more common in middle-aged and elderly patients, cardiac disease may occur at any age. Symptoms depend on the site where the embolus (or emboli) eventually lodges. Monocular vision loss from cardiac disease is caused by embolus to the anterior circulation. • Monocular loss of vision lasting up to 30 minutes • There may be an embolus or subtle evidence of a branch retinal artery occlusion on ophthalmoscopy with a corresponding visual field defect (Figs. 5–3 and 5–4).
TRANSIENT VISUAL LOSS
KEY POINTS IN THE HISTORY
KEY POINTS IN THE EXAMINATION
BLURRING OR VISUAL LOSS

MONOCULAR OR BINOCULAR
POSITIVE VISUAL PHENOMENA
KNOWN PRECIPITANTS OR ASSOCIATIONS
BROAD CATEGORY 1: OCULAR SURFACE DISEASE
PRESENTATION AND RED FLAGS
Classic Presentation
Red Flags (All Suggestive of Other Categories of Disease)
 Darkening or other changes in vision
Darkening or other changes in vision
 Curtain or shade across vision
Curtain or shade across vision
 Hemianopic or quadrantanopic symptoms
Hemianopic or quadrantanopic symptoms
 Abnormal neuro-ophthalmic examination
Abnormal neuro-ophthalmic examination
BROAD CATEGORY 2: ANTERIOR CIRCULATION DISEASE
CAROTID ARTERY DISEASE
Classic Presentation
Red Flag
 Rarely, carotid artery disease can cause binocular (homonymous) visual loss when an embolus lodges in the brain (stroke). If the visual loss is binocular, consider other etiologies first, such as cardiac disease or vertebrobasilar insufficiency, discussed later.
Rarely, carotid artery disease can cause binocular (homonymous) visual loss when an embolus lodges in the brain (stroke). If the visual loss is binocular, consider other etiologies first, such as cardiac disease or vertebrobasilar insufficiency, discussed later.
CAROTID DISSECTION
Classic Presentation
CARDIAC DISEASE
Classic Presentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


