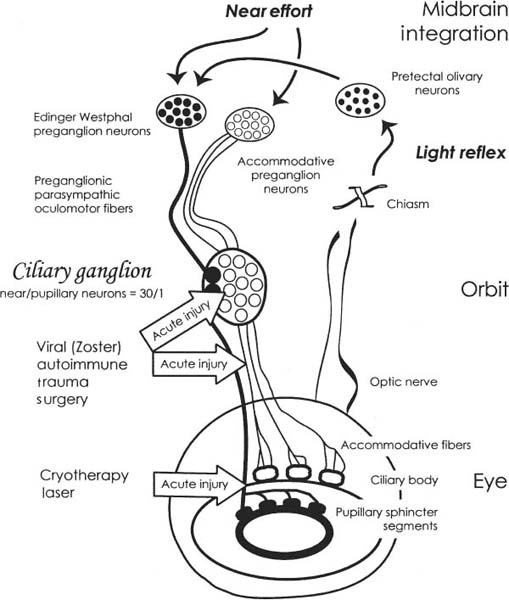
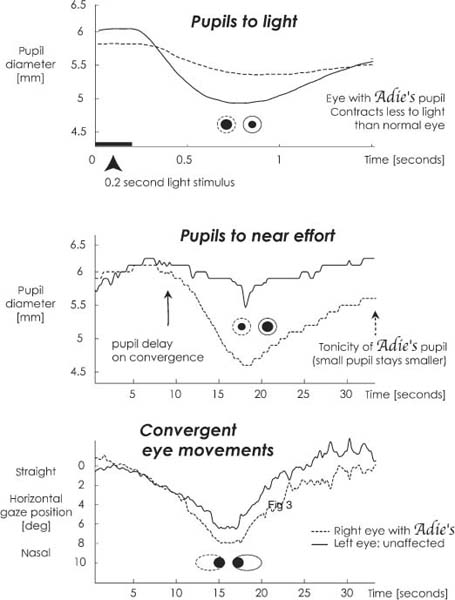
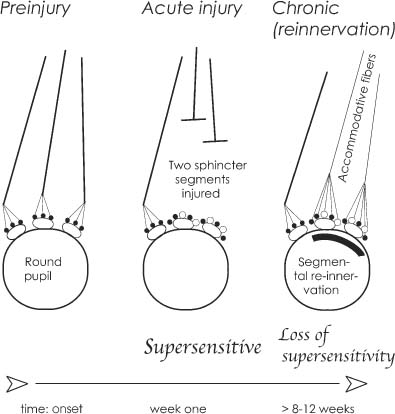
Chapter 37 Adie’s pupil is a common cause of anisocoria. It is an efferent pupil defect in which the light reaction of one or more iris sphincter segments is lost due to injury of the postganglionic parasympathetic nerves originating in the ciliary ganglion.1 The exact cause of the injury is usually not known, but in most cases it is benign. The pathologic process begins with an acute denervation of smooth muscle segments in both the iris sphincter and ciliary body, followed by reinnervation of the muscles by accommodative neurons over time. Acutely, there is loss of part or all of the pupil light reflex and decrease in accommodative function at near. Chronically, with regrowth of axons of accommodative neurons, focusing improves somewhat, but contraction of the pupil to light does not. The hallmark of an Adie’s pupil is the characteristic segmental palsy of the iris sphincter muscle observed using the high magnification of a slit lamp. This characteristic segmental nature of Adie’s pupil can be confirmed by observing that the unaffected clock-hour segments of the iris adjacent to the pupil border contract and “bunch up” with a sudden “turning up” of the illumination knob on the slit lamp. Adjacent, palsied segments do not move, however, or they are passively pulled toward adjacent working segments with bright illumination. Thus, with a bright, abrupt-onset illumination and with the magnification of a slit lamp, the normally innervated segments of the iris sphincter still contract in concert, but the intervening palsied segments do not contract to light and this gives the impression of what was once called a “vermiform” movement of the iris. Small segments of the iris sphincter have occasionally been seen to contract spontaneously.2 Pharmacologic testing during the acute stage of denervation with a dilute solution of a topical cholinergic agonist (e.g., 0.1% pilocarpine) given to both eyes demonstrates some cholinergic supersensitivity. Observation in darkness before and 30 minutes after topical 0.1% pilocarpine shows that the affected eye has a greater pupil contraction and often becomes the smaller of the two pupils due to the supersensitivity. The amount of supersensitivity varies with the number of muscle segments that have become denervated. This cholinergic supersensitivity may be present as soon as 4 to 5 days after the onset of acute denervation. Cholinergic supersensitivity may also diminish over time, as reinnervation of iris sphincter segments by accommodative neurons occurs over the following 2 to 4 months, as explained later (Fig. 37–1). Following acute injury there is usually some regrowth of axons from the postganglionic parasympathetic cell bodies in the ciliary ganglion that survive the injury. Normally, the cell bodies of accommodative neurons innervating the ciliary body outnumber the neurons innervating the iris sphincter muscle in a ratio of 30:1. This is due to the greater mass of smooth muscle in the ciliary body, and hence more neurons supplying it. Because of this, reinnervation of both the iris sphincter and ciliary muscle occurs after at least 8 weeks3 and is almost all due to regrowth of the accommodative axons. The reinnervation of the palsied iris sphincter segments by accommodative neurons over time is a form of aberrant regeneration and causes the reinnervated iris sphincter segments to now contract to a near effort, but the light reflex contraction does not recover. This phenomenon results in a characteristic light-near dissociation of the affected eye and should be considered a sign of a chronic Adie’s pupil. It is not present during the acute stage. Often the pupil may appear randomly to change size during the examination due to changes in the patient’s focus point, and hence state of accommodation (Fig. 37–2). When accommodative fibers densely reinnervate a large number of clock-hour segments of the iris sphincter, the muscle remains in a chronic state of contraction almost all of the time, resulting in a small “little old Adie’s pupil.” In this case, the pupil remains small, even in darkness, because the accommodative neurons do not show a reduction in discharge with a decrement of light (compared with light reflex fibers in a normally innervated iris sphincter). The pupil remains small in all lighting conditions, resulting in a “tonic” pupil. The tonic pupil contracts to an even smaller size with a good near effort by the patient. The normal pupil contracts to a near effort and promptly redilates with refixation on a distant target. The chronic Adie’s pupil remains in a state of tonic contraction after a near effort and only slowly dilates after refixation on a distant target (i.e., after 15–30 seconds), and even then the tonic pupil may not dilate fully, compared with the fellow eye. A similar dynamic of tonic muscle contraction to a near effort also occurs in the ciliary body. This causes unequal accommodation between the two eyes, especially when the patient who has been reading or working at a computer attempts to shift focus to a distant target (Fig. 37–3). FIGURE 37–1 The ciliary ganglion and/or the postganglionic fibers are damaged in Adie’s pupil. The postganglionic fibers are separate for pupil constriction and for accommodation. Input to the ciliary ganglion is from the pupillary light reflex and the near effort originating from the midbrain. There is no urgency for workup of a suspected Adie’s pupil, unless there is involvement of extraocular muscles or ptosis, in which case the possibility of a third nerve palsy should be excluded within 24 hours. Adie’s pupils are best evaluated by an ophthalmologist. FIGURE 37–2 Denervated and reinnervated pupillary segments in Adie’s pupil. Injury either to the ciliary ganglion or the postganglionic fibers causes an increased numbers of receptors (small open circles), which in turn causes cholinergic supersensitivity, taking about 1 week to establish. When reinnervation occurs, the increased number of receptors is occupied by axonal endings, and therefore, supersensitivity may diminish. Predominance of women and of the 20- to 40-year old age group, but also reported in children.4–6 Familial incidence can occur.7,8 Four to seven per 100,000 per year.9 The average incidence of second-eye involvement is ~4% per year during the first decade of the illness.10 The tendon reflexes tend to get worse during the time course of the disease. In 89% of 73 patients, the reflexes were diminished or absent.11 The patient, an acquaintance, or a doctor notices unequal pupils, but the patient is asymptomatic. 1. Acute: Difficulty with near vision: lack of accommodation, unequal accommodation, or induced cylinder at near. 2. Chronic: Difficulty adjusting to changes in accommodation (first working on a computer or reading, then looking off in distance and experiencing an unequal far point; the dynamics of accommodation are unequal between the affected and unaffected eye). Photophobia in bright light, glare symptoms during night driving (Table 37–1). The sequence of the exam and distinguishing features of Adie’s pupil are shown in Fig. 37–4 and summarized as follows: Demonstrate that the affected eye has an efferent pupil defect to light; the anisocoria in an acute Adie’s pupil should increase as the illumination is increased (the involved pupil doesn’t contract to the same extent as the fellow eye). In a chronic unilateral Adie’s pupil, the affected pupil may be the smaller pupil in dim light (“little old Adie’s pupil” or tonic pupil). In very bright light, you should always be able to demonstrate an anisocoria, with the affected pupil being the larger one as long as the patient doesn’t accommodate. Even with a little old Adie’s pupil, the unaffected pupil should still contract to a smaller size than the affected pupil, as long as the light used is bright enough (an inadequately bright light is a common error in exam). A confusing result on the pupil exam may be found in patients with a light-near dissociation occurring in chronic Adie’s pupil. The patient may inadvertently accommodate on the examiner’s face, causing the affected pupil momentarily to become small. Therefore, it is imperative that patients should relax their accommodation and stay focused on a distant target during the pupil exam; otherwise, accommodation-induced pupil contraction may confuse the results of the exam. If the patient is accommodating and the pupil becomes small, a light shined in the eye may produce paradoxical pupil dilation, due to an accommodative effort that is broken by the bright light shined into the eye. FIGURE 37–3 Pupillographic simultaneous recording of the right and left pupils of a patient with a chronic right Adie’s pupil. The top panel demonstrates that before the light stimulus the right pupil is a little smaller than the normal left pupil, and following a light stimulus, the contraction of the right pupil is impaired, causing it to be the larger of the two pupils during the contraction phase. The middle panel shows the right and left pupil contraction to a target coming closer to the patient, causing accommodation and a light-near dissociation, with the right pupil becoming smaller than the normal left pupil. The two eyes’ horizontal positions were also recorded at the same time, demonstrating binocular convergence (bottom panel). The tonicity of the near contraction of the right pupil is demonstrated in the middle panel at the end of the recording. Here there was still a sustained contraction of the right pupil compared with the fellow eye at a time when the convergence ended and the eyes diverged as the target was moved back toward the far point (at ~30 to 40 seconds). Under the magnification of a slit lamp, there should be one or more sphincter segments that contract normally to light and interspersed palsied segments that do not contract to light; these segments may move passively from the pulling of adjacent, contracting segments. The spared sphincter segment that is still normally innervated may represent a very small area along the pupil circumference, so it may be necessary to look carefully at each clock hour during the slit-lamp exam while turning the light off and on. Rarely, all segments may be affected.
ADIE’S PUPIL
URGENCY OF EVALUATION
DIAGNOSIS
DEMOGRAPHICS
Age and Sex Distribution
Genetics
Incidence
Natural History of Adie’s
Second-Eye Involvement
Tendon Reflexes
SYMPTOMS
Asymptomatic
Difficulty with Focusing
Photophobia
SIGNS
Abnormal Response to Light
Slit-Lamp Examination
Symptoms12 | Pupil related | 72% (88 of 122) of the patients complaint was anisocoria 10% (12 of 122) had photophobia 3% (4 of 122) had difficulties with dark-adaptation |
| Ciliary muscle related | Blurred vision was present on 33% (40 of 122) Tonicity of accommodation in 7% (8 of 122) Brow ache with near work in 5% (6 of 122) |
Light-Near Dissociation
Check for a pupil contraction to a near effort that exceeds the light response in the affected eye. This is termed a light-near dissociation (see sidebars: Recognizing Light-Near Dissociation and How to Test for a Pupillary Near Response). If a light-near dissociation is present, it is not an acute Adie’s pupil; rather, it is chronic and is showing aberrant regeneration of the iris sphincter by accommodative nerve fibers.
Normal Motility
Check eye motility and eyelid function to confirm that this is not an early sign of a pupil-involving oculomotor nerve palsy.
RECOGNIZING LIGHT-NEAR DISSOCIATION Sometimes, in a doubtful case, it is hard to know where to draw the line for a light-near dissociation. When is the near response clearly greater than the light reaction? When you face the patient, with pocket light in hand, there are usually three levels of light available to the examiner:
Darkness, with a light shining tangentially on the pupils from below Room light
Room light with an additional bright light in the eyes
With the patient looking in the distance, shine the bright light in the eye three or four times, each time for only 1 or 2 seconds. This tells you how small the pupils will go with just a brief, bright light stimulus. Never judge the near response by adding a near stimulus to a bright light stimulus; this almost always produces an apparent light-near dissociation because the near stimulus inevitably adds something to the light stimulus. A real light-near dissociation is present only if the near response (tested in moderate light) exceeds the best constriction that bright light can produce.
HOW TO TEST FOR A PUPILLARY NEAR RESPONSE The pupillary near reaction is usually weak when tested in dim light or in the dark. The patient needs to see what he is looking at before trying to get it into focus. Do not try to induce a near response at the slit lamp unless you need the magnification to see segmental contractions of the iris sphincter; the room is usually dark and there is too much equipment in the patient’s face. The near response should be looked for in moderate room light so that the patient’s pupils are mid-sized, and the near object is clearly visible.
Give the patient an accommodative target to look at —something of interest or with fine detail on it. Sometimes a better response is obtained if an auditory sensory input is added to the stimulus, such as a ticking watch or clicking fingernails. Alternatively, something proprioceptive can help generate a good near response, like the patient’s own thumbnail, which can be held up in front of him, perhaps, in the case of a child, with a little face drawn on it.
Watch for convergence to help you judge how hard the patient is trying. Remember that the near response, although it may be triggered by blurred or disparate imagery, has a large volitional component, and the patient may need encouragement and perhaps a few practice runs (“There, you’re getting the hang of it; try it one more time”). Often on the third or fourth try he will do a good one. When you do not get a near response, it is usually because the patient (or the doctor) has not been trying hard enough.
A patient who is completely blind and has no pupillary reaction to light still sometimes does a good near response if you ask him to “cross your eyes like you did when you were a child.” If you cannot get a patient to do a near response, try the “lid closure reflex”: ask the patient to look at you and squeeze his eyes shut while you try, with both hands, to hold one of them open. This often produces a surprisingly strong near response. This is called the “eye-closure pupil reaction.”
Accommodation
Check the near point of accommodation for each eye with patients wearing their best distant eyeglass correction. This is measured in each eye separately by finding the shortest distance at which patients can still discriminate a small letter equivalent in size (visual angle subtended) to their best corrected distant acuity. In a young person with an acute Adie’s pupil, the accommodative amplitude is decreased in the affected eye, causing the near point to be located further away compared with the other eye. In a chronic Adie’s pupil, the reinnervation of the ciliary body with accommodative fibers may not only restore the near point but also shift it closer than the unaffected eye (Table 37–2).
OTHER ABNORMALITIES
Reflexes
Deep tendon reflexes (biceps, triceps, knee jerk, ankle jerk) are commonly decreased. However, they are normal in the nonidiopathic causes of Adie’s pupil (Fig. 37–5).
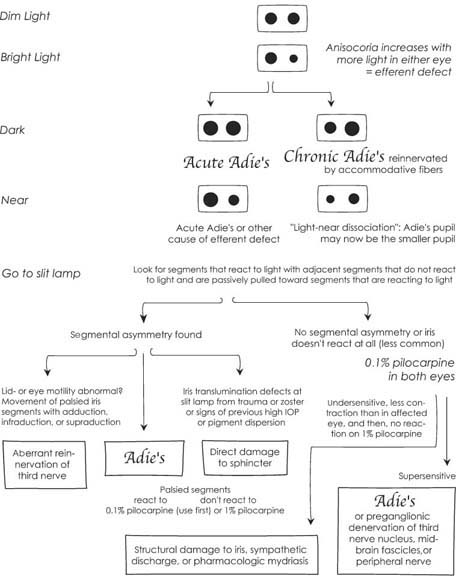
FIGURE 37–4 Flow sheet on how to perform an examination on a patient with an Adie’s pupil, compared with other causes of pupil efferent defect.
Signs | Acute | Chronic |
|---|---|---|
Photophobic | + + | +/− |
Blurring at near | + + + | − |
Abnormal dynamics of focusing | + | + + + |
Findings |
|
|
Segmental loss of light reflex | + + + | + + + |
Contraction segments to near that are paretic to light | − | + + + |
Accommodative amplitude to near target | Decreased | Normal (delayed) or increased |
Corneal sensation | Decreased/normal | Decreased/normal |
Tendon reflexes | −/Normal | −/Normal |
Vibratory sensation | −/Normal | −/Normal |
Vibration Sense
Vibratory sensation is also commonly decreased in the idiopathic form of Adie’s, although the muscle spindles are not affected.13 Ulrich14 has shown that the basic mechanism for explaining the tonic pupil and areflexia lies in a degeneration of neurons of the ciliary and spinal ganglia. If there are areas of skin lacking in sweating and other areas that are hyperhidrotic, then Ross syndrome should be suspected (see Appendix). Corneal sensation may also be decreased in some clock-hour areas of the cornea and is thought to represent involvement of trigeminal afferent fibers as they pass through the ciliary ganglion or short ciliary nerve.
RED FLAGS
The following features should raise the question of alternate diagnoses:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


