Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

2

Visual Assessment
Vision testing in children is often the most challenging part of a comprehensive eye examination. Assessing the visual acuity of infants and young children is an art. The detection of physical abnormalities is only a clue to visual function. Obtaining a quantitative or qualitative assessment of visual function requires a skill that is developed utilizing a repertoire of techniques.1,2 Until the age of 5 or 6 years, the assessment of vision is frequently dependent on the examiner’s clinical judgment and expertise.
In this chapter, we address the art of vision testing and describe approaches to assessing the visual function of infants, preliterate children, and developmentally delayed older children.
 General Principles
General Principles
The examination should begin as a child he enters the exam room. This may be your best opportunity to evaluate vision. Be alert to visual attentiveness of a child. Specifically, be aware of head position, nystagmus, photophobia, or strabismus. Establishing a good rapport with a child is key to obtaining cooperation for subsequent testing. Incorporate the establishment of rapport with the actual examination; make the exam fun. For example, while showing the child a small toy, the examiner can be evaluating fixation patterns (Fig. 2-1). Leading the child into a conversation about the toy establishes the dialogue needed for a later objective vision test. Conversation centered around a toy not only helps to relax the child but also provides an opportunity to evaluate the cooperativeness and developmental level of the child. This knowledge will help direct you toward the appropriate method of visual assessment.
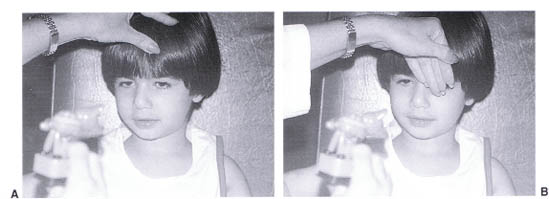
FIGURE 2-1. Child fixates on a small toy while the examiner evaluates fixation preferences. A cover, uncover test is being performed.
Choose the appropriate method of testing based on the level of cooperation and on the developmental rather than chronological age. It is common to encounter bright 3- and 4-year-olds who are prepared to read Snellen letters. However, one also must be alert to developmentally delayed 6- and 7-year-olds who require pre-literate testing methods. It is important to emphasize that the child’s developmental age will determine which tests will be most appropriate.
 Neonates
Neonates
Assessing the visual function of the neonate or very young infant is often limited by the lack of attention by the patient or by lack of patience by the examiner. In the first few weeks of life, an infant sleeps frequently, and it can be difficult to sufficiently arouse her for vision testing. In the most unarousable infant, pupillary responses may be the only measure of visual function available. Multiple visits may be necessary. It can be helpful to see the child when he or she is hungry and is more likely to be alert. Do not confuse a somnolent recently fed baby with one who is neurologically delayed.
The alert neonate with normal visual functions should respond to lights and to faces. The infant’s gaze should fixate on and follow the face of the examiner as the examiner moves in various directions, positioned rather closely to the face of the infant (recorded as Fix and Follow Face). Some infants will also look at the direction of a light source but will not follow the movement of the light source (recorded as Fix, No Follow Light). When no fixation or following movements can be elicited, room lights can be turned on and off. A consistent reaction to the change in room illumination is a gross measure of visual response (recorded as Responds to Room Lights). Avoidance reactions to light of the indirect ophthalmoscope are also useful (recorded as Avoids Bright Light). Observations from home by parents can be an adjunct to the clinician’s observations. Question the parents regarding the infant’s responses to faces and lights. Be careful to eliminate voice recognition. In this age group do not assume that a lack of response is due to inability to cooperate. Most children choose to participate in the examination—even neonates.
Electrophysiological testing or preferential looking testing can be utilized when a quantitative value is necessary. These tests are generally more useful when the infant reaches an age when he or she is more alert. Visual evoked potentials (VEPs) and electroretinograms (ERGs) will be discussed in more detail in Chapter 21. Theoretically, these tests can be performed at any age. However, in neonates these tests can often suggest misleadingly poor visual function. The results, particularly of VEP testing, should, in such cases, be interpreted with caution. An examiner’s judgment often is the most useful test.
There are a number of available tests utilizing a preferential looking technique. These are based on the principle that an infant will “preferentially” look toward a pattern. The patterns are most often gratings or checks. A card is presented to the infant with a pattern on one side of the center and a gray field on the other. The Teller acuity cards, for example, are a series of cards with variously sized gratings. By determining the finest grating to which the infant will consistently direct his or her gaze, acuity can be extrapolated relatively accurately (Fig. 2-2).
Such tests can be administered in any clinical setting by an ophthalmic assistant with minimal training. They serve as a quantitative vision test for patients of all developmental ages and have, in fact, been utilized for vision testing of premature infants shortly after birth in studies of retinopathy of prematurity. These tests, however, have limitations with respect to interpretation and decreased sensitivity to amblyopia.
The recording of neonatal acuity is often descriptive in nature, although preferential looking and VEP results are recorded in cycles/degree, which allows for translation to Snellen acuity. Acuity might otherwise be recorded as “follows faces,” “responds to light,” “avoids bright light,” or “no fixation or following.” Normal neonatal acuity is gross and difficult to quantitate.
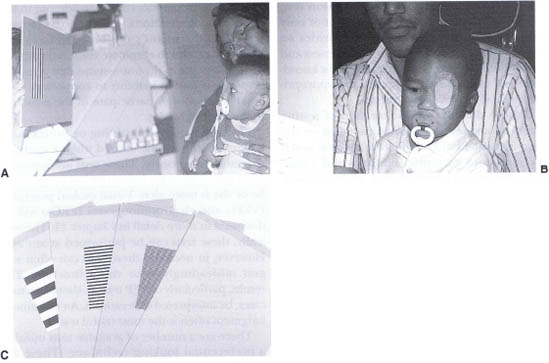
FIGURE 2-2. (A) A child with one eye patched views a Teller Acuity Card while the examiner evaluates the infant’s visual preference for the right or left side of the card. If the child prefers viewing the side of the card with the stripes, the infant is judged to have resolution acuity based on the stripe width. (B) A child with horizontal nystagmus can be tested with the cards held vertically. (C) A display of some of the Teller Acuity Cards showing the range of stripe width.
The visual acuity of a neonate is most often inferred by the physical exam and gross response to light and faces. For instance, if a baby is not responding to your face, your conclusion will vary depending upon whether a lens opacity or significant pathology is present. With a large central opacity, for example, the lack of response would be corroborative. In the absence of an opacity, the lack of response would be perplexing, and an explanation would be necessary.
Assessment of acuity is dependent more upon physical findings and upon evidence of potential abnormalities that could be caused by central nervous system defects or other medical problems. A careful birth and family history should be obtained, and an appropriate follow-up plan to assure optimal visual development is recommended. Fortunately, infants develop at a rapid rate, allowing more detailed assessment to be obtained as described in the following section of this chapter.
 Infants
Infants
At a few months of age an infant is more consistently responsive on a visual and sensory basis. A few classes of convention are used in the assessment. One convention is fixation behavior, as described above. Another, central-steady-maintained, which incorporates fixation preference, is often recorded as CSM.
| CSM Classification | |
|---|---|
| C = Central | Is the visual axis central in each eye, in contrast with eccentric (recorded as nC) fixation? If so, the macula is fixating. |
| S = Steady | Is the monocular fixation without movement, or does the eye wander? Is the globe bobbing up and down or back and forth as in nystagmus? If not steady (recorded as nS), the type of movement must be described. In nystagmus the fixation can often be steady at the null point but not elsewhere. |
| M = Maintained | Can the fixation be maintained with each eye individually under binocular viewing? In strabismus, the amblyopic eye may not maintain fixation under binocular conditions, and the patient will preferentially fixate with the dominant or sound eye. In a neurologically impaired child maintenance of fixation due to a lack of vision versus central neurological suppression (seizures) must be sorted out. |
Determining whether fixation is central and steady tests each eye individually (monocular testing), whereas determining whether fixation is maintained compares the vision of each eye (a binocular test). The evaluation of fixation maintenance (M) allows for better assessment of relative visual acuity and therefore more sensitive detection of amblyopia.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


